LUNG ABSCESS Definition Severe localized suppurative process within lung parenchyma leading to cavity formation containing pus. Etiology A. Infectious • Bacterial (most common) • Anaerobes (oral flora): Peptostreptococcus, Fusobacterium. • Aerobes: Staphylococcus aureus, Klebsiella, Pseudomonas. • Mycobacterium tuberculosis. • Fungal: Aspergillus, Cryptococcus. • Parasitic: Entamoeba histolytica, Strongyloides. B. Non-infectious • Vasculitis • Pulmonary embolism • Sarcoidosis Pathogenesis • Primary lung abscess (most common): Due to aspiration. Common organisms are oral anaerobes. • Secondary lung abscess: Due to pre-existing lung disease such as Bronchiectasis or obstructing bronchogenic carcinoma. Organisms: Staph, Pseudomonas, Klebsiella. Clinical Features Symptoms • Acute: Fever, chills and rigors, chest pain, foul-smelling expectoration, cough. • Chronic: Weight loss, malaise, anorexia, deep-seated chest pain. Signs • Consolidation: Crepitations, ↑ vocal fremitus, dullness on percussion. • Cavitation: Cavernous / amphoric breathing, coarse crepitations. Complications • Empyema • Pleural effusion • Hemorrhage / Hemoptysis • Fibrosis Investigations • Chest X-ray: Shows a cavity with an air-fluid level. • Blood tests • Sputum examination • CT chest • Bronchoscopy: Used to exclude malignancy, obtain specimens, and remove secretions. Treatment 1. Supportive • Postural drainage • Chest physiotherapy 2. Antibiotic therapy (4–6 weeks) • Empirical (oral): Ampicillin, Cotrimoxazole, Clindamycin (DOC for anaerobes). • Severe disease: IV clindamycin, IV metronidazole \pm carbapenem. 3. Interventional • Large abscess: Aspiration / pigtail catheter. 4. Surgery • Lobectomy / Pneumonectomy if: Persistent abscess, massive hemoptysis, or underlying bronchogenic carcinoma. Explain this concept in very easy and simple way covering all the points
🫁 Lung Abscess - Made Simple
What Is It? (Definition)
Think of it like a boil (pimple) - but inside your lung.
What Causes It? (Etiology)
A. Infectious Causes (most common)
| Type | Examples |
|---|---|
| Bacteria - Anaerobes (mouth germs, no oxygen needed) | Peptostreptococcus, Fusobacterium |
| Bacteria - Aerobes (need oxygen) | Staph aureus, Klebsiella, Pseudomonas |
| TB bacteria | Mycobacterium tuberculosis |
| Fungi | Aspergillus, Cryptococcus |
| Parasites | Entamoeba histolytica, Strongyloides |
B. Non-Infectious Causes
- Vasculitis - blood vessel inflammation
- Pulmonary embolism - blood clot in lung
- Sarcoidosis - inflammatory disease
How Does It Develop? (Pathogenesis)
1. Primary Lung Abscess (Most Common)
- Caused by aspiration - when you accidentally inhale food, saliva, vomit, or oral secretions into the lungs
- This carries mouth bacteria (oral anaerobes) deep into the lung
- Common in: alcoholics, unconscious patients, post-surgery patients, epileptics (people who can't protect their airway properly)
2. Secondary Lung Abscess
- Happens because of a pre-existing lung problem:
- Bronchiectasis (damaged airways)
- Lung cancer blocking a bronchus
- Organisms here are tougher: Staph, Pseudomonas, Klebsiella
Simple analogy: Primary = you accidentally swallow dirty water into your lungs. Secondary = your lung was already sick and then got infected on top.
