Nasal turbinate anomalies in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
nasal turbinate hypertrophy concha bullosa anomalies
nasal turbinate anomalies concha bullosa paradoxical turbinate RGUHS ENT 20 marks
nasal turbinate anatomy concha bullosa paradoxical middle turbinate
inferior turbinate hypertrophy treatment surgery radiofrequency
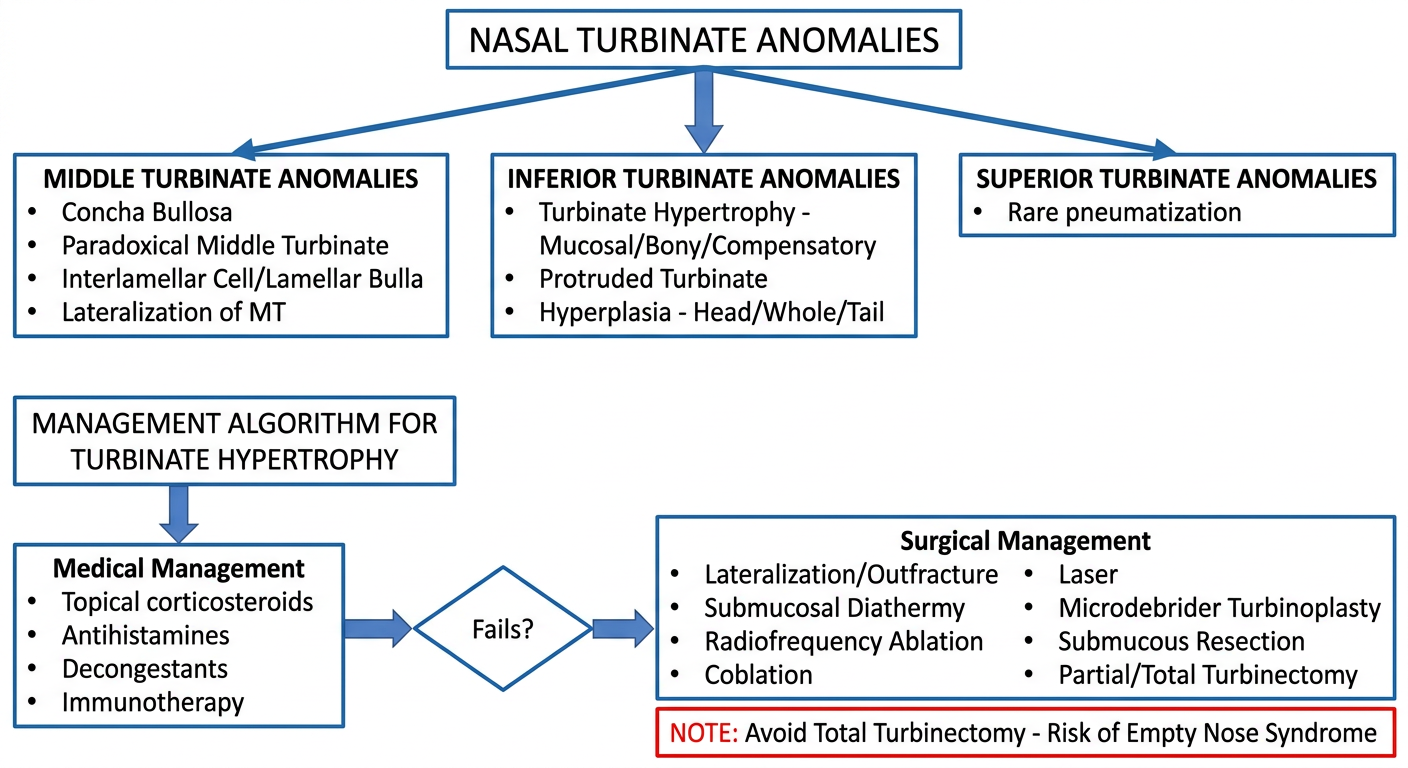
Medical flowchart for nasal turbinate anomalies showing: top box "NASAL TURBINATE ANOMALIES" branching into three main categories: "MIDDLE TURBINATE ANOMALIES" (containing: Concha Bullosa, Paradoxical Middle Turbinate, Interlamellar Cell/Lamellar Bulla, Lateralization of MT), "INFERIOR TURBINATE ANOMALIES" (containing: Turbinate Hypertrophy - Mucosal/Bony/Compensatory, Protruded Turbinate, Hyperplasia - Head/Whole/Tail), and "SUPERIOR TURBINATE ANOMALIES" (rare pneumatization). Below, a second flowchart titled "MANAGEMENT ALGORITHM FOR TURBINATE HYPERTROPHY" with: Medical Management box (Topical corticosteroids, Antihistamines, Decongestants, Immunotherapy) arrow to "Fails?" diamond, then Surgical Management box (Lateralization/Outfracture, Submucosal Diathermy, Radiofrequency Ablation, Coblation, Laser, Microdebrider Turbinoplasty, Submucous Resection, Partial/Total Turbinectomy), with note "Avoid Total Turbinectomy - Risk of Empty Nose Syndrome". Clean medical diagram style with labeled boxes and arrows, white background.
