Atherosclerosis notes pathology by robbins mbbs 10 marks with flow chart and diagrams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content from both Robbins textbooks plus all the key diagrams. Let me compile the full 10-mark notes.
ATHEROSCLEROSIS - Pathology Notes (Robbins) - 10 Marks
DEFINITION
Atherosclerosis (Greek: athero = gruel/porridge; sclerosis = hardening) is a chronic inflammatory disease of large and medium-sized arteries characterized by intimal lesions called atheromas (atherosclerotic plaques) - raised lesions with a soft, grumous lipid core covered by a fibrous cap that protrude into vessel lumens and can rupture.
It is the most common cause of morbidity and mortality in the Western world, responsible for ~50% of all deaths.
EPIDEMIOLOGY
- Sites most affected (in decreasing order): Abdominal aorta > coronary arteries > popliteal arteries > descending thoracic aorta > internal carotid arteries > Circle of Willis vessels
- Causes: Ischemic heart disease (MI), stroke, aortic aneurysm, peripheral vascular disease
- Death rate in Eastern Europe is 3-5x higher than the USA; Africa, India, Southeast Asia rates now exceed the USA
RISK FACTORS
FLOW CHART: Risk Factors
RISK FACTORS FOR ATHEROSCLEROSIS
│
├── NON-MODIFIABLE (Constitutional)
│ ├── Genetics / Family history (most important independent RF)
│ ├── Age (incidence of MI increases 5x between ages 40-60)
│ ├── Male sex (premenopausal females relatively protected by estrogen)
│ └── Clonal hematopoiesis (CHIP - pro-inflammatory monocytes)
│
└── MODIFIABLE
├── MAJOR
│ ├── Hyperlipidemia (↑LDL, ↓HDL, ↑Lp[a]) ← most important
│ ├── Hypertension
│ ├── Cigarette smoking
│ └── Diabetes mellitus
│
└── ADDITIONAL / EMERGING
├── Inflammation (↑CRP, IL-6)
├── Hyperhomocysteinemia
├── ↑Plasminogen activator inhibitor-1
