Cephalosporin Composition, action, dosage, route, indications, contraindications, Drug interactions, side effects, adverse effects, toxicity and role of nurse
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a comprehensive response. Here is the complete reference guide:
Cephalosporins - Complete Pharmacology Reference
1. Composition / Chemical Structure
Cephalosporins are semisynthetic β-lactam antibiotics derived from 7-aminocephalosporanic acid (7-ACA). Their nucleus consists of:
- A β-lactam ring fused to a dihydrothiazine ring (6-membered, unlike penicillin's 5-membered thiazolidine ring)
- R² side chain at the 7-position - determines antibacterial activity and spectrum
- R¹ side chain at the 3-position - modifies pharmacokinetic properties
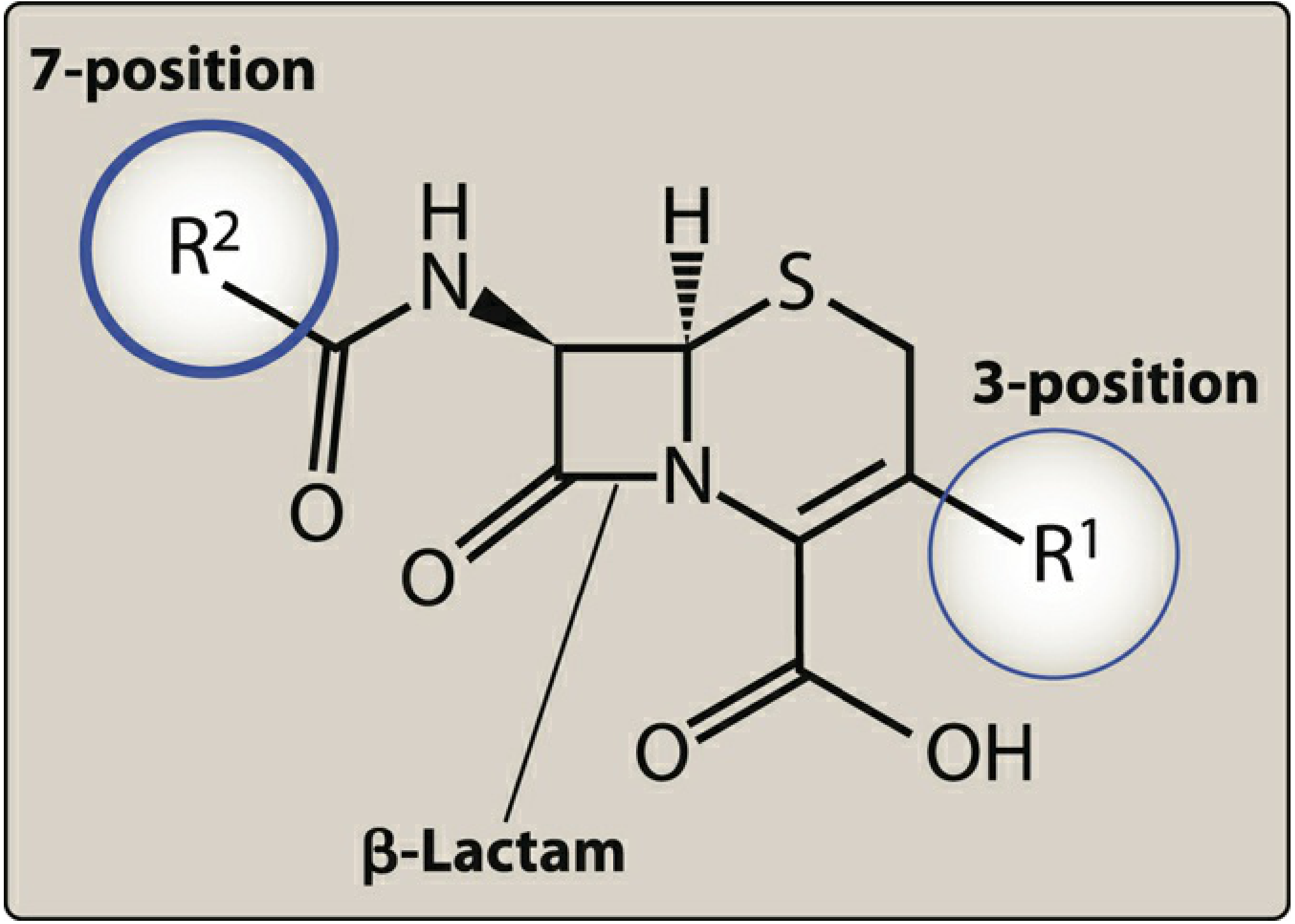
Figure: Structural features of cephalosporin antibiotics - Lippincott Illustrated Reviews Pharmacology
They tend to be more stable than penicillins to certain β-lactamases due to modifications in this core structure.