What Does the Patient Feel? (Clinical Features)
Symptoms - Acute (sudden onset)
- 🌡️ Fever with chills and rigors (shaking)
- 💨 Foul-smelling cough/sputum - this is a hallmark! The pus smells terrible because anaerobes produce bad odors
- 🤢 Chest pain
- Lots of coughing
Symptoms - Chronic (long-standing)
- ⚖️ Weight loss
- 😴 Malaise (general tiredness)
- 😞 Anorexia (loss of appetite)
- Deep-seated chest pain
Signs (what the doctor finds on examination)
- Crepitations (crackling sounds with stethoscope)
- Increased vocal fremitus (vibrations felt more strongly)
- Dullness on percussion (like tapping a solid object)
- Cavernous/Amphoric breathing - hollow, echoing sound (like blowing over a bottle's mouth)
- Coarse crepitations
What Can Go Wrong? (Complications)
| Complication | What Happens |
|---|---|
| Empyema | Pus spills into the space around the lung (pleural space) |
| Pleural Effusion | Fluid accumulates around the lung |
| Hemorrhage / Hemoptysis | Erosion of blood vessels causes coughing up blood |
| Fibrosis | Healing leaves scar tissue behind |
How Is It Diagnosed? (Investigations)
-
Chest X-Ray - The classic finding: a cavity with an air-fluid level (you see a dark hole with a white fluid level inside - like a half-filled cup)
-
Blood Tests - Check for infection markers (raised WBC, CRP)
-
Sputum Examination - Culture and sensitivity to identify the exact bacteria
-
CT Chest - More detailed view of the cavity, its walls, location, and surrounding tissue
-
Bronchoscopy - A camera passed into the airways to:
- Rule out cancer (which can mimic/cause abscess)
- Collect specimens
- Clear out secretions
How Is It Treated? (Treatment)
Step 1 - Supportive Care
- Postural drainage - Tilting the patient so gravity helps drain the pus out (like tipping a bottle)
- Chest physiotherapy - Tapping/vibrating the chest to loosen secretions
Step 2 - Antibiotics (4-6 weeks - long course!)
-
Mild/Moderate disease (oral):
- Ampicillin
- Cotrimoxazole
- Clindamycin = Drug of Choice for anaerobes (most common cause)
-
Severe disease (IV):
- IV Clindamycin
- IV Metronidazole
- +/- Carbapenem (if very serious or resistant bugs)
Why so long? Because the cavity is poorly vascularized - antibiotics take time to penetrate.
Step 3 - Interventional (if abscess is large)
- Aspiration or pigtail catheter - A needle/tube inserted to drain the pus out directly
Step 4 - Surgery (last resort)
- Abscess persists despite treatment
- Massive hemoptysis (life-threatening bleeding)
- Underlying bronchogenic carcinoma (lung cancer)
Quick Memory Summary
Lung Abscess = Pus-filled cavity in lung
Most common cause → Aspiration of oral anaerobes
Classic symptom → Foul-smelling sputum
Classic X-ray → Cavity with air-fluid level
Drug of choice → Clindamycin (for anaerobes)
Duration → 4-6 weeks antibiotics
Surgery when → Persistent / Hemoptysis / Cancer
Create a visual comparison poster of primary vs secondary lung abscess
Copd
Medical education poster: Visual comparison of Primary vs Secondary Lung Abscess. Split layout with two columns. Left column titled "PRIMARY LUNG ABSCESS" with blue theme, right column titled "SECONDARY LUNG ABSCESS" with orange theme. Each column includes sections for: Cause (with icon of aspiration on left, pre-existing lung disease on right), Common Organisms (anaerobes/oral flora on left, Staph/Pseudomonas/Klebsiella on right), Risk Factors (alcoholics, unconscious patients, post-surgery on left; bronchiectasis, lung cancer on right), Location (posterior segments on left, any segment on right), Prognosis (better response to antibiotics on left, harder to treat on right). Clean clinical medical poster style with lung diagrams, icons, bold headers, white background, professional medical illustration quality.