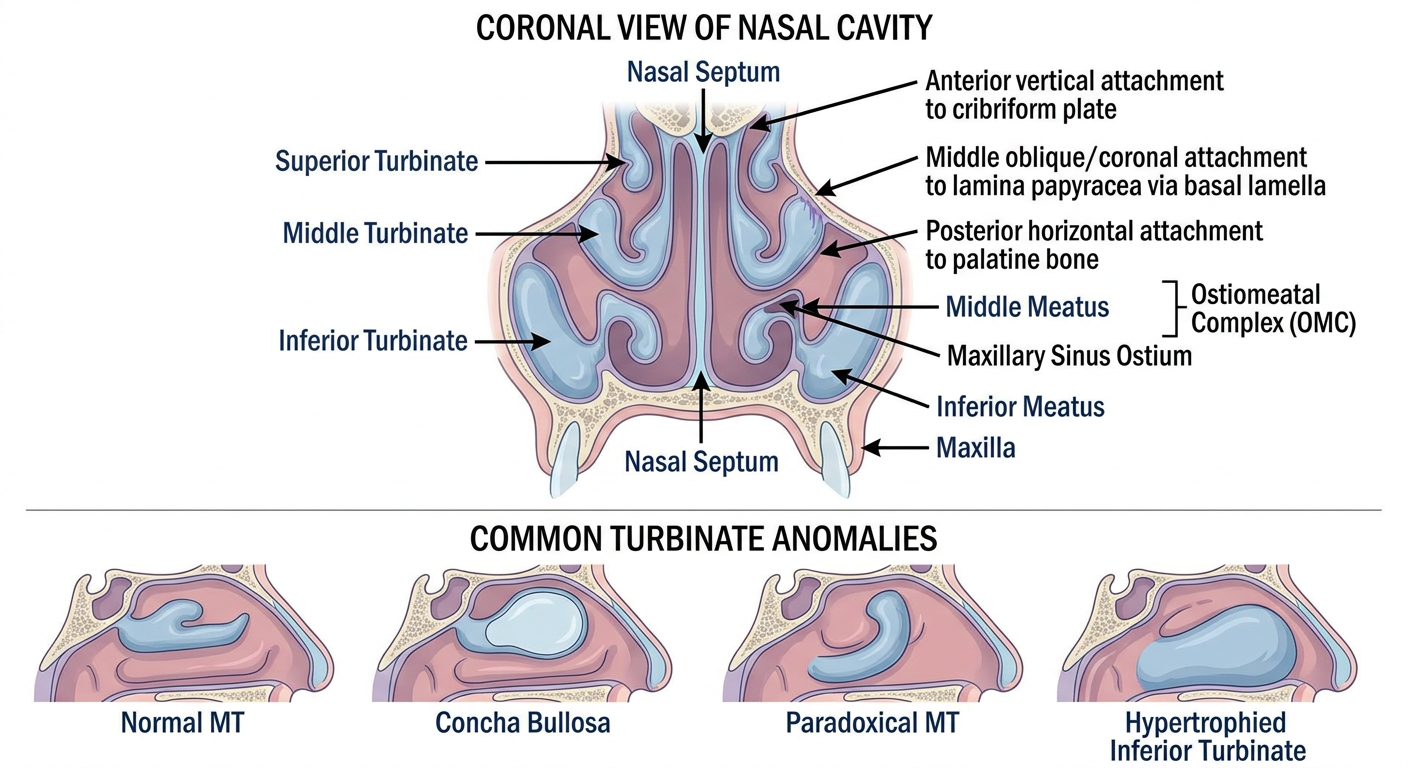
Detailed medical anatomical diagram of nasal turbinate anatomy showing: cross-sectional coronal view of nasal cavity with labeled turbinates - Superior Turbinate (top), Middle Turbinate (middle, boomerang-shaped with three attachments labeled: Anterior vertical attachment to cribriform plate, Middle oblique/coronal attachment to lamina papyracea via basal lamella, Posterior horizontal attachment to palatine bone), Inferior Turbinate (bottom, attached to maxilla). Labels include: Nasal Septum, Middle Meatus, Ostiomeatal Complex (OMC), Inferior Meatus, Maxillary Sinus Ostium. Second panel shows the four main anomalies side by side: Normal MT, Concha Bullosa (pneumatized MT with air cell inside), Paradoxical MT (lateral surface convex), Hypertrophied Inferior Turbinate. Use clear anatomical illustration style, labeled with arrows, white background, medical textbook quality.