2. Mechanism of Action
Cephalosporins share the same mode of action as penicillins:
- They are bactericidal and time-dependent agents (bacterial killing is maximized when drug concentrations remain above the Minimum Inhibitory Concentration [MIC] for the greatest proportion of the dosing interval)
- They inhibit bacterial cell wall synthesis by binding to Penicillin-Binding Proteins (PBPs) - enzymes responsible for cross-linking peptidoglycan chains
- Binding to PBPs prevents transpeptidation (the final cross-linking step of peptidoglycan), weakening the cell wall and causing osmotic lysis
- They are affected by the same resistance mechanisms as penicillins (β-lactamase hydrolysis, reduced PBP affinity)
Clinical implication: IV β-lactams are often infused over 3-4 hours (extended infusion) or continuously over 24 hours to maintain concentrations above the MIC for longer periods, maximizing bacterial killing. - Lippincott Illustrated Reviews Pharmacology
3. Generations, Examples, and Spectrum
Cephalosporins are classified into 5 generations based on antibacterial spectrum and β-lactamase resistance:
| Generation | Key Drugs | Spectrum |
|---|---|---|
| 1st | Cefazolin (IV/IM), Cephalexin (oral), Cefadroxil (oral) | Gram (+) cocci: S. aureus, S. epidermidis, S. pneumoniae, S. pyogenes; Limited gram (-): E. coli, K. pneumoniae, P. mirabilis |
| 2nd | Cefuroxime, Cefaclor, Cefoxitin, Cefotetan | Broader gram (-) including H. influenzae, Neisseria gonorrhoeae, Enterobacter aerogenes; Some anaerobes |
| 3rd | Ceftriaxone, Cefotaxime, Ceftazidime, Cefdinir, Cefixime | Expanded gram (-) spectrum; Ceftazidime covers P. aeruginosa; Achieves therapeutic CSF levels (meningitis treatment) |
| 4th | Cefepime | Broad gram (+) and gram (-) including P. aeruginosa, AmpC-producing Enterobacter spp. |
| Advanced/5th | Ceftaroline, Cefiderocol | Ceftaroline: only β-lactam with MRSA activity; Cefiderocol: novel siderophore mechanism, active against multidrug-resistant gram (-) including KPC and MBL producers |
Note: All commercially available cephalosporins are ineffective against L. monocytogenes, C. difficile, and Enterococcus spp.
