SIMPLE WAY TO UNDERSTAND MI IN ECG
Reading File
Finding Sources
Searching Images
myocardial infarction ECG changes ST elevation Q wave
Finding Sources
Loading Image
Loading Image
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Searching Images
ECG evolution STEMI hyperacute T wave ST elevation Q wave inversion diagram
Reading File
Loading Image
Loading Image
Here is a clear, structured guide to understanding MI on the ECG — from basic concepts to localization.
MI on the ECG — A Simple Guide
1. The Core Concept: Why Does MI Change the ECG?
When a coronary artery is blocked, the affected myocardium can no longer depolarize or repolarize normally. This creates a current of injury — an electrical gradient between healthy and ischemic tissue — which distorts the ST segment and other waveforms.

- Subendocardial ischemia (inner wall only) → ST vector points inward → leads overlying the area show ST depression
- Transmural ischemia (full thickness, as in STEMI) → ST vector points outward → overlying leads show ST elevation
2. The Three Classic ECG Changes of MI
Think of them as a timeline — they appear in sequence:
| Phase | Timing | ECG Finding | What It Means |
|---|---|---|---|
| Hyperacute | Minutes | Tall, broad, peaked T waves | Very early ischemia — often missed |
| Acute | Minutes–hours | ST elevation (tombstoning) | Active transmural injury (STEMI) |
| Evolving | Hours–days | T wave inversion | Tissue injured but not yet dead |
| Established | Hours–weeks | Pathological Q waves | Myocardial necrosis (dead tissue) |
The Pathological Q Wave Rule:
Width ≥ 0.04 s (1 small square) AND depth ≥ 25% of the R wave height = pathological Q wave → indicates myocardial necrosis
Q waves develop most commonly at 8–12 hours after infarction onset.
3. STEMI Diagnostic Criteria (Fourth Universal Definition)
ST elevation in ≥2 contiguous leads:
- V2–V3: ≥2.5 mm in men <40 yrs | ≥2 mm in men >40 yrs | ≥1.5 mm in women
- All other leads: ≥1 mm
4. Localizing the MI — Which Leads Tell You Which Wall?
This is the most clinically useful part. Match the leads with the anatomy:
| ECG Leads Showing Changes | Wall Affected | Artery Usually Blocked |
|---|---|---|
| V1–V4 | Anterior | LAD (Left Anterior Descending) |
| V1–V2 | Septal | LAD (septal branches) |
| V5–V6, I, aVL | Lateral | LCx (Left Circumflex) |
| V1–V6 + I + aVL | Anterolateral | LAD (proximal) or Left Main |
| II, III, aVF | Inferior | RCA (Right Coronary Artery) |
| V1–V3 depression (reciprocal) | Posterior | RCA or LCx |
| Right-sided leads (V3R–V4R) | Right Ventricle | Proximal RCA |
Memory tip: Think of the leads as "cameras" pointed at the heart — whatever wall they face, they record those changes.
