Coarctation of aorta causes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from the medical library. Here is the full answer:
Coarctation of the Aorta - Causes & Pathology
Definition
Coarctation of the aorta (CoA) is a congenital narrowing (constriction) of the aorta. It is one of the more common congenital heart defects (CHD), accounting for ~10% of all CHDs. It occurs twice as often in males as in females, though females with Turner syndrome are also frequently affected.
Types / Forms
There are two classic anatomical types:
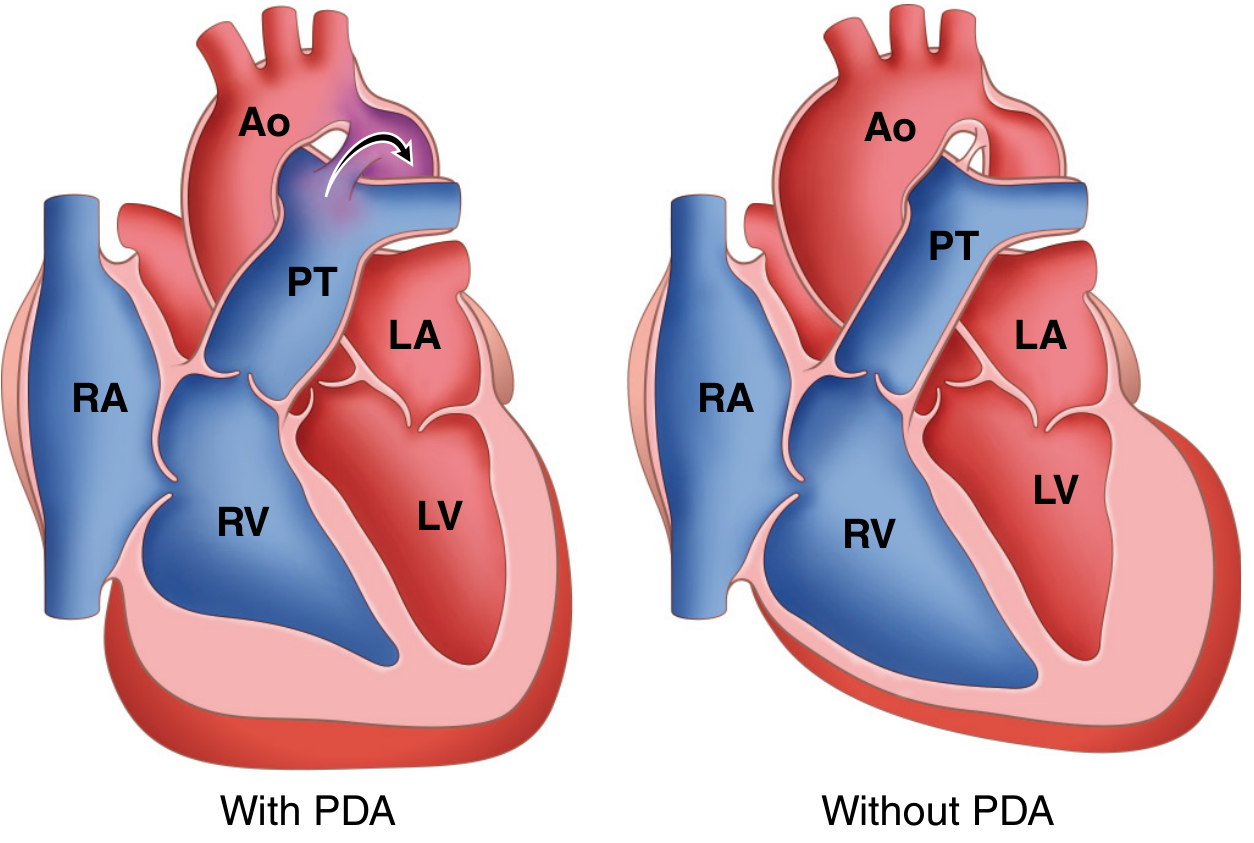
1. Preductal ("Infantile") Form
- Narrowing is proximal to the ductus arteriosus (between the left subclavian artery and the ductus)
- Associated with a patent ductus arteriosus (PDA)
- Characterized by tubular hypoplasia of the aortic arch
- The PDA is the main source of (deoxygenated) blood delivered to the distal aorta
- Pulmonary trunk is dilated; right ventricle is hypertrophied (it now perfuses the lower body through the PDA)
2. Postductal ("Adult") Form
- A discrete ridge-like infolding of the aorta adjacent to the closed ductus arteriosus (ligamentum arteriosum)
- More common form
- The constricted segment is made up of smooth muscle and elastic fibers from the aortic media
- Proximal to the coarctation: aortic arch and branch vessels are dilated
- Left ventricle is hypertrophied from chronic pressure overload
Note: In ~90% of cases, the coarctation is directly opposite the ductus arteriosus (juxtaductal position).