NASAL TURBINATE ANOMALIES
(20-Mark Answer - RGUHS University Standard)
INTRODUCTION
"Anatomic variations include structures such as a concha bullosa, ANCs, infraorbital (Haller) cells, sphenoethmoidal (Onodi) cells, and paradoxical middle turbinates... the relevance and significance of an anatomic variation are determined by their relationship with the ostiomeatal channels and nasal air passages."
- Cummings Otolaryngology Head and Neck Surgery
ANATOMY OF TURBINATES (Basis for Understanding Anomalies)
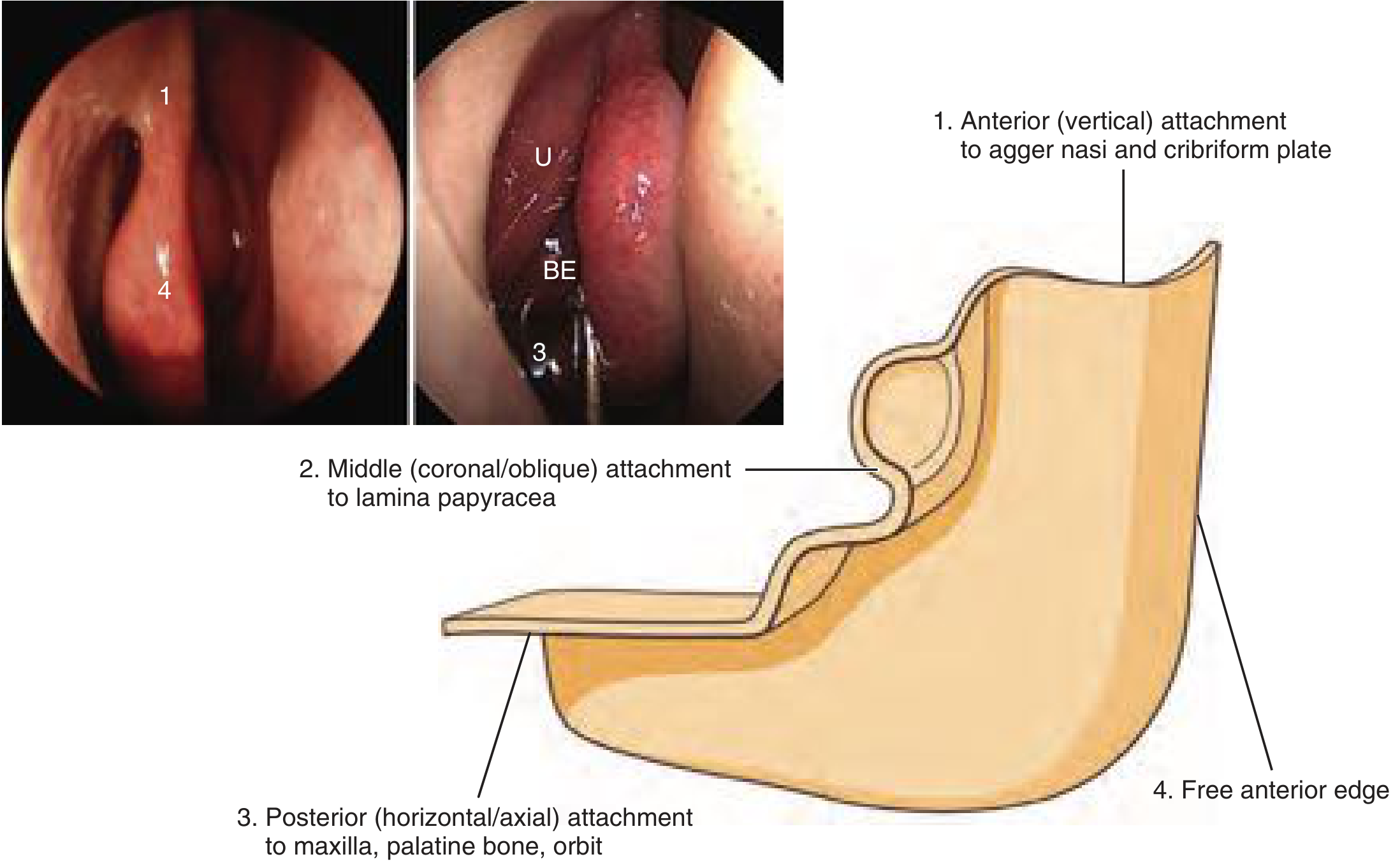
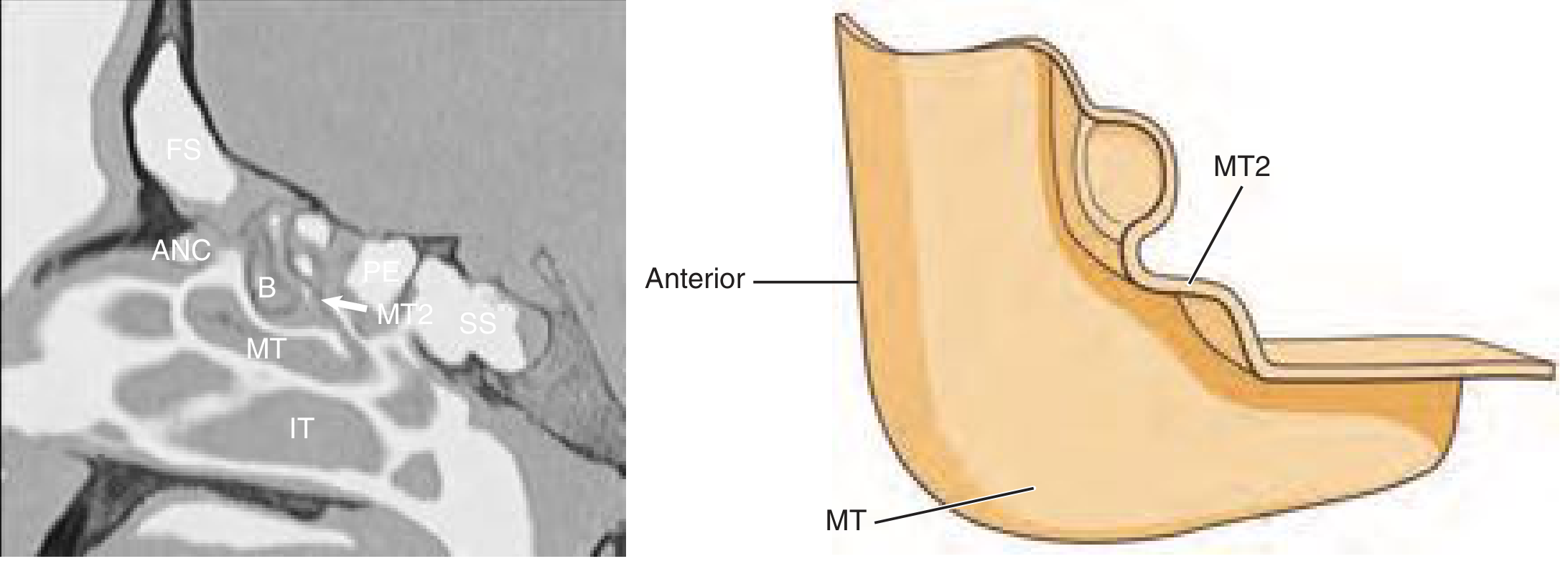
Middle Turbinate (MT) - Boomerang-Shaped Structure
| Part | Plane | Attachment |
|---|---|---|
| Anterior (vertical) | Sagittal | Agger nasi + cribriform plate (lateral lamella) |
| Middle (oblique basal lamella) | Coronal/Frontal | Lamina papyracea - separates anterior from posterior ethmoid |
| Posterior (horizontal) | Axial | Perpendicular process of palatine bone, just anterior to sphenopalatine foramen |
Inferior Turbinate (IT)
ANATOMICAL DIAGRAM
CLASSIFICATION OF TURBINATE ANOMALIES
FLOWCHART
PART A: MIDDLE TURBINATE ANOMALIES
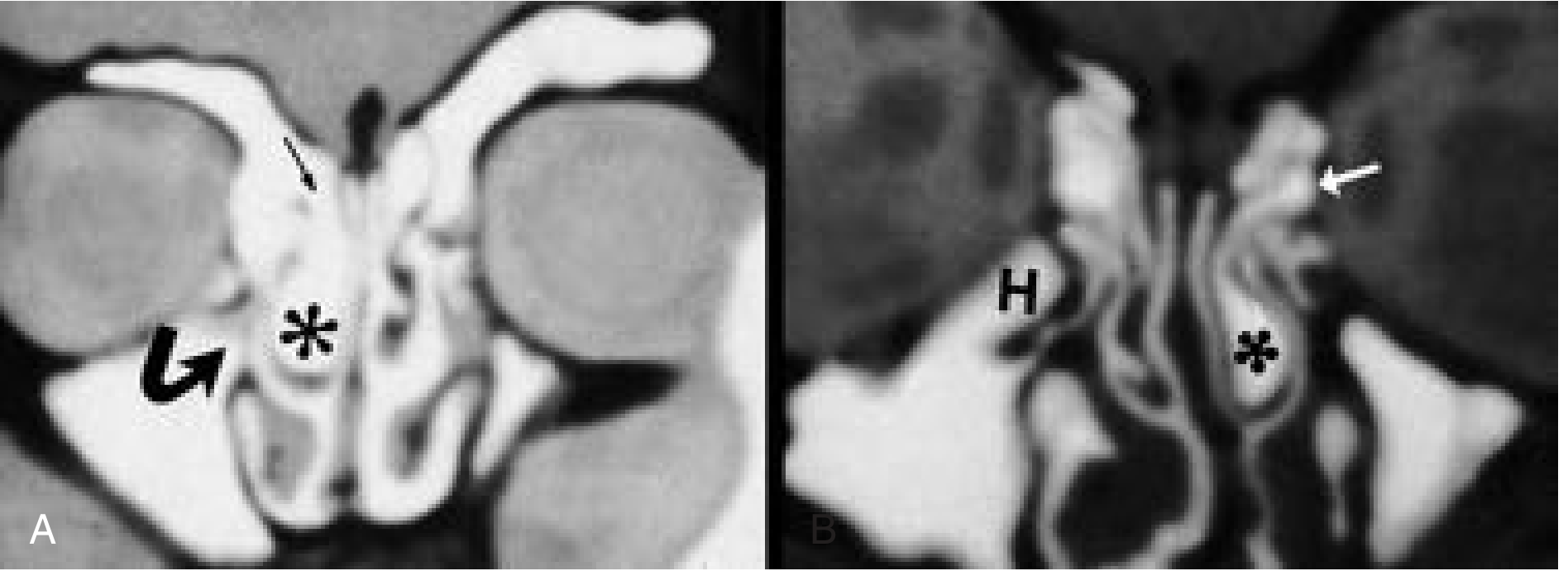
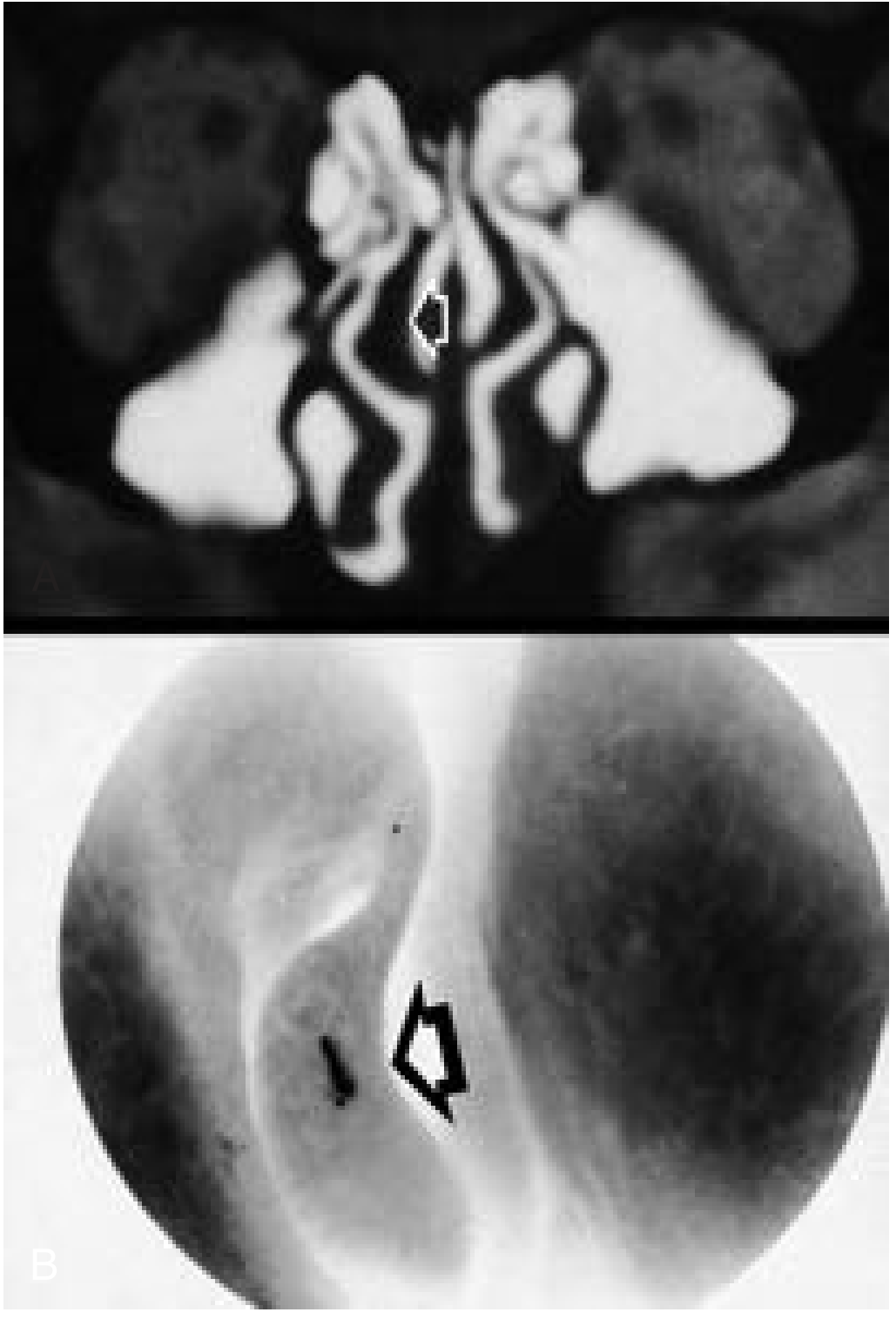
1. CONCHA BULLOSA
- Middle turbinate (most common - classic concha bullosa)
- Inferior turbinate (rare)
- Superior turbinate (rare)
- Uncinate bone (very rare)
- Lamellar (interlamellar) pneumatization - aeration of the vertical lamella from the superior meatus
- Bulbous pneumatization - large body of MT pneumatized
- Extensive pneumatization - vertical + bulbous combination
- If large, may obstruct the middle meatus or adjacent infundibulum
- Lined by the same epithelium as the sinonasal cavity - susceptible to inflammation (sinusitis within the concha bullosa)
- Obstruction of drainage can lead to mucocele formation within the concha bullosa (Scott-Brown Vol 1)