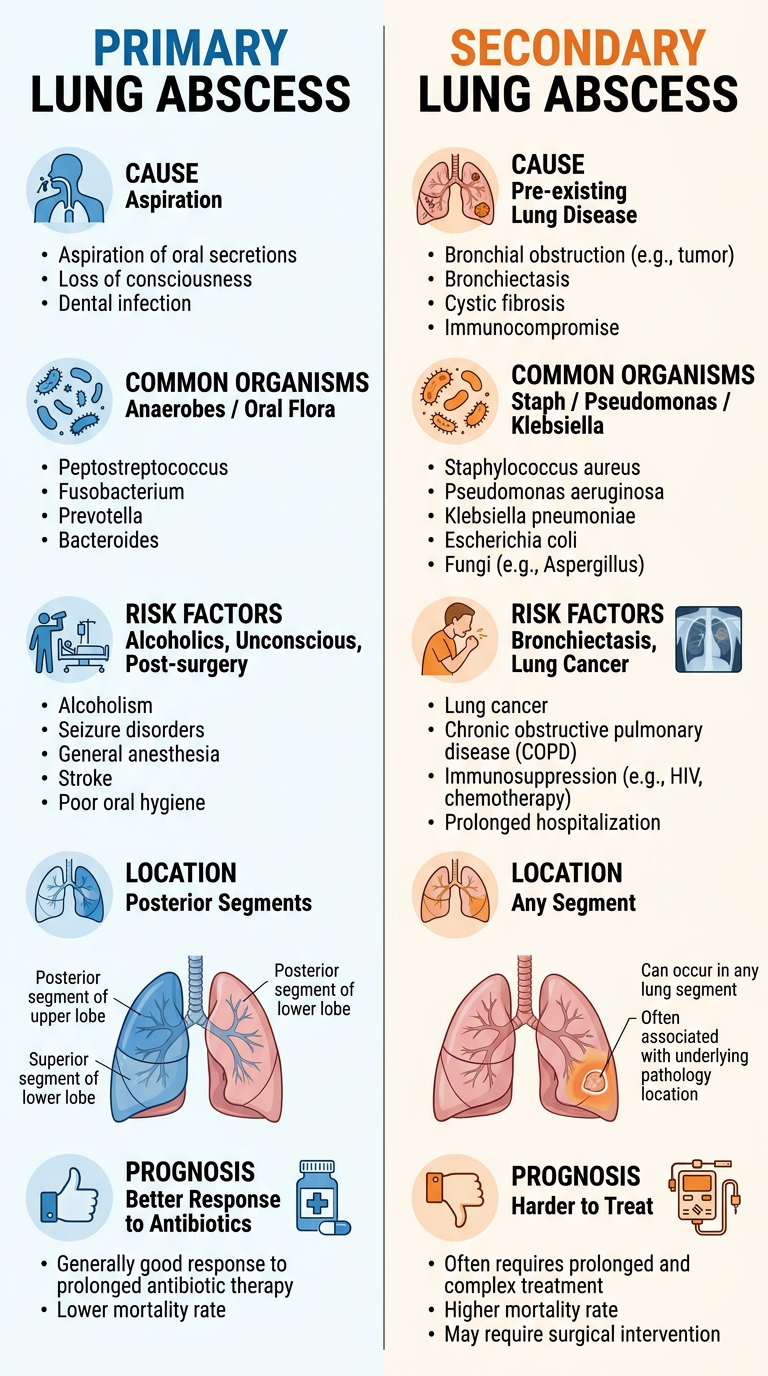
| Feature | Primary | Secondary |
|---|---|---|
| Cause | Aspiration of oral secretions | Pre-existing lung disease |
| Organisms | Oral anaerobes | Staph, Pseudomonas, Klebsiella |
| Risk factors | Alcoholics, unconscious, post-op | Bronchiectasis, lung cancer |
| Location | Posterior segments (gravity-dependent) | Any segment |
| Prognosis | Responds well to antibiotics | Harder to treat |
- Explain COPD in the same simple, easy style as the lung abscess breakdown?
- Create a visual poster for COPD (e.g., emphysema vs chronic bronchitis comparison)?
- Both?
Explain COPD pathophysiology in simple language
🫁 COPD Pathophysiology - Made Simple
What Is COPD?
The key word is OBSTRUCTION - air can get in, but it struggles to get OUT.