├── Lipoprotein(a) [Lp(a)]
├── Obesity
└── Physical inactivity
Key point - Hyperlipidemia:
- ↑LDL cholesterol = most important modifiable RF
- ↓HDL = independent risk factor (HDL promotes cholesterol efflux/reverse transport)
- LDL-lowering with statins reduces risk of MI by ~30%
- Oxidized LDL is far more atherogenic than native LDL
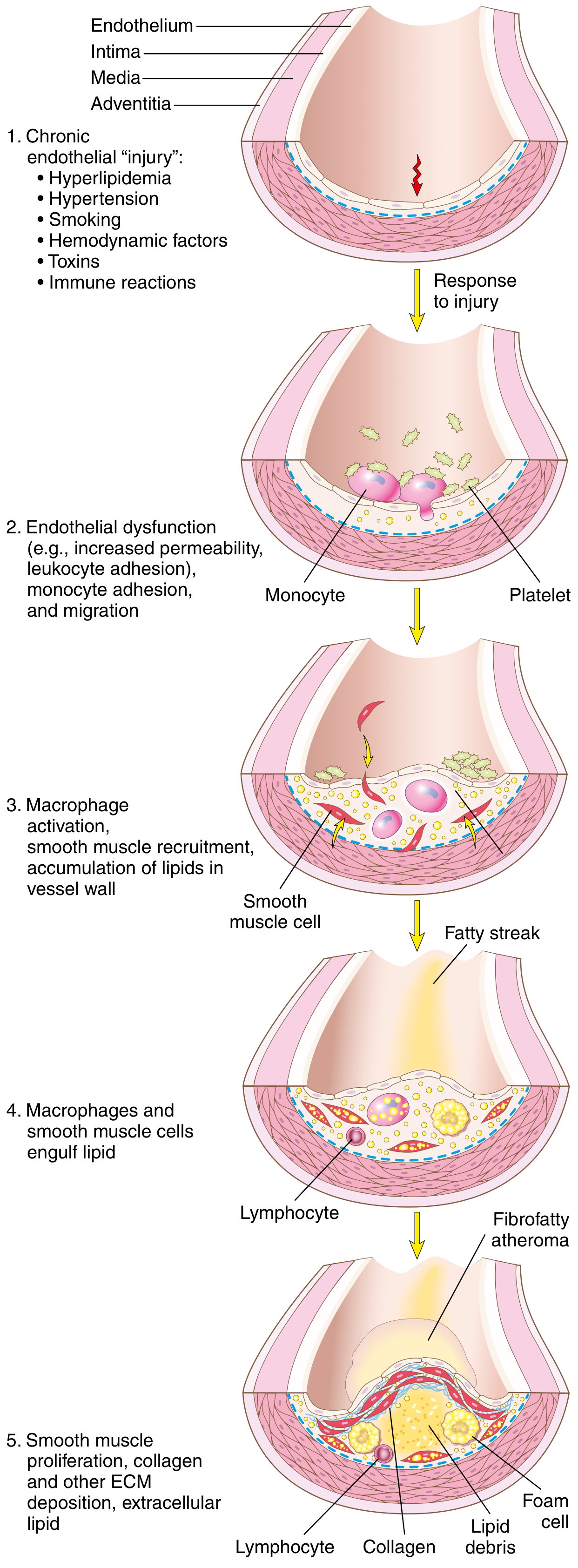
PATHOGENESIS
The currently accepted model is the "Response to Injury" Hypothesis (Ross, 1976, updated). Atherosclerosis is viewed as a chronic inflammatory response of the arterial wall to endothelial injury.
FLOW CHART: Pathogenesis of Atherosclerosis
ENDOTHELIAL INJURY / DYSFUNCTION
(Hyperlipidemia, HTN, Smoking, Hemodynamic turbulence, Toxins)
│
▼
ENDOTHELIAL DYSFUNCTION
• ↑Permeability to lipoproteins
• ↑Leukocyte adhesion molecule expression (VCAM-1, ICAM-1)
• Pro-thrombotic state
• ↓Nitric oxide (vasodilatory, anti-inflammatory)
│
├──────────────────────────────────────────┐
▼ ▼
LDL ACCUMULATION IN INTIMA MONOCYTE ADHESION & MIGRATION
• LDL oxidized by free radicals into intima
• Oxidized LDL is cytotoxic to ECs ↓
• Triggers further inflammation MACROPHAGES (via M-CSF)
│ + FOAM CELLS
└────────────────┬─────────────┘
▼
FATTY STREAK FORMATION
(earliest lesion - yellow intimal discoloration)
Foam cells = macrophages + SMCs engorged with lipid
│
▼
PLATELET ADHESION
(exposed subendothelial collagen)
│
▼
RELEASE OF GROWTH FACTORS & CYTOKINES
(PDGF from platelets, macrophages, ECs)
(FGF, TGF-α, TNF, IL-1, MCP-1)
│
▼
SMC RECRUITMENT (from media → intima)
SMC PROLIFERATION + ECM SYNTHESIS
(collagen, proteoglycans → FIBROUS CAP)
│
▼
ADVANCED ATHEROSCLEROTIC PLAQUE
• Fibrous cap (collagen, SMCs, macrophages)
• Necrotic/lipid core (foam cell debris,
cholesterol crystals, calcium)
• Shoulder region (most inflammatory)