4. Dosage and Route of Administration
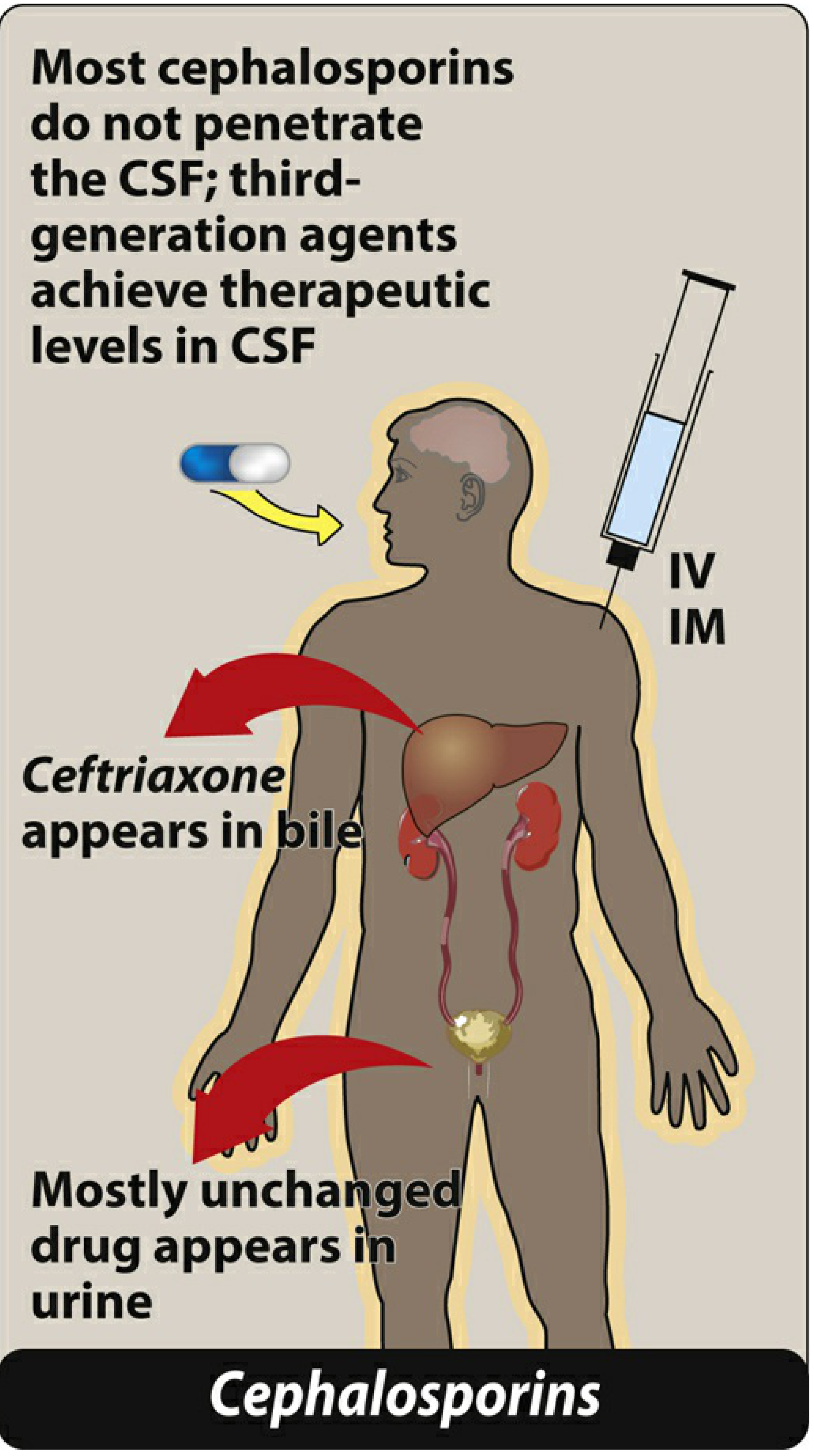
Figure: Cephalosporin administration routes and pharmacokinetic distribution - Lippincott Illustrated Reviews Pharmacology
Routes: Oral, IV, IM (most parenterally administered due to poor oral absorption; exceptions are first-generation oral agents and some 2nd/3rd generation oral formulations)
| Drug | Route | Usual Dose | Frequency |
|---|---|---|---|
| Cefazolin | IV / IM | 1-2 g | Q8h |
| Cephalexin | Oral | 250-500 mg | Q6h |
| Cefuroxime axetil | Oral | 250-500 mg | Q12h |
| Ceftriaxone | IV / IM | 1-2 g | Q12-24h |
| Cefotaxime | IV / IM | 1-2 g | Q6-8h |
| Ceftazidime | IV / IM | 1-2 g | Q8h |
| Cefepime | IV / IM | 1-2 g | Q8-12h |
| Ceftaroline | IV | 600 mg | Q12h |
Dose adjustment is required in renal impairment for most cephalosporins (excreted unchanged in urine). Cefiderocol notably requires adjustment for augmented renal clearance (may need Q6h dosing).