Embryological Causes (Three Main Theories)
From The Developing Human - Clinically Oriented Embryology:
-
Ductal muscle theory: During formation of the aortic arch, smooth muscle tissue from the ductus arteriosus is incorporated into the aortic wall. When the ductus constricts at birth, the ductal muscle within the aorta also constricts, producing the coarctation.
-
Abnormal involution theory: Abnormal involution (regression) of a small segment of the left dorsal aorta occurs. This stenotic segment later migrates cranially with the left subclavian artery, forming the coarctation.
-
Aortic isthmus theory: During fetal life, the segment of the aortic arch between the left subclavian artery and the ductus arteriosus is normally narrow because it carries very little blood (most flow is via the ductus). After birth, when the ductus closes, this narrow isthmus should enlarge. If the narrowing persists, it becomes a coarctation.
Genetic / Syndromic Causes
| Association | Notes |
|---|---|
| Turner syndrome (45,X) | Most common genetic association; ~35% of Turner females have CoA |
| Bicuspid aortic valve | Present in 50-70% of CoA cases - most common associated defect |
| Other CHDs | ASD, VSD, aortic stenosis, mitral regurgitation |
| Berry aneurysms (circle of Willis) | Also associated with CoA |
Pathophysiology / Hemodynamic Consequences
| Situation | Consequence |
|---|---|
| Above coarctation | Hypertension in upper extremities |
| Below coarctation | Hypotension, weak pulses, claudication, coldness in lower limbs |
| Collateral circulation | Enlarged intercostal and internal mammary arteries - produces rib notching on X-ray |
| Preductal + PDA | Differential cyanosis: lower body cyanosis (deoxygenated blood from PDA) |
| LV | Concentric hypertrophy due to pressure overload (postductal form) |
Clinical Features Summary
- Preductal (infantile): Presents at birth or early neonatal period with lower-body cyanosis and cardiac failure. Critical - most die without intervention. Prostaglandin E2 given to keep PDA open.
- Postductal (adult): Often asymptomatic until adulthood. Classic findings:
- Upper extremity hypertension
- Weak/absent femoral pulses
- Radiofemoral delay
- Rib notching on CXR
- Systolic murmur (+ sometimes thrill)
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Ch. 12 (Cardiovascular)
- Robbins & Kumar Basic Pathology, Ch. 9
- The Developing Human - Clinically Oriented Embryology, Ch. 13
What are the diagnostic findings and imaging for CoA?
