Ascites
Reading File
Finding Sources
Searching PubMed
ascites management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Ascites
Ascites is the pathological accumulation of fluid within the peritoneal cavity. It is one of the most common complications of cirrhosis and carries significant prognostic implications.
Epidemiology & Prognosis
-
Cirrhosis accounts for 84% of all ascites cases
-
Cardiac ascites, peritoneal carcinomatosis, and "mixed" ascites account for 10-15%
-
~80% of ascites is non-malignant; only ~10% is due to malignancy
-
Of malignant ascites, 80% arises from epithelial cancers (colon, gastric, pancreatic, ovarian, breast, endometrial)
-
Median survival: 2 years (non-malignant) vs. 4 months (malignant)
-
Harrison's Principles of Internal Medicine, 22E
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Pathophysiology
In Cirrhosis (Portal Hypertension Mechanism)
The mechanism involves three interrelated processes:
1. Increased Intrahepatic Resistance
- Hepatic fibrosis disrupts sinusoidal architecture
- Activated hepatic stellate cells cause smooth-muscle contraction
- Decreased eNOS leads to reduced nitric oxide and increased intrahepatic vasoconstriction
2. Splanchnic Vasodilation
- Paradoxically, cirrhosis increases systemic nitric oxide, VEGF, and TNF, causing splanchnic arterial vasodilation
- Blood pools in the splanchnic circulation, decreasing effective circulating volume
- Kidneys perceive this as hypovolemia
3. Renal Sodium and Water Retention
- Compensatory ADH release causes free water retention
- Activation of the sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system (RAAS) leads to renal Na+ and H2O retention
- This is the "peripheral arterial vasodilation hypothesis"
Systemic Inflammation: Decompensated cirrhosis also features bacterial translocation from the gut (PAMPs and DAMPs), which activates innate immune cells, releasing proinflammatory cytokines (IL-6, IL-8, TNF-α), further worsening circulatory dysfunction.
- Harrison's Principles of Internal Medicine, 22E
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
In Non-Cirrhotic States
| Mechanism | Example |
|---|---|
| Protein-rich exudation + lymphatic blockage | Peritoneal carcinomatosis, tuberculous peritonitis |
| Increased capillary pressure (systemic) | Heart failure, constrictive pericarditis, IVC obstruction |
| Increased capillary pressure (portal) | Budd-Chiari syndrome, portal vein thrombosis |