5. Pharmacokinetics
- Absorption: Most oral agents are well absorbed; most IV/IM agents have poor oral bioavailability
- Distribution: Widely distributed to tissues, pleural fluid, and joint fluid. Most do not penetrate CSF - exception: third-generation agents (ceftriaxone, cefotaxime) achieve therapeutic CSF levels
- Metabolism: Minimal hepatic metabolism; mostly excreted unchanged
- Excretion: Primarily renal (glomerular filtration + tubular secretion). Exception: Ceftriaxone is significantly excreted in bile (can cause biliary sludging)
- Probenecid blocks tubular secretion, increasing and prolonging cephalosporin blood levels
6. Indications
Surgical Prophylaxis
- Cefazolin (1st gen) is the gold-standard for most surgical prophylaxis (cardiac, orthopedic, abdominal procedures)
Infections
| Condition | Agent of Choice |
|---|---|
| Skin and soft tissue infections | Cephalexin (oral), Cefazolin (IV) |
| Community-acquired pneumonia | Ceftriaxone ± azithromycin |
| Bacterial meningitis | Ceftriaxone or cefotaxime |
| Urinary tract infections | Cephalexin, Ceftriaxone |
| Gonorrhea | Ceftriaxone (IM, single dose) |
| Hospital-acquired / VAP pneumonia | Cefepime, Ceftazidime |
| MRSA infections | Ceftaroline (only cephalosporin with MRSA activity) |
| Complicated UTI / hospital-acquired pneumonia (MDR gram-negatives) | Cefiderocol |
| Spontaneous bacterial peritonitis (SBP) | Cefotaxime or ceftriaxone (coverage ~95% of causative organisms) |
| Open fractures (Type III) | Cefazolin ± aminoglycoside; 3rd gen cephalosporin for gram-negative coverage |
| Intra-abdominal / surgical infections | Cefoxitin (2nd gen, with anaerobic coverage) |
7. Contraindications
- Known hypersensitivity to cephalosporins - absolute contraindication
- Known hypersensitivity to penicillin - use with caution (cross-reactivity ~3-5%, highest between penicillin and 1st-generation cephalosporins; determined by side chain similarity, not the β-lactam ring itself)
- Patients with Stevens-Johnson syndrome or toxic epidermal necrolysis from penicillins should NOT receive cephalosporins
- Patients with a negative penicillin skin test have no greater risk of cephalosporin reaction than the general population
- Caution in severe renal impairment (dose adjustment required)
Source: Fitzpatrick's Dermatology; Lippincott Illustrated Reviews Pharmacology
8. Drug Interactions
| Interaction | Effect | Clinical Action |
|---|---|---|
| Probenecid | Blocks renal tubular secretion → increased and prolonged cephalosporin levels | Monitor for toxicity; can be used therapeutically |
| Warfarin + cefotetan, cefamandole, cefoperazone, cefixime, cefaclor | Altered anticoagulant effect (hypoprothrombinemia) | Monitor INR closely |
| Cyclosporine + ceftriaxone or ceftazidime | Increased cyclosporine levels → nephrotoxicity risk | Monitor cyclosporine levels and renal function |
| Antacids and iron salts + cefdinir | Reduced oral absorption of cefdinir | Administer cefdinir 2 hours before or after antacids/iron |
| Aminoglycosides (concurrent use) | Additive nephrotoxicity (especially with older cephalosporins) | Monitor BUN and serum creatinine |
| Alcohol + cefotetan, cefamandole, cefoperazone | Disulfiram-like reaction (flushing, tachycardia, nausea) due to N-methylthiotetrazole side chain | Counsel patients to avoid alcohol during and 72 hours after treatment |
| First + fourth generation combination | Same-class combination not recommended for gram-positive coverage | Substitute vancomycin or clindamycin instead |
9. Side Effects and Adverse Effects
Common Side Effects
- GI disturbances: Nausea, vomiting, diarrhea (more common with oral agents and broad-spectrum agents)
- Injection site reactions: Pain, phlebitis at IV site
- Diarrhea / Pseudomembranous colitis: Disruption of normal intestinal flora; C. difficile-associated colitis possible with all cephalosporins
Allergic / Hypersensitivity Reactions
- Urticaria, rash, pruritus (most common)
- Serum sickness-like reactions
- Anaphylaxis (rare but life-threatening)
- Cross-reactivity with penicillin allergy (~3-5%)
Hematologic Effects
- Thrombocytopenia, neutropenia, eosinophilia
- Hypoprothrombinemia (with cephalosporins containing N-methylthiotetrazole side chains: cefotetan, cefoperazone) - can prolong PT/INR