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks (Braunwald's Heart Disease, Grainger & Allison's Diagnostic Radiology, Greenfield's Surgery, and others). Here is the complete answer:
Diagnostic Findings and Imaging in Coarctation of the Aorta
1. Clinical Diagnostic Findings
Blood Pressure - The Key Clinical Clue
The single most important diagnostic finding is a blood pressure differential between the upper and lower limbs:
- Systolic BP gradient ≥20 mmHg between the right arm and lower limb indicates significant coarctation
- Upper extremity hypertension with weak/absent femoral pulses and lower extremity hypotension
- Brachial-femoral delay - femoral pulse arrives later than the brachial pulse
- Note: Left arm BP may be misleadingly low if the left subclavian artery was involved in or sacrificed during repair
Physical Examination Signs
| Finding | Detail |
|---|---|
| Upper limb hypertension | Most common presenting finding in children/adults |
| Reduced/absent femoral pulses | Characteristic; pulses are weak and delayed |
| Radiofemoral delay | Radial pulse arrives before femoral |
| Systolic murmur | Best heard over the back/interscapular area |
| Continuous interscapular murmur | Suggests collateral arterial flow |
| Lower limb claudication/coldness | Arterial insufficiency below coarctation |
| Hypertensive retinopathy | On fundoscopy in longstanding cases |
Neonatal/Infant Presentation
- Shock, severe metabolic acidosis, oliguria, diminished distal pulses after ductal closure
- Irritability, tachypnea, poor feeding
- Differential cyanosis (preductal form): lower body cyanosis, upper body pink
2. ECG Findings
- Left ventricular hypertrophy (LVH) - due to chronic pressure overload (postductal form)
- Left atrial enlargement
- LV strain pattern - in neonates with severe obstruction
- RV hypertrophy - in preductal form (RV perfuses lower body via PDA)
3. Chest X-Ray (CXR) Findings
The CXR is classically abnormal in older children and adults:
"Figure 3" Sign (most specific CXR sign)
- Formed by the silhouette of the dilated aortic arch/left subclavian artery (pre-stenotic dilatation) above and the post-stenotic dilatation of the descending aorta below, with the coarctation notch in between
- Creates the shape of the number "3" on the left mediastinal border
Rib Notching (Roesler's sign)
- Most characteristic plain film finding in adults
- Pressure erosion of the inferior surfaces of ribs 3-9 (usually bilateral but asymmetric)
- Caused by enlarged, tortuous intercostal collateral arteries
- Ribs 1-2 are spared (intercostals here arise from the costocervical trunk, proximal to the coarctation)
- Takes several years to develop - absent in infants and young children
- Can be unilateral if one subclavian artery arises distal to the coarctation
Other CXR Features
- Cardiomegaly (especially in neonates and older adults)
- Pulmonary venous congestion (in neonates with heart failure)
- Prominent ascending aorta (especially with associated bicuspid aortic valve)
- Poorly visible aortic knuckle
- Enlarged internal mammary artery shadow behind sternum (lateral view)

4. Echocardiography
- Usually the primary confirmatory modality, especially in neonates and infants
- 2D echo: Demonstrates narrowing of the aorta at the coarctation site
- Color Doppler: Turbulent flow in the descending aorta at the coarctation site; aliasing jet
- Continuous-wave (CW) Doppler: Elevated peak velocity across coarctation (>3.5 m/sec suggests significant obstruction); diastolic tail - flow persists throughout diastole, indicating severe coarctation
- Suprasternal notch view: Shows the double envelope (proximal aortic flow + high-velocity coarctation jet)
- Modified Bernoulli equation applied to peak velocity estimates pressure gradient
- Also assesses: LV function, LV mass/hypertrophy, bicuspid aortic valve, other associated defects
- Limitation: Can be technically difficult in older children and adults (poor acoustic window)
Caution: When extensive collateral circulation is present, Doppler gradient may underestimate the true severity of coarctation.
5. MRI / Cardiac MRI (CMR) - Modality of Choice
MRI is the imaging technique of choice for both infantile and adult coarctation, and for post-treatment follow-up.