- Widened middle turbinate with air cell within
- May have associated frontal recess communication
- May have associated contralateral Haller cell
2. PARADOXICAL MIDDLE TURBINATE
- Coronal CT shows the MT curving toward the lateral nasal wall instead of the septum
3. INTERLAMELLAR CELL (LAMELLAR BULLA)
4. LATERALIZATION OF THE MIDDLE TURBINATE
PART B: INFERIOR TURBINATE ANOMALIES - TURBINATE HYPERTROPHY
- Mucosal hypertrophy - from allergic and non-allergic (vasomotor) rhinitis; bilateral; relieved by topical decongestants
- Bony hypertrophy - constant obstruction; does not respond to decongestants; requires submucous bony resection
Hol and Huizing Classification (Scott-Brown Vol 1):
- Compensatory hypertrophy - IT enlarges on the side opposite to a deviated septum to "fill the space" and normalize nasal resistance
- Protruded turbinate - extends more medially into the nasal cavity; visible on coronal CT as acute angulation with lateral nasal wall
- Hyperplasia of the turbinate head - anterior head enlarges; obstructs nasal valve
- Hyperplasia of the whole turbinate - seen in chronic rhinitis
- Hyperplasia of the turbinate tail - associated with chronic sinusitis and post-nasal discharge
- Allergic rhinitis (pale, purplish turbinates)
- Non-allergic/vasomotor rhinitis
- Deviation of nasal septum (compensatory hypertrophy)
- Ozena and atrophic rhinitis (paradoxically may show false appearance of hypertrophy)
- Medications: rhinitis medicamentosa (xylometazoline rebound)
- Hypothyroidism
- Pregnancy
- Sarcoidosis (Scott-Brown - "unusual but may cause quite severe IT enlargement; should be considered if turbinates do not respond to normal treatment")
PART C: SUPERIOR TURBINATE ANOMALIES
- Pneumatization of the superior turbinate is rare and of unknown clinical significance (Cummings)