- Coombs-positive hemolytic anemia (rare)
Renal
- Nephrotoxicity (uncommon at standard doses; potentiated by concurrent aminoglycoside use)
- Acute interstitial nephritis (rare)
Neurological
- Seizures (rare, with very high doses or in patients with renal failure/CNS disease)
- Cefepime-associated encephalopathy - confusion, myoclonus, nonconvulsive status epilepticus, especially in renal impairment if dose is not adjusted
Biliary
- Biliary pseudolithiasis (biliary sludge): Seen particularly with ceftriaxone, especially in children - ceftriaxone precipitates as an insoluble calcium salt in bile
10. Toxicity
| Type | Details |
|---|---|
| Nephrotoxicity | Additive with aminoglycosides; uncommon alone; monitor BUN/creatinine |
| Neurotoxicity / Seizures | High doses, renal failure; cefepime most associated |
| Hepatotoxicity | Rare transient elevation of liver enzymes |
| Hypoprothrombinemia | MTT side-chain cephalosporins (cefotetan, cefoperazone) inhibit vitamin K metabolism |
| Disulfiram-like toxicity | Alcohol + MTT side-chain cephalosporins |
| Biliary sludge | Ceftriaxone precipitation in gallbladder (especially pediatrics, high doses) |
11. Role of the Nurse
Pre-Administration
- Allergy assessment: Always inquire about penicillin AND cephalosporin allergy before administration; document the type of reaction (anaphylaxis vs. rash)
- Baseline assessments: Obtain baseline renal function (BUN, serum creatinine), complete blood count, and LFTs for prolonged therapy
- Culture collection: Ensure culture and sensitivity specimens are collected before the first dose
- Reconstitution and compatibility: Verify correct reconstitution technique, concentration, and IV compatibility (avoid calcium-containing solutions with ceftriaxone, particularly in neonates)
- Dose verification: Confirm dose is appropriate for the patient's weight, age, and renal function
During Administration
- Infusion rate: Administer IV over 30-60 minutes (standard); use extended infusion over 3-4 hours when ordered for time-dependent optimization
- Monitor IV site: Observe for phlebitis, extravasation, redness, or pain; rotate sites
- Monitor for allergic reaction: Especially during the first 30 minutes - watch for urticaria, pruritus, wheezing, hypotension; have resuscitation equipment ready
- IM injections: Administer deep into a large muscle (e.g., gluteus); warn patient about pain at injection site
Post-Administration Monitoring
- Therapeutic response: Monitor WBC trends, temperature curves, clinical signs of infection improvement
- Renal function: Monitor urine output, BUN, and creatinine, especially with aminoglycoside co-administration
- Coagulation: Monitor PT/INR in patients on warfarin or receiving MTT-containing cephalosporins
- Superinfection: Watch for signs of C. difficile-associated diarrhea (watery/bloody stools), oral candidiasis, or vaginal candidiasis
- Cefepime neurotoxicity watch: Report confusion, myoclonus, or altered consciousness, particularly in renal impairment
Patient and Family Education
- Oral agents: Take the full prescribed course even if feeling better; take with food if GI upset occurs
- Iron/antacids: Separate cefdinir from iron supplements and antacids by at least 2 hours
- Alcohol avoidance: Counsel patients on cefotetan or cefoperazone to avoid alcohol during therapy and for 72 hours after the last dose
- Report symptoms: Advise immediate reporting of rash, difficulty breathing, severe diarrhea, yellowing of skin/eyes, or unusual bleeding
- Breast-feeding/pregnancy: Inform the prescriber; cephalosporins are generally considered safe in pregnancy (Category B) but documentation is required
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Chapter 29 (β-Lactam Antibiotics / Cephalosporins)
- Fitzpatrick's Dermatology, Contraindications and Precautions of Cephalosporin Therapy
- Red Book 2021: Report of the Committee on Infectious Diseases, Cephalosporin Cross-Reactivity
- Campbell's Operative Orthopaedics, 15th Ed, Antibiotic Treatment and Open Fracture Management
- The Washington Manual of Medical Therapeutics, Cefepime dosing
This is a shared conversation. Sign in to Orris to start your own chat.