What MRI Provides:
- Morphological: T1-weighted spin-echo shows the whole aorta, major branches, and larger collateral vessels
- Functional: Cine phase-contrast imaging visualizes turbulence through the stenosis
- Gradient quantification: Phase-contrast MRI quantifies the pressure gradient across the coarctation
- Collateral flow assessment: Measures flow in proximal vs. descending aorta; the increment = collateral contribution
- 3D gadolinium-enhanced MRA: Provides high anatomical detail - shows length of narrowing, arch involvement, post-stenotic dilatation
- LV assessment: LV mass (indirect marker of increased afterload), function, and volumes
- Aortic root: Detects dilatation associated with bicuspid valve, aortic regurgitation/stenosis
Key Imaging Goals on CMR (Grainger & Allison):
- Location and degree of stenosis + length of coarctation segment
- Aortic root involvement and post-stenotic dilatation
- Aortic valve assessment (often bicuspid)
- Delineation of collateral vessels
- Head and neck vessel anatomy
- Ventricular function, volume, and LV mass
- Post-repair: re-coarctation or pseudoaneurysm
6. CT Angiography (CTA)
- Also provides excellent anatomical detail of the coarctation, arch, and collaterals
- Used sparingly in children due to radiation dose
- Strongest role: Follow-up of stent-graft placement - CT better than MRI when metal artefact from stent hampers MR visualisation (assesses in-stent restenosis, stent fracture)