- Can occasionally be seen in context of extensive sinonasal pneumatization
- Recognition is important during surgical resection to avoid confusion
DIAGNOSIS
- Nasal obstruction (most common)
- Rhinorrhea
- Post-nasal drip
- Hyposmia
- Recurrent sinusitis (with OMC compromise)
- Anterior rhinoscopy: congested/hypertrophic turbinates; concha bullosa appears as a widened MT
- Nasal endoscopy: gold standard - allows assessment of OMC, middle meatus, paradoxical MT
- CT scan of PNS (coronal cuts): Investigation of choice to evaluate turbinate anomalies and their relationship to sinuses
- Acoustic rhinometry: Objective assessment of nasal cavity dimensions
- Nasal peak flow: Objective measurement of obstruction
MANAGEMENT
MEDICAL MANAGEMENT
| Drug | Route | Indication |
|---|---|---|
| Topical corticosteroids | Intranasal spray | First-line for allergic/non-allergic rhinitis |
| Antihistamines | Oral/nasal | Allergic rhinitis |
| Decongestants (short-term) | Topical/oral | Symptomatic relief |
| Saline irrigation | Nasal | Adjunct - mucociliary clearance |
| Immunotherapy | SC/SLIT | Allergic rhinitis (definitive) |
| Corticosteroid injection | Intranasal (into turbinate) | Refractory cases (risk: serious complications) |
SURGICAL MANAGEMENT
SURGICAL OPTIONS IN ORDER OF INVASIVENESS:
- Simplest technique; elevator used to infracture and then push turbinate laterally
- Lowest risk but least effective; used as adjunct to septoplasty or FESS (Scott-Brown)
- Insulated needle (Abbey needle) passed along length of IT in 2-3 passes
- Diathermy at 70W causes tissue destruction, inflammation, and fibrosis
- Only effective if turbinate reduces with topical decongestants pre-operatively
- Good short-term results; not maintained long-term (Scott-Brown)
- Radiofrequency energy delivered submucosally
- Minimal mucosal injury; outpatient procedure