Key cellular players:
| Cell | Role |
|---|---|
| Endothelial cells | Injury triggers the whole cascade; become dysfunctional |
| Monocytes/Macrophages | Engulf oxidized LDL → foam cells; release cytokines (TNF, IL-1, MMP) |
| Smooth muscle cells | Migrate from media → intima; proliferate; synthesize collagen (fibrous cap) |
| T lymphocytes | Produce IFN-γ → inhibit SMC collagen synthesis → plaque destabilization |
| Platelets | Adhere to injured endothelium; release PDGF, TGF-β |
MORPHOLOGY
Gross Appearance
1. Fatty Streak (earliest lesion)
- Flat or slightly raised yellow intimal streak or spot
- Composed of foam cells (lipid-laden macrophages + SMCs)
- Reversible - can appear in aorta of infants/children (harmless at this stage)
- Precursor to atherosclerotic plaques
2. Atherosclerotic (Fibrous/Atheromatous) Plaque
- Yellow-white raised intimal lesion, 0.3-1.5 cm diameter
- May coalesce → larger plaques
- Eccentric distribution (not circumferential)
- Patchy, irregular distribution throughout the vessel
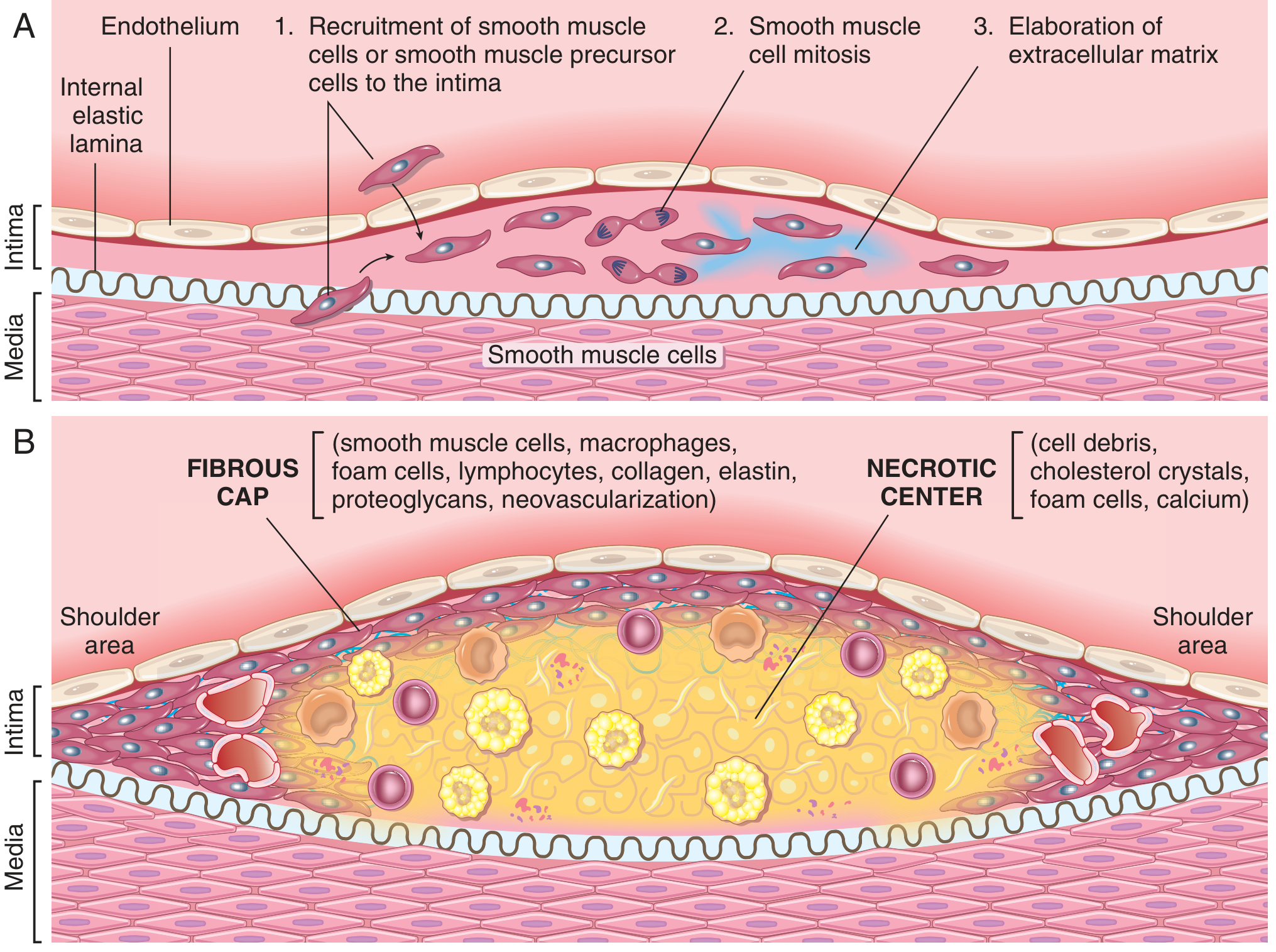
Components of a Mature Plaque (Microscopic)
LUMEN
│
▼
┌─────────────────────────────────┐
│ FIBROUS CAP │
│ • SMCs, macrophages, foam │
│ cells, T lymphocytes │
│ • Collagen, elastin, │
│ proteoglycans │
│ • Neovascularization │
│ SHOULDER (most vulnerable │
│ to rupture - most inflamed) │
├─────────────────────────────────┤
│ NECROTIC/LIPID CORE │
│ • Cell debris │
│ • Cholesterol crystals │
│ • Foam cells │
│ • Calcium deposits │
│ • Intraplaque hemorrhage │
│ (rupture of vasa vasorum) │
└─────────────────────────────────┘
│
MEDIA (compressed, may atrophy)
│
ADVENTITIA
Textbook Robbins Diagram - Atheromatous Plaque Structure:
PATHOGENESIS DIAGRAM (Robbins Classic)
STABLE VS. VULNERABLE PLAQUE
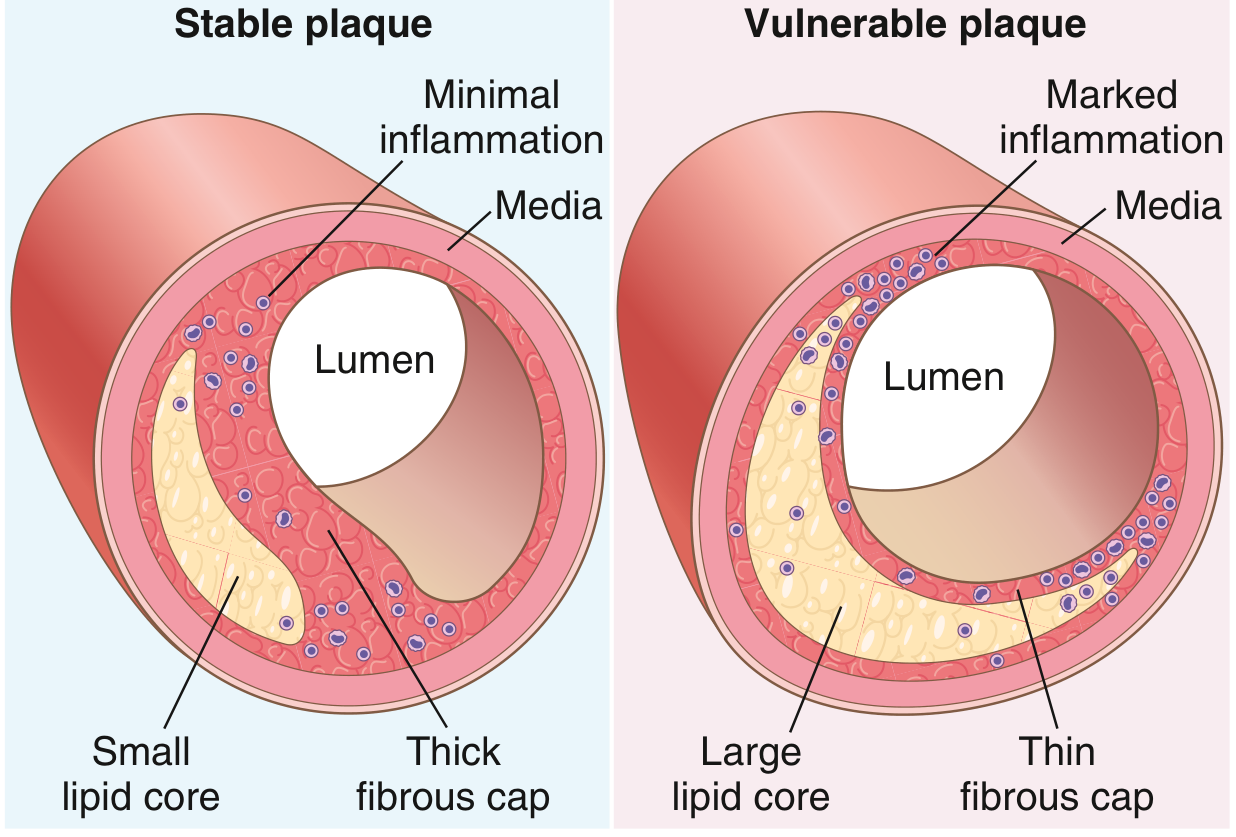
