Teach me PUK for ophthalmology PG exam considering all point that should be taken in mind to impress external
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive data from Kanski's and Wills Eye Manual. Let me compile the complete exam-oriented answer.
PUK (Peripheral Ulcerative Keratitis) - Complete PG Exam Guide
Sources: Kanski's Clinical Ophthalmology 10th Ed., Wills Eye Manual
WHAT TO SAY FIRST (Examiner Hook)
"PUK is a potentially sight-threatening and life-threatening condition because it may be the first manifestation of a systemic vasculitis. Its detection mandates urgent systemic workup."
This line alone impresses an external examiner - it shows you understand the systemic importance.
1. DEFINITION
PUK is a crescentic peripheral stromal ulceration at the limbus with:
- Epithelial defect
- Stromal infiltration and thinning
- Associated limbal inflammation (limbitis/episcleritis/scleritis)
2. PATHOGENESIS (Score Points Here)
The mechanism - which examiners love - involves a 3-step cascade:
- Immune complex deposition in the peripheral cornea (the peripheral cornea is uniquely vulnerable due to proximity to limbal vasculature)
- Episcleral and conjunctival capillary occlusion → cytokine release + inflammatory cell recruitment
- Upregulation of collagenases (MMPs) + reduced activity of their inhibitors → stromal melting
Key point to say: "The peripheral cornea is a watershed area where immune complexes preferentially deposit, making it the battleground for systemic autoimmune disease."
3. SYSTEMIC ASSOCIATIONS (Must Know in Order)
| Rank | Condition | Key Examiner Point |
|---|---|---|
| 1st | Rheumatoid Arthritis | Most common; PUK bilateral in 30%; occurs in advanced RA |
| 2nd | Granulomatosis with Polyangiitis (GPA/Wegener's) | Ocular features are presenting feature in 50%; c-ANCA positive |
| 3rd | Polyarteritis nodosa | p-ANCA |
| 4th | Relapsing polychondritis | Topical steroids may actually help here (exception!) |
| 5th | Systemic lupus erythematosus | ANA positive |
| Others | Crohn disease, IBD |
Examiner Tip: "Nearly 50% of patients with PUK have an associated systemic collagen vascular disease - RA is the most common." - Goldman-Cecil Medicine
4. CLINICAL FEATURES
Symptoms
- Pain (prominent, may be severe)
- Photophobia
- Blurred vision
- Redness
Signs (slit-lamp findings to rattle off)
- Crescentic ulceration with epithelial defect at the limbus
- Stromal infiltration and thinning - peripheral
- Spread is circumferential (and occasionally central)
- No clear zone between the ulcer and the limbus (same as Mooren)
- Limbitis, episcleritis, or scleritis are usually present
- Scleral extension can occur - KEY differentiator from Mooren ulcer
- Advanced: "Contact lens cornea" - extreme thinning
- Advanced: Perforation
Special Variant - Rheumatoid PCUK
- Paracentral (not peripheral) location
- Punched-out lesion with little infiltrate
- In a quiet eye (no scleritis)
- Can perforate rapidly
- Responds well to topical ciclosporin ± bandage contact lens ± tissue glue
- Usually does NOT need systemic treatment
5. PUK vs MOOREN ULCER - THE CLASSIC COMPARISON TABLE
This table is asked in nearly every exam:
| Feature | PUK (Systemic) | Mooren Ulcer |
|---|---|---|
| Systemic disease | Present | Absent (diagnosis of exclusion) |
| Scleral involvement | Yes | No |
| Scleritis | Common | Absent (limbitis only) |
| Bilaterality | 30% (in RA) | Can be bilateral (aggressive type) |
| Pathogenesis | Immune complex deposition | Autoimmune to calgranulin C |
| Pain | Yes | Yes (severe) |
| Undermined edge | Not characteristic | Characteristic |
| Treatment | Systemic immunosuppression | Topical steroids first; systemic if needed |
| Hepatitis C association | No | Yes (Mooren-like ulcer) |
6. MOOREN ULCER (Know This to Compare)
- Definition: Rare, progressive circumferential peripheral stromal ulceration - idiopathic autoimmune
- Antigen: May represent host reaction to calgranulin C (hidden corneal antigen)
- Two types:
- Type 1 (Benign): Older patients, unilateral, responds to medical therapy
- Type 2 (Aggressive): Younger patients, bilateral, South Asian men, severe pain, needs systemic immunosuppression
- Hallmark sign: Undermined and infiltrated leading edge
- Vascularization occurs up to (but NOT beyond) the leading edge
- No scleritis (this is key - if scleritis is present, think systemic PUK)
- HCV association - Mooren-like ulcer associated with hepatitis C
7. WORKUP (Demonstrate Systematic Approach)
Say: "I would take a detailed history and perform a systemic workup in collaboration with an internist/rheumatologist."