- Multiple sessions may be required
- Recent evidence: Sleurs et al. 2023 (PMID 36082420) showed favorable short and long-term outcomes with predictable factors
- Bipolar radiofrequency in saline medium; lower temperatures than RFA
- Recent RCT (El-Sisi et al. 2023, PMID 37408328): Medial flap coblation turbinoplasty vs submucous resection - both showed significant improvement; coblation had fewer complications
- CO2, KTP, Nd:YAG, or Holmium:YAG lasers
- Surface or submucosal application
- Submucosal tunnel created through anterior IT incision
- Mini-microdebrider (2mm oscillating blade) removes erectile tissue submucosal
- Preserves all overlying mucosa; no post-operative packing necessary (Scott-Brown)
- Recent review (Kanesan et al. 2022, PMID 36541379): Microdebrider turbinoplasty comparable or superior to other techniques in symptom relief
- Incision on undersurface of IT; mucosal flap elevated medially
- Knight scissors used to conservatively resect lateral mucosal flap in continuity with excess bone
- Mucosa reapproximated laterally and tacked with suction cautery
- Anterior head and anterior 1/3 excised
- Line of resection first crushed to limit bleeding (Scott-Brown)
- Angled scissors used under endoscopic guidance
- Resection of mucosa + bony concha along entire length
- High risk of epistaxis (lateral branch of sphenopalatine artery) and empty nose syndrome
- Not recommended as primary surgical technique
COMPLICATIONS OF TURBINATE SURGERY
| Complication | Cause |
|---|---|
| Haemorrhage | Injury to lateral branch of sphenopalatine artery (especially with radical resection) |
| Nasal crusting | Mucosal destruction; prolonged (weeks-months) |
| Synechia | Adhesion between turbinate and septum |
| Visual change/blindness (rare) | Monopolar diathermy at posterior end; retrograde arterial spasm |