- Detects complications: restenosis, aneurysm, collateral supply
- The role of CT vs. MRI is still debated; MRI preferred when no stent is present
7. Cardiac Catheterization / Angiography
- Historically the gold standard but now rarely needed for diagnosis
- Current role: Reserved for intervention (balloon angioplasty, stent placement) or investigation of associated cardiac abnormalities
- Can cross the coarctation from the femoral artery (or brachial artery if femoral approach fails)
- Multiple angiographic views needed due to asymmetry of stenosis
- Invasive peak-to-peak gradient ≥20 mmHg = threshold for intervention in adults
8. Fetal Diagnosis
- Coarctation can be suspected on fetal echocardiography (disproportion between left and right heart structures), though it can be difficult to confirm prenatally as the aortic isthmus normally carries reduced flow in fetal life
Summary Table: Investigations in CoA
| Investigation | Key Findings |
|---|---|
| BP measurement (4 limbs) | Upper > lower; gradient ≥20 mmHg |
| ECG | LVH, LV strain, LA enlargement |
| CXR | Rib notching (ribs 3-9), "figure 3" sign |
| Echocardiography | Narrowing site, CW Doppler gradient, diastolic tail, LVH |
| MRI/CMR | Modality of choice - full anatomy, gradient, collaterals, LV mass |
| CT angiography | Excellent anatomy; best for post-stent follow-up |