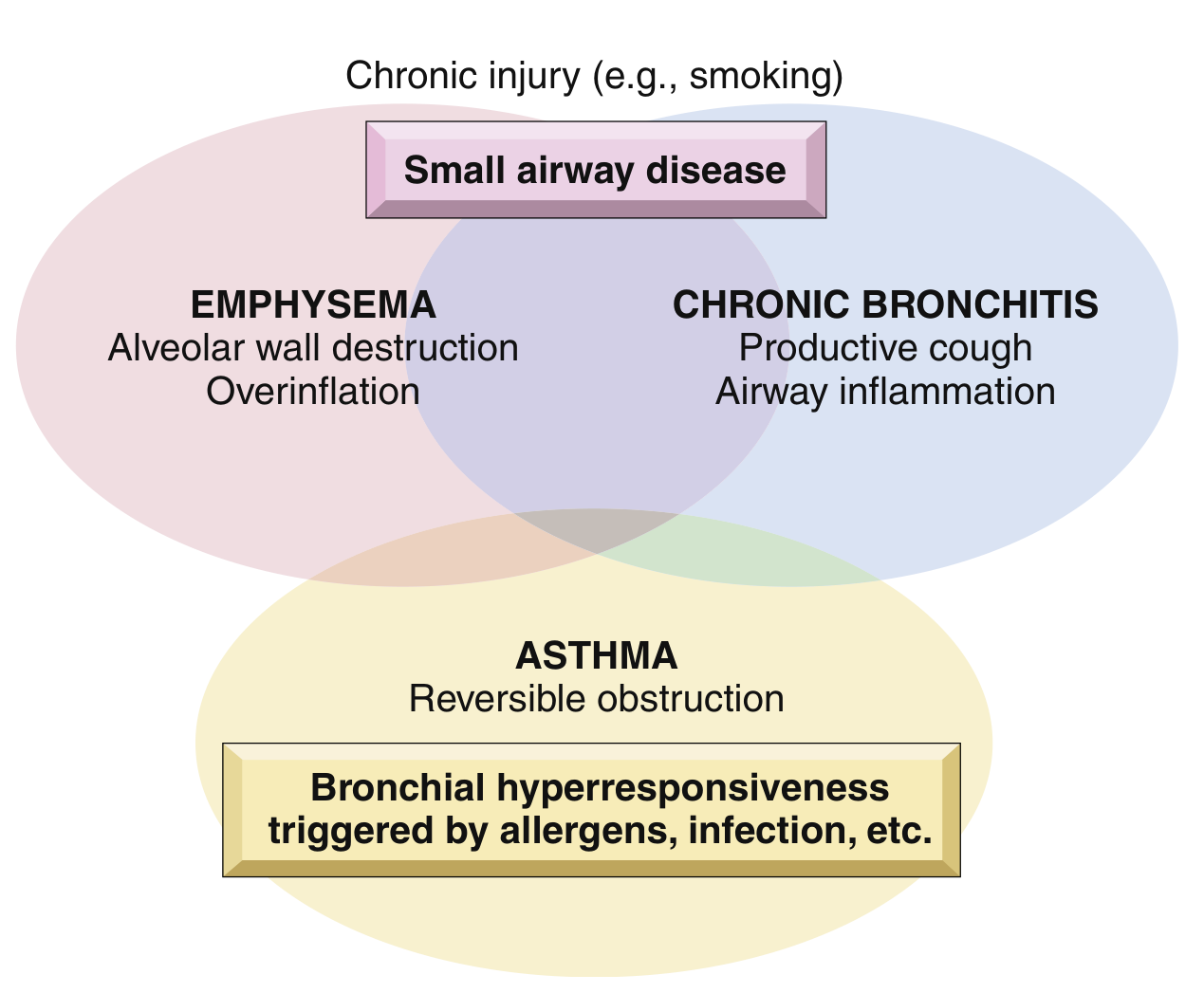
| Emphysema | Chronic Bronchitis | |
|---|---|---|
| Definition basis | Anatomical (lung structure destroyed) | Clinical (symptoms-based) |
| Core problem | Air sac walls destroyed | Airways blocked by mucus |
| Nickname | "Pink Puffer" | "Blue Bloater" |
The BIG Picture - What Causes It?