| Feature | Stable Plaque | Vulnerable Plaque |
|---|---|---|
| Fibrous cap | Thick | Thin |
| Lipid core | Small | Large |
| Inflammation | Minimal | Marked (foamy macrophages, T cells) |
| SMC content | High | Low |
| Collagen | Abundant | Reduced (MMPs degrade it) |
| Risk | Angina (stable) | ACS, MI, sudden death |
CONSEQUENCES / COMPLICATIONS
FLOW CHART: Complications of Atherosclerosis
ATHEROSCLEROTIC PLAQUE
│
├──── GRADUAL STENOSIS (>70% occlusion)
│ → Chronic ischemia
│ → Stable angina
│ → Intermittent claudication
│ → Mesenteric ischemia
│
├──── ACUTE PLAQUE CHANGE (rupture/erosion)
│ │
│ THREE TYPES:
│ 1. Rupture/Fissuring → exposed thrombogenic core
│ → THROMBOSIS (occlusive)
│ → MYOCARDIAL INFARCTION
│ → ISCHEMIC STROKE
│ → SUDDEN CARDIAC DEATH
│ 2. Erosion/Ulceration → exposed subendothelial
│ basement membrane
│ → partial thrombosis
│ 3. Intraplaque Hemorrhage → rupture of vasa vasorum
│ → rapid plaque expansion
│
├──── ATHEROEMBOLISM
│ • Plaque debris → microemboli downstream
│ • Can cause renal failure, bowel ischemia
│
└──── ANEURYSM FORMATION
• Plaque ischemia of media
• SMC loss + ECM degradation in media
• Weakens wall → dilatation
→ Abdominal Aortic Aneurysm (AAA) most common
→ Risk of rupture → hemorrhage → death
LESION SEQUENCE (AHA Classification)
TYPE I - Initial lesion
(isolated macrophage foam cells)
↓
TYPE II - Fatty streak
(multiple foam cell layers; visible yellow streaks)
[REVERSIBLE STAGE]
↓
TYPE III - Intermediate lesion
(foam cells + small extracellular lipid pools)
↓
TYPE IV - Atheroma
(large lipid core = "gruel"; endothelium intact)
↓
TYPE V - Fibroatheroma
(lipid core + fibrous cap = classic plaque)
[MOST CLINICALLY SIGNIFICANT]
↓
TYPE VI - Complicated lesion
(surface defect, hematoma, hemorrhage, thrombosis)
[CAUSES ACUTE EVENTS - MI, STROKE]