| Cardiac catheterization | Invasive gradient; needed for intervention |
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th Ed., Ch. 82
- Grainger & Allison's Diagnostic Radiology, Ch. 17
- Mulholland and Greenfield's Surgery, Ch. 81
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, Ch. 12
Give me clinical x ray images
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are all the clinical imaging findings for CoA from authoritative textbooks:
Coarctation of the Aorta - Clinical Imaging Gallery
Image 1: CXR - Rib Notching (Subtle)
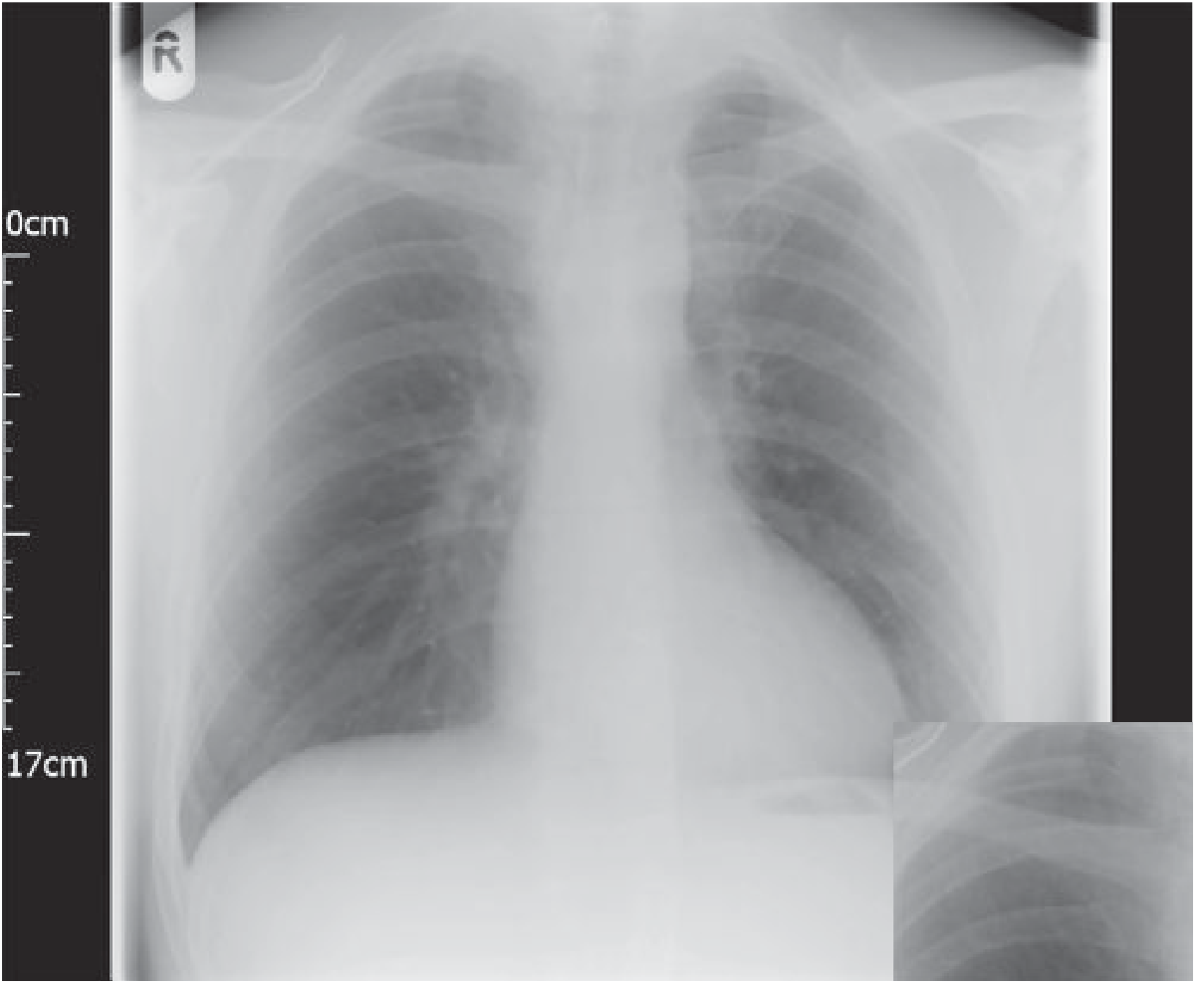
Fig. 3.3 - PA chest radiograph showing subtle inferior rib notching due to enlarged collateral intercostal vessels. The magnified inset (bottom right) clearly demonstrates the notches along the inferior rib borders (arrows).
- Grainger & Allison's Diagnostic Radiology
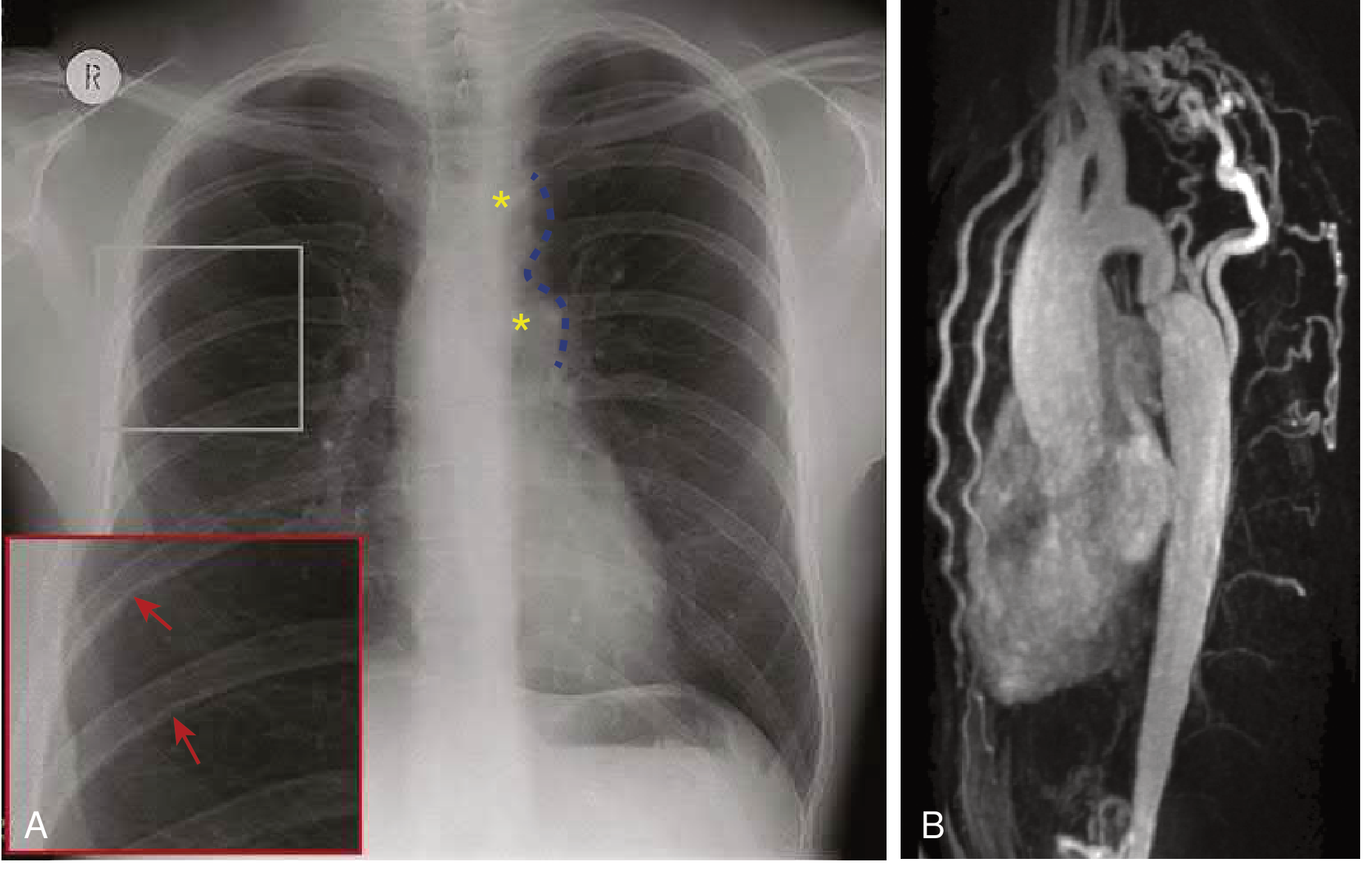
Image 2: CXR + "Figure 3" Sign + MRI Angiography
Fig. 82.34 - (A) PA CXR showing:
- Rib notching (red arrows) at ribs 3-5 bilaterally
- "Figure 3" sign (blue dashed outline, yellow asterisks) = pre-stenotic dilatation of distal arch/dilated left subclavian artery + post-stenotic dilatation of descending aorta
(B) CMR contrast-enhanced angiography confirming tight coarctation with extensive collateral vessels (tortuous intercostal and internal mammary arteries).
- Braunwald's Heart Disease, 15th Ed.