- 80% caused by cigarette smoking
- Other causes: air pollution, dust, fumes, genetic factors
- 35-50% of heavy smokers develop COPD
- Women are more susceptible than men
PART 1: EMPHYSEMA Pathophysiology
Normal Lung First
What Goes Wrong in Emphysema?
- Smoke overwhelms this defense
- Too much elastase, not enough AAT → Protease-Antiprotease Imbalance
- Small airways collapse during expiration (no radial traction)
- Air gets TRAPPED inside → lungs become over-inflated (barrel chest)
- Gas exchange is lost because the alveolar surface area is destroyed
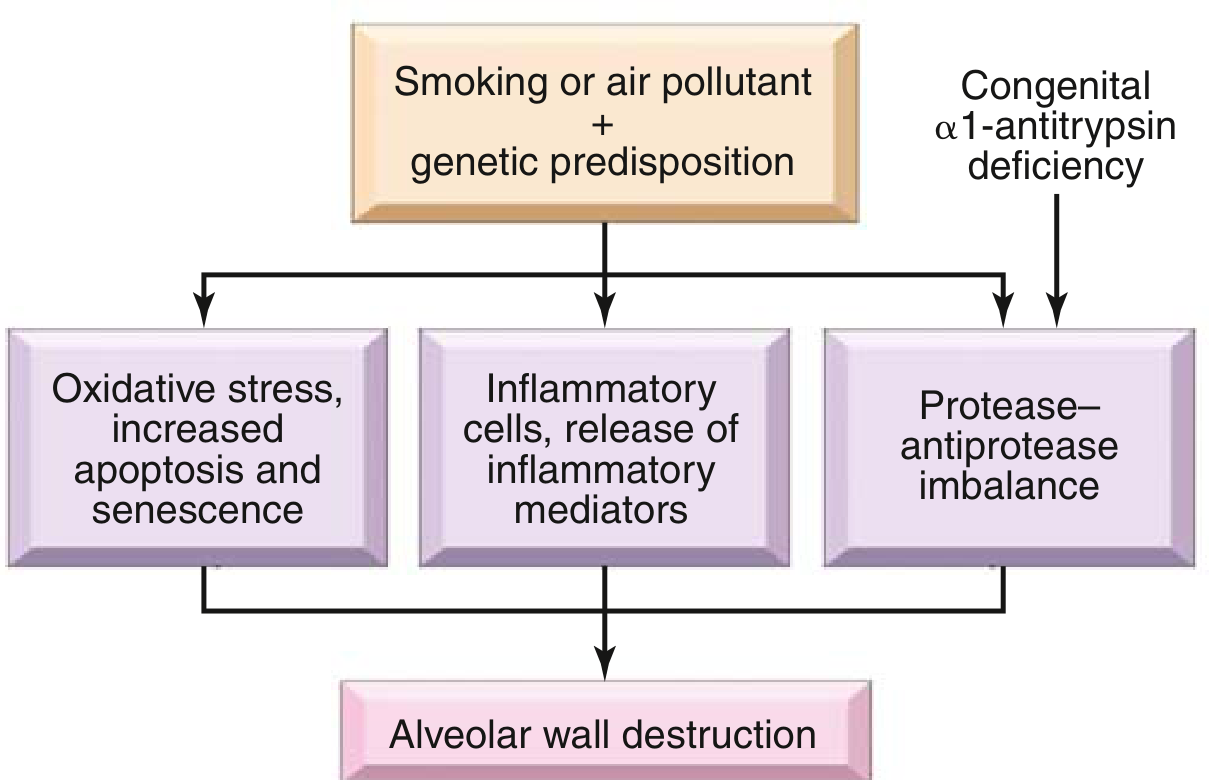
The Pathogenesis Diagram (from Robbins Basic Pathology):
Types of Emphysema
| Type | Where | Cause |
|---|---|---|
| Centriacinar (most common) | Central part of acinus, upper lobes | Cigarette smoking |
| Panacinar | Whole acinus, lower lobes | α1-antitrypsin deficiency |
| Distal acinar | Near pleura | Unknown - causes spontaneous pneumothorax |
| Irregular | Anywhere with scarring | Scar-related |
Memory trick: Centrilobular = Cigarettes (C-C). Panacinar = Pi gene deficiency (P-P).