| Hypoalbuminemia | Nephrotic syndrome, protein-losing enteropathy, malnutrition |
| Pancreatic enzyme leakage | Pancreatic ascites |
| Lymphatic impairment | Chylous ascites |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Grading (International Club of Ascites)
| Grade | Definition |
|---|---|
| Grade 1 | Mild - detectable only by ultrasound |
| Grade 2 | Moderate - detectable by clinical examination |
| Grade 3 | Large - marked abdominal distention |
Refractory ascites = recurs ≥3 times within one year despite appropriate treatment.
Clinical Features
- Abdominal distension, discomfort, early satiety
- Shifting dullness and fluid thrill on examination
- Respiratory compromise when tense
- Signs of underlying cause: jaundice, spider angiomata, caput medusae (portosystemic shunt via umbilical vein), palmar erythema (cirrhosis); raised JVP, S3 gallop (cardiac)
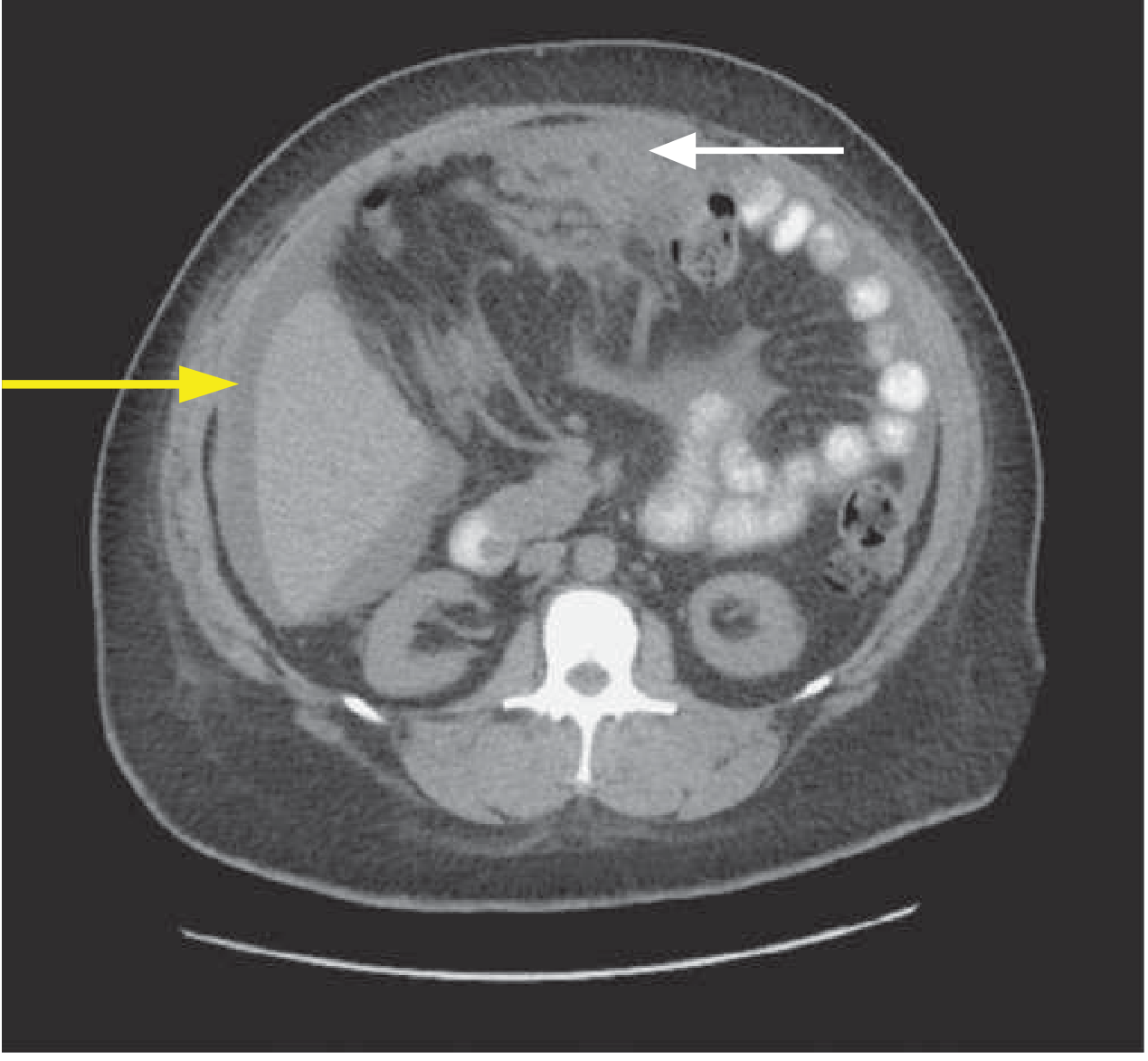
CT scan of peritoneal carcinomatosis (white arrow) with ascites (yellow arrow):
Diagnosis
Diagnostic Paracentesis - Always Send:
- Cell count (PMN >250/mm³ = SBP)
- Albumin (for SAAG calculation - simultaneous serum albumin needed)
- Total protein
Additional Studies (Situational):
| Test | Indication |
|---|---|
| Gram stain + culture | Infection |
| Glucose, LDH | Bacterial peritonitis |
| Amylase | Pancreatic ascites |
| Triglycerides | Chylous ascites |
| Cytology | Malignancy |
| Bilirubin | Bilious ascites |
| TB culture/PCR | TB peritonitis |
- Yamada's Textbook of Gastroenterology, 7th Ed.
Serum-Ascites Albumin Gradient (SAAG)
SAAG = Serum albumin - Ascites albumin (both measured same day)
SAAG reflects hepatic sinusoidal pressure and is ~97% accurate in diagnosing portal hypertension as the cause.
| SAAG | Interpretation | Causes |
|---|---|---|
| ≥1.1 g/dL (high) | Portal hypertension | Cirrhosis, alcoholic hepatitis, congestive heart failure, Budd-Chiari, portal vein thrombosis, fulminant liver failure, myxedema, fatty liver of pregnancy |
| <1.1 g/dL (low) | Non-portal hypertensive | Nephrotic syndrome, peritoneal carcinomatosis, mesothelioma, TB peritonitis, chylous ascites, pancreatic ascites, bile ascites |
Ascites total protein provides additional information:
-
In cardiac ascites: light yellow fluid, low specific gravity, protein <25 g/L
-
In malignant/TB ascites: dark yellow, often blood-stained, protein >25 g/L
-
Yamada's Textbook of Gastroenterology, 7th Ed.