5. Reciprocal Changes — The Mirror Image
Reciprocal ST depression in the opposite leads strongly confirms a true STEMI (vs. benign elevation):
- Inferior STEMI (II, III, aVF elevation) → ST depression in I and aVL
- Anterior STEMI → ST depression in III and aVF
- Posterior MI → ST depression in V1–V3 (the "window" looking at the posterior wall from the front)
6. Real ECG Examples
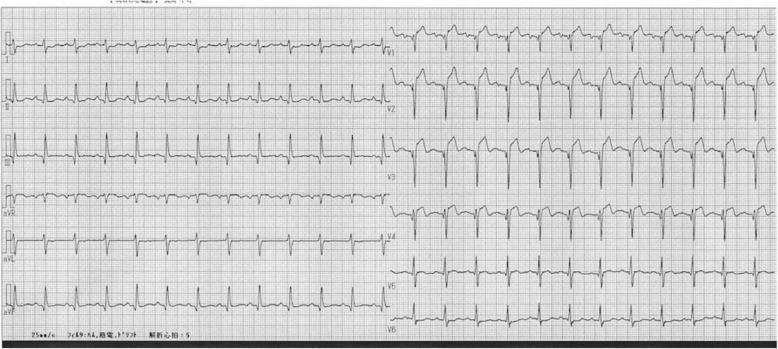
Acute Anterior STEMI (LAD occlusion) — "tombstone" morphology in V2–V4:
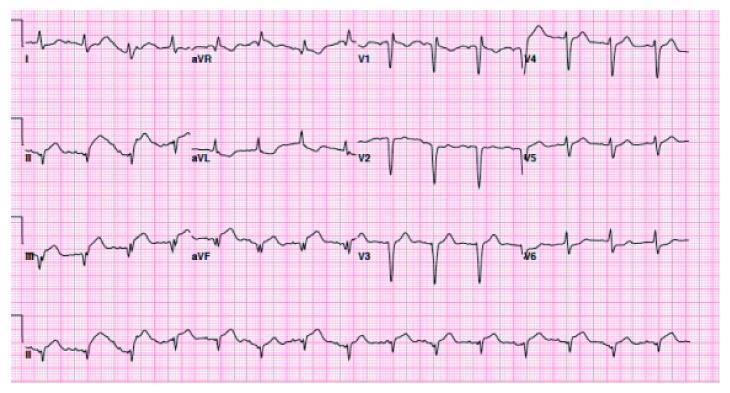
Acute Inferior STEMI (RCA occlusion) — ST elevation in II, III, aVF with reciprocal depression in aVL:
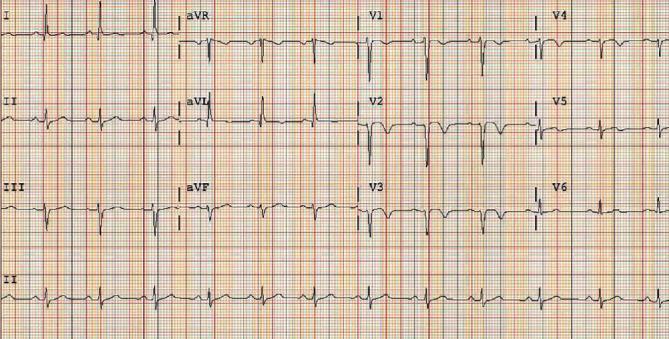
Subacute/Evolving Anterior MI — Q waves and deep T inversions in V2–V5 (post-infarction pattern):
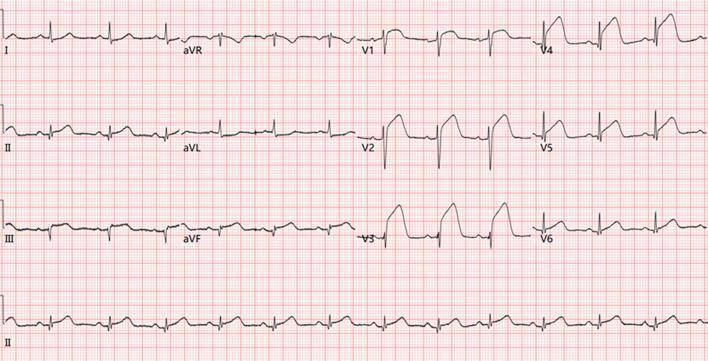
Extensive STEMI — Combined anterior + inferior involvement with tombstoning:
7. NSTEMI vs. STEMI — Quick Distinction
| Feature | STEMI | NSTEMI |
|---|---|---|
| Mechanism | Complete occlusion (transmural) | Partial occlusion (subendocardial) |
| ECG | ST elevation ± Q waves | ST depression and/or T wave inversion (no STE) |
| Treatment | Emergent reperfusion (PCI/thrombolysis) | Anticoagulation + early PCI |
8. One Simple Reading Approach (Bedside Checklist)
- Is there ST elevation? → In which leads? → Localise the wall
- Are there reciprocal depressions? → Confirms STEMI
- Are there Q waves? → Established infarction
- Are there T-wave inversions? → Evolving ischemia or post-STEMI
- Is there ST depression only? → Think NSTEMI or posterior MI
Sources: Harrison's Principles of Internal Medicine 22E; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.