History
- Connective tissue disease symptoms (joint pain, skin rash, oral ulcers)
- Contact lens use
- Prior HSV/VZV keratitis
- Inflammatory bowel disease
- Prior ocular surgery
Investigations
Ocular:
- Slit-lamp examination (infiltrate, epithelial defect, AC reaction, scleritis)
- Corneal sensation (rule out neurotrophic)
- Schirmer test (dry eye)
- Corneal scrapings + cultures (rule out infection first!)
- Dilated fundus exam (cotton-wool spots = connective tissue disease; posterior scleritis signs)
Systemic:
| Test | Target Disease |
|---|---|
| ESR, CRP | Inflammation marker |
| CBC with differential | Rule out leukemia |
| Rheumatoid factor (RF) | RA |
| ANA | SLE |
| c-ANCA (PR3) | GPA/Wegener's |
| p-ANCA (MPO) | Polyarteritis nodosa, microscopic polyangiitis |
| ACE level | Sarcoidosis |
| Chest X-ray / CT | GPA, sarcoidosis |
| HCV serology | Mooren-like ulcer |
8. TREATMENT
Step-by-step approach to impress examiner:
Step 1 - Rule out infection first
"PUK is caused by infection until proven otherwise." - Kanski's (This line scores marks)
Step 2 - General/Supportive
- Preservative-free lubricants (artificial tears)
- Topical antibiotic prophylaxis if epithelial defect present (e.g., erythromycin ointment)
- Cycloplegic (cyclopentolate 1% or atropine 1%) if AC reaction or pain present
- Protective glasses (polycarbonate) during day; eye shield at night
Step 3 - Anticollagenase therapy
- Doxycycline 100 mg OD or BD - for anticollagenase (MMP inhibitor) effect
- Ascorbic acid (Vitamin C) 1-2 g/day - collagen synthesis promoter
Step 4 - Immunosuppression (the main treatment)
- Systemic steroids (prednisone 60-100 mg/day) - for acute control; pulsed IV for severe disease
- Add antiulcer prophylaxis (pantoprazole 40 mg or ranitidine 150 mg BD)
- Steroid-sparing agents for long-term:
- Methotrexate, mycophenolate mofetil, azathioprine
- Cyclophosphamide (especially for GPA)
- Infliximab, Rituximab (biologics - "show promise")
- Always coordinate with rheumatologist
Step 5 - Topical immunosuppression
- Topical cyclosporin A (up to 2%) - takes weeks to work
- Tacrolimus 0.1% ointment - for refractory cases
CRITICAL WARNING about topical steroids:
"Topical steroids should be used with CAUTION or generally AVOIDED in PUK because they can worsen corneal thinning and risk perforation. The notable EXCEPTION is relapsing polychondritis where topical steroids may actually improve the thinning."
Step 6 - Surgical
- Conjunctival resection/recession if no response to medical therapy (extends 4 mm from limbus, 2 mm beyond margins)
- Keratoepithelioplasty - donor corneal lenticule sutured onto scleral bed as physical barrier
- Cyanoacrylate tissue adhesive - impending/actual perforation
- Amniotic membrane graft - impending perforation