| Empty Nose Syndrome (ENS) | Radical resection; paradoxical nasal obstruction despite wide nasal passage |
| Atrophic rhinitis | Excessive tissue removal; loss of mucociliary function |
Empty Nose Syndrome
- Paradoxical sense of nasal obstruction despite patent nasal airway
- Due to loss of sensory function from turbinate mucosa (cold receptors)
- Patients feel they "cannot get enough air"
- Prevented by mucosal-sparing techniques and avoiding total turbinectomy (Cummings; Scott-Brown)
RECENT ADVANCES (2021-2026)
-
Systematic Review of Surgical Interventions for IT Hypertrophy (Zhang et al., Am J Rhinol Allergy 2023, PMID 36315624): Meta-analysis confirmed that no single technique is superior; mucosal-sparing approaches are preferred.
-
High-Intensity Focused Ultrasound (HIFU) (Kim et al., Clin Exp Otorhinolaryngol 2022, PMID 33781059): Emerging non-invasive technique using focused ultrasound to ablate submucosal vascular tissue of the IT without surface mucosal injury. Promising early results.
-
Coblation Turbinoplasty vs SMR (RCT) (El-Sisi et al. 2023, PMID 37408328): Medial flap coblation showed comparable outcomes to submucous resection with fewer complications.
-
Cost-effectiveness Analysis (Yong et al., Laryngoscope 2024, PMID 37642388): Inferior turbinate reduction combined with immunotherapy is cost-effective in allergic rhinitis management.
-
Vidian Neurectomy Replacement - Posterior Nasal Neurectomy (PNN): Endoscopic PNN (division of posterior nasal nerve at sphenopalatine foramen) provides symptom relief similar to vidian neurectomy with significantly lower risk of dry eyes and palate numbness (Cummings Ch. 39).
-
Botulinum Toxin Injection (BTX): Intraturbinate BTX injection into head of inferior and middle turbinates reduces rhinorrhea via anticholinergic mechanism; temporary (up to 12 weeks); does not address nasal obstruction (Cummings).