Image 3: CXR - Bilateral Rib Notching (Pronounced)
Fig. 17.56 - PA CXR with well-established CoA showing:
- Bilateral rib notching on the inferior margins of multiple ribs
- Poorly visible aortic knuckle (the coarctation flattens the normal aortic prominence)
- Grainger & Allison's Diagnostic Radiology
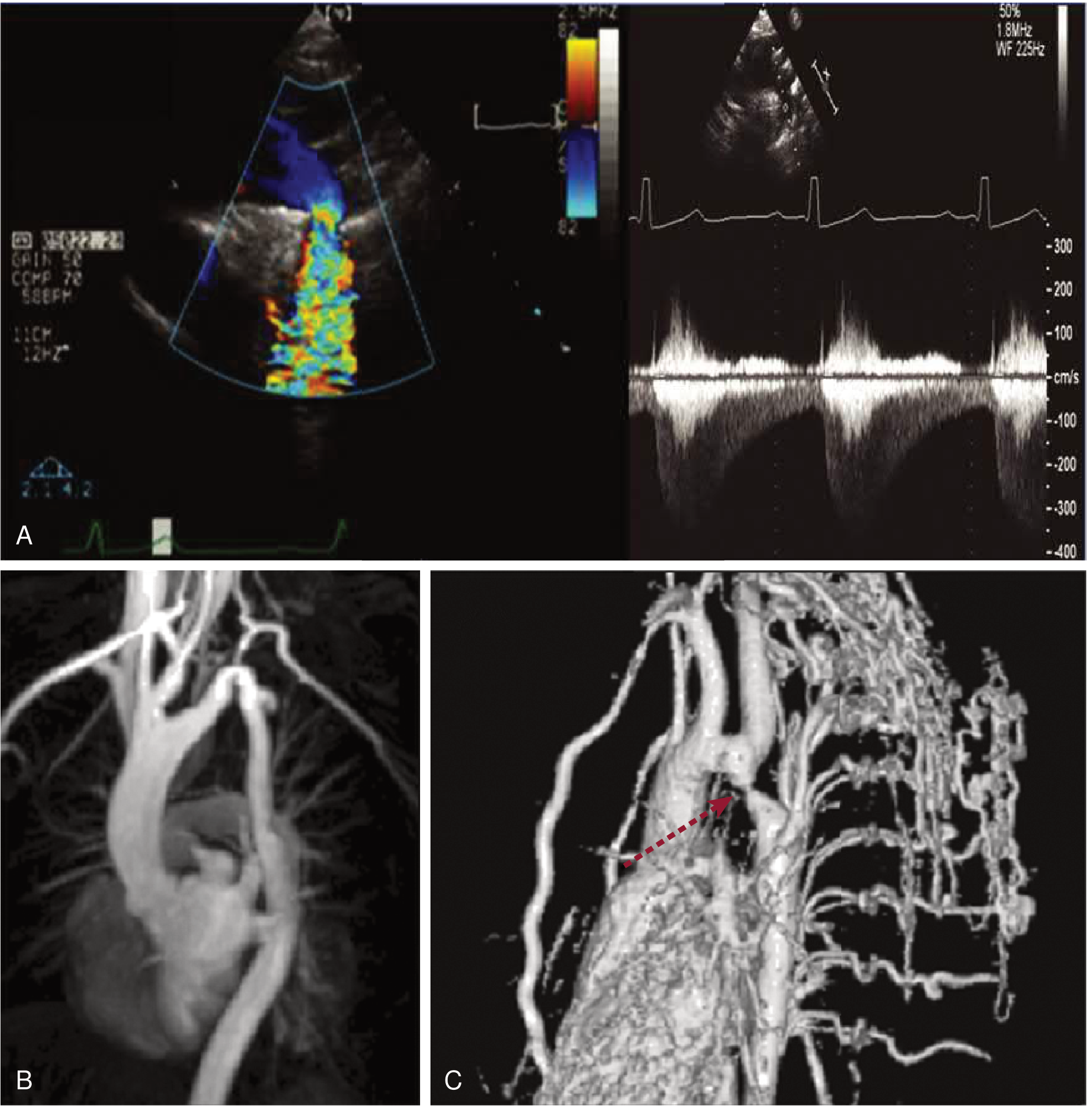
Image 4: Multi-Modal Panel - CXR + MRI + 3D CTA + Doppler Echo