PART 2: CHRONIC BRONCHITIS Pathophysiology
Definition (Clinical - not anatomical)
What Goes Wrong?
- Mucous glands in bronchi HYPERTROPHY (enlarge) - measured by the Reid Index (normally < 0.4; raised in chronic bronchitis)
- Goblet cells proliferate in smaller airways (they normally shouldn't be there)
- Result: Massive mucus overproduction (hypersecretion)
- IL-13 from T cells drives mucin production
- Neutrophil elastase also increases (same enzyme as in emphysema!)
- Note: Unlike asthma, NO eosinophils in chronic bronchitis
- Mucus plugs block bronchioles
- Inflammation causes bronchiolar wall swelling
- Fibrosis narrows the lumen further
- Eventually: Bronchiolitis obliterans (complete obliteration)
How Both Lead to the Same End Result
EMPHYSEMA CHRONIC BRONCHITIS
(Destroy the walls) (Clog the pipes)
↓ ↓
Elastic recoil lost Small airways blocked
↓ ↓
Airways collapse Mucus + fibrosis narrows airway
↓ ↓
←— AIRFLOW OBSTRUCTION —→
↓
FEV1/FVC ratio < 70%
↓
COPD diagnosed
The Overlap - Why They Co-exist
Key Diagnostic Marker
- FEV1/FVC < 70% (can't breathe out fast enough) = Obstructive pattern = COPD
- FEV1 = volume exhaled in the first 1 second
- The lower the FEV1, the more severe the COPD
Simple Summary
COPD Pathophysiology in 3 lines:
1. Smoking/pollution → Inflammation → Protease-antiprotease imbalance
→ Destroys alveolar walls → EMPHYSEMA (elastic recoil lost, air traps)
2. Smoking/pollution → Mucus gland hypertrophy + goblet cell proliferation
→ Small airway fibrosis + mucus plugging → CHRONIC BRONCHITIS
3. Both → FEV1/FVC < 70% → Irreversible airflow obstruction = COPD
26 years of female come with the complaint of sudden pain in her lower back on movements not able to lean forward feel relief when lie down in supine position ,lifting back up causing pain since 1 week its get normal them again occur
🏥 Clinical Case Analysis
🔍 Most Likely Diagnosis
Acute Mechanical Low Back Pain / Lumbar Disc Disease (Intervertebral Disc Prolapse)
🧩 Analyzing Her Symptoms
| Her Symptom | What It Tells Us |
|---|---|
| Sudden onset | Acute disc herniation or acute muscle/ligament strain |
| Pain on movement | Mechanical in nature (movement-dependent = musculoskeletal) |
| Cannot lean forward | Forward flexion compresses the disc anteriorly, pushing the herniated material further back - classic disc sign |
| Relief on lying supine | Lying flat removes axial load and disc pressure - hallmark of mechanical/disc pain |
| Worsened by lifting | Lifting increases intra-abdominal pressure and disc load - classic disc aggravator |
| Recurrent episodes | Recurrent disc herniation or recurrent muscle strain - very typical pattern |
| Age 26, female | Young adult - peak age for disc herniation and mechanical back pain |
As Morgan & Mikhail's Clinical Anesthesiology states directly: "Pain associated with disc disease is aggravated by bending, lifting, prolonged sitting... It is usually relieved by lying down." - This matches her presentation perfectly.