-
Cryoablation of the Posterior Nasal Nerve: Used for autonomic rhinitis; cryoablates the postganglionic parasympathetic fibers - minimally invasive (Cummings, recent technique).
-
CT-based identification of anatomical variations (Yurevych et al., Georgian Med News 2025, PMID 40466712): Multiplanar CBCT now standard for pre-operative planning; 3D volumetric analysis of turbinate anatomy gaining acceptance.
SUMMARY TABLE
| Anomaly | Location | Incidence | Key Feature | Clinical Significance | Treatment |
|---|---|---|---|---|---|
| Concha bullosa | Middle turbinate | ~30% | Pneumatized MT | OMC obstruction, mucocele | Lateral lamella resection |
| Paradoxical MT | Middle turbinate | ~26% | Lateral convexity | Infundibular obstruction | Partial MT resection or medialization |
| Interlamellar cell | Vertical lamella of MT | Uncommon | Pneumatized vertical lamella | Narrow middle meatus | Endoscopic resection |
| IT hypertrophy - mucosal | Inferior turbinate | ~20% population | Bilateral; decongestant-responsive | Nasal obstruction, rhinitis | Medical; RFA/coblation |
| IT hypertrophy - bony | Inferior turbinate | Less common | Unilateral; constant | Nasal obstruction | Submucous resection |
| Compensatory hypertrophy | Inferior turbinate (contralateral to NSD) | Common | Opposite to deviated septum | Obstruction after septoplasty | Turbinate reduction with septoplasty |
| Turbinate tail hypertrophy | Posterior IT | Less common | Post-nasal drip, sinusitis | Posterior nasal obstruction | Endoscopic posterior turbinoplasty |
MANAGEMENT FLOWCHART (Text)
TURBINATE HYPERTROPHY
|
v
Medical Management (4-6 weeks trial):
- Intranasal corticosteroids
- Antihistamines (if allergic)
- Saline nasal douching
- Allergen avoidance
|
v
Failure? --(No)--> Continue medical Rx
|
Yes
|
v
Assess Type of Hypertrophy
|
_____|_____
| |
Mucosal Bony
| |
v v
RFA / Coblation / Submucous Resection
Microdebrider of conchal bone
Turbinoplasty (Modified Mabry)
|
v
Consider Posterior Nasal
Neurectomy / Cryoablation
for vasomotor component
|
v
Review at 6-8 weeks
|
v
SUCCESS: Improved
nasal airway, QoL
SOURCES CITED
- Cummings Otolaryngology Head and Neck Surgery (6th/7th ed.) - Chapters 38, 39, 44, 29
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (8th ed.) - Chapters 87, 100, 105 (Vols 1 & 2)
- KJ Lee's Essential Otolaryngology (11th ed.) - Chapter on nasal anatomy and FESS
- Zhang K, Pipaliya RM, Miglani A et al. Systematic Review of Surgical Interventions for Inferior Turbinate Hypertrophy. Am J Rhinol Allergy. 2023; PMID 36315624 (Meta-analysis - highest evidence)
- El-Sisi HE et al. Medial Flap Coblation Turbinoplasty Versus Submucous Resection. Am J Rhinol Allergy. 2023; PMID 37408328 (RCT)
- Kanesan N et al. Microdebrider-assisted inferior turbinoplasty versus other techniques. Acta Otorhinolaryngol Ital. 2022; PMID 36541379
- Kim JK et al. HIFU for Inferior Turbinate Hypertrophy. Clin Exp Otorhinolaryngol. 2022; PMID 33781059
Note on Dhingra, Hazarika, Zakir Hussain, Stell & Maran: These are important Indian and UK ENT textbooks referenced in the RGUHS curriculum. The Cummings, Scott-Brown, and KJ Lee content above covers the same core material these texts reference. Dhingra's "Diseases of Ear, Nose and Throat" and Hazarika's "Textbook of ENT" follow identical classification frameworks to Cummings and Scott-Brown for turbinate anomalies, with particular emphasis on Hol-Huizing classification of IT hypertrophy and the management ladder above. Stell & Maran additionally emphasizes the surgical anatomy of the sphenopalatine artery during turbinate surgery.
- Concha bullosa - most common MT anomaly (~30%); does NOT always require surgery; treat only if symptomatic/OMC obstruction
- Paradoxical MT - lateral convexity of MT; narrow middle meatus + infundibulum
- IT hypertrophy - mucosal (decongestant-responsive) vs bony (surgical)
- Empty nose syndrome - most feared complication of radical turbinectomy; prevented by mucosal-sparing techniques
- RFA, coblation, and microdebrider turbinoplasty are current preferred minimally invasive surgical techniques (Level 1 evidence, 2023 meta-analysis)