KEY MOLECULES SUMMARY TABLE
| Molecule | Source | Effect |
|---|---|---|
| Oxidized LDL | Oxidation of LDL in intima | Cytotoxic to ECs; stimulates foam cell formation |
| MCP-1 (CCL2) | Endothelial cells, SMCs | Recruits monocytes into intima |
| VCAM-1 | Dysfunctional endothelium | Adhesion of monocytes and T cells |
| PDGF | Platelets, macrophages, ECs | Stimulates SMC migration + proliferation |
| M-CSF | ECs, macrophages | Macrophage differentiation and activation |
| IFN-γ | T lymphocytes | Inhibits SMC collagen synthesis → cap weakening |
| MMPs (metalloproteinases) | Macrophages, foam cells | Degrade collagen → plaque instability |
| IL-1, TNF | Macrophages | Pro-inflammatory; upregulate adhesion molecules |
| HDL | Liver | Reverse cholesterol transport; protective |
| hsCRP | Liver (acute phase) | Marker of inflammation; independent risk predictor |
IMPORTANT EXAM POINTS (10-Mark Answer Tips)
- Definition: Chronic inflammatory disease of large/medium arteries - always mention "response to injury hypothesis"
- Fatty streak = earliest lesion - foam cells - reversible
- Plaque components: Fibrous cap (collagen, SMCs) + Necrotic core (lipid, calcium, debris)
- Vulnerable plaque = thin cap + large lipid core + marked inflammation = rupture → ACS
- Sites: Abdominal aorta > coronary > popliteal arteries
- Complications: Stenosis, thrombosis (MI, stroke), aneurysm, atheroembolism
- Role of oxidized LDL as central pathogenic molecule
- Foam cells = macrophages + SMCs engorged with oxidized LDL via scavenger receptors
REFERENCES
- Robbins & Kumar Basic Pathology, 11th ed. - Chapter 8 (Vascular Diseases), pp. 316-324
- Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th ed. - Chapter 11 (Blood Vessels), pp. 466-478
This is a shared conversation. Sign in to Orris to start your own chat.