📋 Differential Diagnosis
| Diagnosis | For | Against |
|---|---|---|
| Lumbar Disc Prolapse (Most likely) | All symptoms match; recurrent; age group | No leg pain/sciatica mentioned |
| Acute Lumbar Muscle Strain | Sudden onset; movement-related; young; relief supine | Recurrent pattern less typical |
| Facet Joint Syndrome | Back pain worse on extension/movement | Typically worse leaning BACK not forward |
| Spondylolisthesis | Young female; recurrent | Usually chronic, not episodic |
| Endometriosis / Gynecological | Young female; recurrent | No mention of menstrual association |
| Sacroiliac Joint Dysfunction | Common in young women | SI pain usually unilateral, buttock radiation |
🔬 Understanding the Mechanism (Pathophysiology)
Normal disc:
[Vertebra] — [Annulus Fibrosus (tough outer ring)]
[Nucleus Pulposus (gel center)]
— [Vertebra]
In disc prolapse:
Lifting/bending → ↑ disc pressure
→ Nucleus Pulposus pushes/herniates through annulus
→ Bulge posteriorly → presses on nerve root or posterior ligament
→ PAIN
Why forward bending hurts:
Flexion compresses disc ANTERIORLY → pushes herniation POSTERIORLY → MORE nerve pressure → MORE PAIN
Why lying down helps:
Removes axial load → disc pressure drops → nerve decompresses → RELIEF
⚠️ Red Flags to Rule Out (Ask These!)
- 🚨 Bladder/bowel incontinence or retention → Cauda Equina Syndrome (surgical emergency)
- 🚨 Bilateral leg weakness → Large central disc herniation
- 🚨 Night sweats, fever, unexplained weight loss → Spinal TB, malignancy
- 🚨 History of cancer → Metastatic disease
- 🚨 Pain at rest / night pain → Inflammatory or sinister cause
- 🚨 Saddle anesthesia (numbness around genitals/inner thighs) → Cauda equina
🔎 Investigations
First Line
| Test | Purpose |
|---|---|
| X-ray lumbar spine (AP + lateral) | Rule out fracture, spondylolisthesis, scoliosis |
| MRI lumbar spine | Gold standard - shows disc herniation, nerve compression, disc degeneration |
Note: Routine MRI is NOT recommended for simple non-specific back pain (up to 30-40% of asymptomatic people have abnormal MRI findings). Only order if red flags present or no improvement in 6 weeks.
If Gynecological Cause Suspected
- Pelvic ultrasound
- Menstrual history
- CA-125 (if endometriosis suspected)
💊 Treatment
1. Conservative (First 4-6 weeks - most cases resolve)
- Stay active as tolerated - bed rest is NOT recommended (prolonged bed rest worsens outcomes)
- Avoid heavy lifting and sustained forward flexion
- Short periods of rest when severe
- NSAIDs (Ibuprofen, Diclofenac) - first-line for acute pain
- Muscle relaxants (Cyclobenzaprine, Methocarbamol) if muscle spasm component
- Paracetamol for mild pain
- McKenzie exercises (extension-based exercises for disc pain)
- Core strengthening
- Posture correction
- Local heat helps muscle spasm
2. If Not Resolving (6-12 weeks)
- Transforaminal epidural steroid injection - reduces nerve root inflammation
- Pregabalin - for neuropathic/radicular component
3. Surgery (Last resort - if conservative fails >6-12 weeks OR neurological deficit)
- Microdiscectomy - standard procedure; 70% of patients improve without surgery within this time frame
📌 Key Teaching Points for This Case
26F + sudden low back pain + worse on forward flexion
+ relieved lying supine + worse on lifting + recurrent
↓
= Classic Mechanical Back Pain / Lumbar Disc Disease
No red flags → Conservative management first
NSAIDs + Physiotherapy + Activity modification
MRI only if no improvement in 6 weeks
Important for this young woman: Given her age (26), it is also worth asking about her menstrual cycle - if the episodes coincide with her periods, endometriosis with uterosacral ligament involvement is a differential that should not be missed, as it causes cyclical lower back pain that may mimic disc disease in young females.