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Management
1. Salt Restriction + Diuretics (First-line for Cirrhotic Ascites)
- Dietary sodium restricted to ≤2 g/day (more restrictive diets compromise nutrition)
- Spironolactone (aldosterone antagonist): start 100 mg/day, titrate every 3-4 days to max 400 mg/day - more effective than loop diuretics
- Furosemide: start 40 mg/day, escalate to 160 mg/day; add concurrently if tense ascites, or if hyperkalemia or inadequate weight loss on spironolactone alone
- Target weight loss: 1 kg/week (first week), then 2 kg/week thereafter
- Do not exceed: 0.5 kg/day without edema; 1 kg/day with edema
- Avoid: ACEIs, ARBs, NSAIDs (worsen renal function)
Diuretic side effects: hypovolemic hyponatremia, hyperkalemia, renal dysfunction, encephalopathy, gynecomastia (spironolactone)
2. Albumin Infusion
- Long-term albumin (40 g twice weekly x 2 weeks, then 40 g weekly) added to diuretics significantly reduces recurrent ascites and improves 18-month survival
- After large-volume paracentesis (>5L): albumin 6-8 g IV per liter removed to prevent paracentesis-induced circulatory dysfunction (PICD)
3. Large-Volume Paracentesis (LVP)
- Used in 10-20% of patients refractory to diuretics
- Goal: removal of all or most fluid
- Mandatory albumin supplementation when >5 L removed (8 g/L removed)
- Improves comfort, respiratory effort, oral intake, and reduces SBP risk
4. TIPS (Transjugular Intrahepatic Portosystemic Shunt)
- More effective than LVP + albumin in preventing recurrent ascites
- BUT associated with higher rate of hepatic encephalopathy
- Polytetrafluoroethylene-covered TIPS in patients needing >2 LVP/month: may improve survival
5. Peritoneovenous Shunt
- Silicone tube placed subcutaneously transferring ascitic fluid from peritoneal cavity to systemic circulation
- For patients not candidates for TIPS or liver transplantation
6. Automated Flow Pumps
- Move ascitic fluid to the bladder; reduce need for LVP and improve QoL
- Require surgical placement; risk of infection
7. Liver Transplantation
-
Definitive treatment for cirrhotic ascites
-
Goldman-Cecil Medicine
-
Rosen's Emergency Medicine
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Complications
Spontaneous Bacterial Peritonitis (SBP)
- Defined as infection of previously sterile ascitic fluid without an intraabdominal source (no GI perforation)
- Most common cause of primary peritonitis
- Pathogens: mainly gram-negative aerobes (E. coli, Klebsiella) and anaerobes
- Diagnosis: ascitic fluid PMN >250 cells/mL
- Treatment: broad-spectrum antibiotics covering gram-negatives + anaerobes, tailored to cultures
- Suspect SBP in: abdominal pain/tenderness, fever, leukocytosis, sepsis, renal insufficiency, hepatic encephalopathy
- Gram stain often negative (low bacterial counts in the fluid)
Hepatorenal Syndrome (HRS)
- Functional kidney injury from hemodynamic abnormalities in end-stage liver disease + severe portal hypertension
- High mortality despite specific therapy
- HRS in absence of prerenal azotemia = indication to consider liver transplantation
Hyponatremia
- Severe (serum Na <130 mEq/L): fluid restrict to 1.5 L/day
- Tolvaptan (V2-receptor antagonist) may transiently raise serum Na but has no overall survival benefit and carries hepatotoxicity risk - not routinely approved; short-term use as bridge to transplant only
Hepatic Encephalopathy
- Cumulative survival: 20-40% at 1 year, 15% at 3 years once encephalopathy develops
Hepatic Hydrothorax
- Ascitic fluid tracking through diaphragmatic defects, usually into the right pleural space
Special Fluid Characteristics
| Type | Appearance | Protein | SAAG | Notes |
|---|---|---|---|---|
| Cirrhotic | Straw-colored | Low | ≥1.1 | Commonest |
| Cardiac | Light yellow | Low (<25 g/L) | ≥1.1 | Low specific gravity |
| Malignant | Dark yellow/blood-stained | High (>25 g/L) | <1.1 | Cytology positive |
| TB | Straw/turbid | High | <1.1 | Lymphocytic predominance |
| Chylous | Milky | High | <1.1 | Triglycerides >200 mg/dL |
| Pancreatic | Variable | High | <1.1 | Amylase very elevated |
| Meigs' | Straw | Variable | Variable | Resolves with ovarian fibroma resection |
Sources: Harrison's Principles of Internal Medicine, 22E | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Yamada's Textbook of Gastroenterology, 7th Ed. | Goldman-Cecil Medicine | Bailey and Love's Short Practice of Surgery, 28th Ed. | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.