- Lamellar or penetrating keratoplasty - visual rehabilitation once inflammation settles (with immunosuppressive cover)
9. DIFFERENTIAL DIAGNOSIS OF PERIPHERAL CORNEAL THINNING
Know this list to show breadth:
| Condition | Key Feature |
|---|---|
| PUK (systemic) | Inflammatory, scleral involvement, systemic disease |
| Mooren ulcer | Inflammatory, undermined edge, no scleritis, idiopathic |
| Terrien marginal degeneration | Non-inflammatory, superior, men >75%, lipid line, intact epithelium |
| Pellucid marginal degeneration | Non-inflammatory, inferior (4-8 o'clock), protrusion ABOVE thinning |
| Furrow degeneration | Non-inflammatory, peripheral to arcus senilis, elderly |
| Marginal (staphylococcal) keratitis | Limbal clearing zone present (2 mm gap from limbus) |
| Delle | Adjacent to elevation, resolves with lubrication |
| Sclerokeratitis | Associated scleritis, rule out GPA |
| Exposure/neurotrophic keratopathy | Inferior location, no inflammation |
| Dry eye | Inferior/interpalpebral, Schirmer reduced |
10. HIGH-YIELD EXAMINER POINTS (Say These Verbatim)
- "PUK may precede the onset of systemic features" - meaning the eye is the window to undiagnosed vasculitis
- "PUK in a quiet eye with a punched-out paracentral lesion = Rheumatoid PCUK" - distinct entity, responds to topical ciclosporin
- "Topical steroids are generally avoided in PUK - except in relapsing polychondritis"
- "GPA (Wegener's) is the second most common cause, but ocular features are the PRESENTING feature in 50% of GPA cases"
- "Nearly 50% of patients with PUK have a systemic collagen vascular disease"
- "Doxycycline works by MMP inhibition, not by its antibiotic effect"
11. CLINICAL PHOTOGRAPH
Here is a slit-lamp image of PUK showing peripheral corneal ulceration with surrounding conjunctival injection:
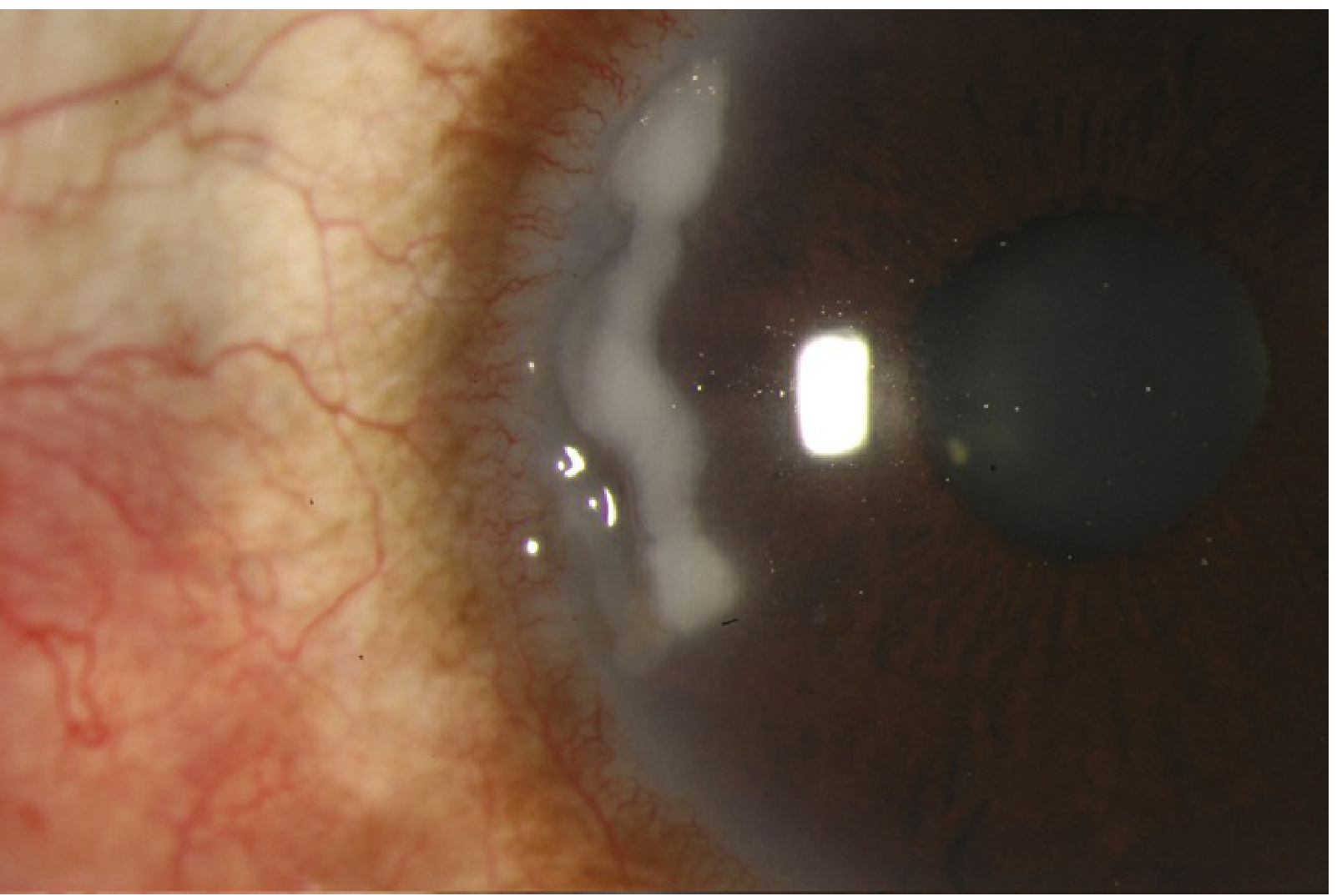
Note the white stromal opacity at the peripheral cornea with limbal vascular engorgement - classic PUK appearance.
12. HOW TO STRUCTURE YOUR ANSWER IN VIVA
When examiner asks "Tell me about PUK":
- Open with the life-threatening angle (systemic vasculitis)
- Define it (crescentic peripheral ulceration)
- Pathogenesis (immune complex → collagenase cascade)
- Systemic associations in order (RA > GPA > PAN > RP > SLE)
- Clinical features with the PUK vs Mooren comparison
- Workup (infection first, then systemic)
- Treatment (doxycycline + systemic immunosuppression, avoid topical steroids, biologics)
- Surgical options (conjunctival resection → glue → keratoplasty)
- End with the exception (relapsing polychondritis and topical steroids)
This structure shows you understand the disease, not just memorized facts.
Sources: Kanski's Clinical Ophthalmology 10th Ed., p. 239-241 | Wills Eye Manual, Chapter 4.22
This is a shared conversation. Sign in to Orris to start your own chat.