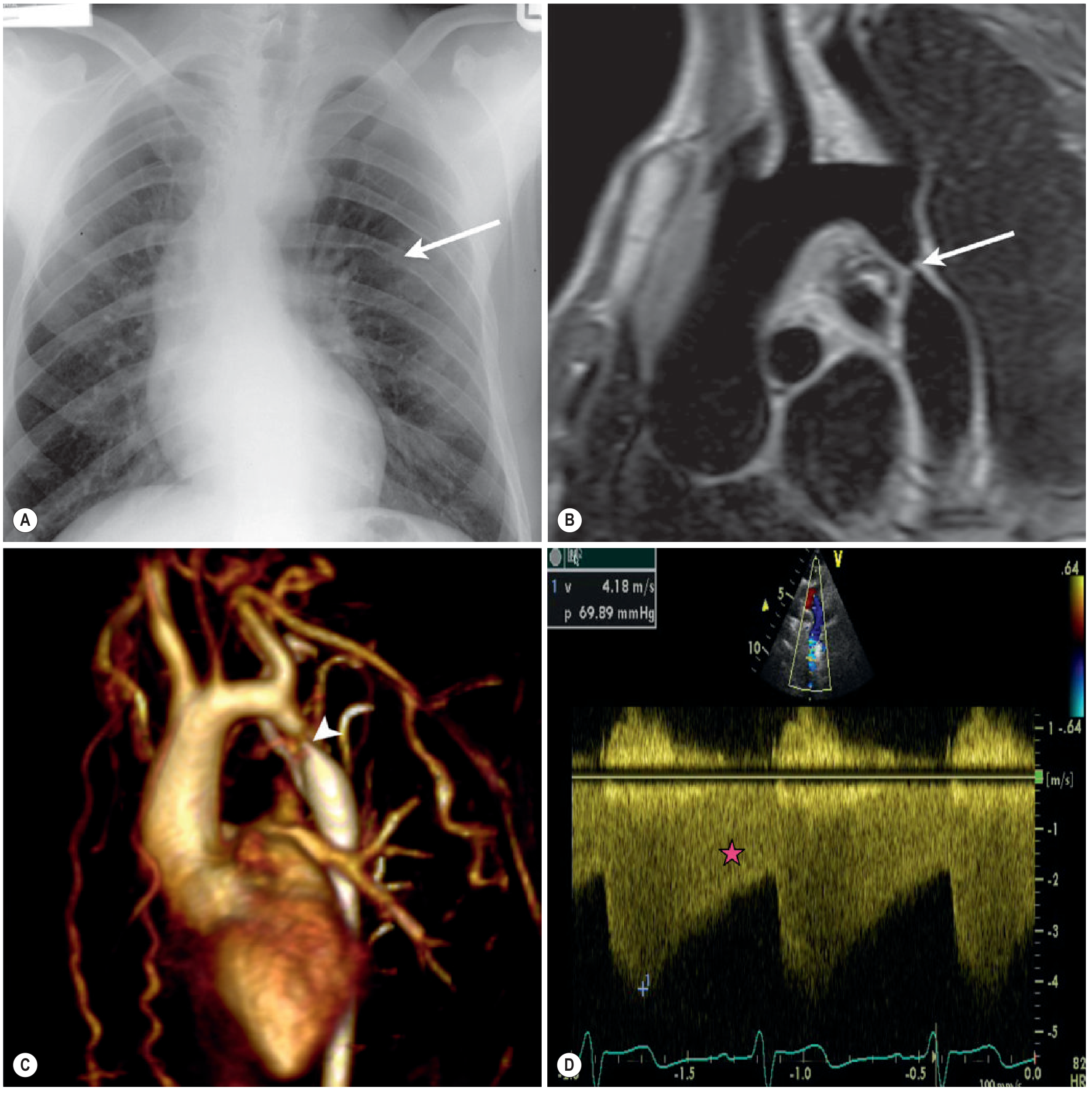
Fig. 13.8 - Severe Coarctation of the Aorta:
| Panel | Modality | Finding |
|---|---|---|
| (A) | PA CXR | Bilateral rib notching (white arrow) from collateral circulation |
| (B) | Black-blood MRI (oblique sagittal) | Tight discrete coarctation at juxtaductal position (white arrow) |
| (C) | 3D MRA volume-rendered | Tight coarctation (arrowhead) + multiple large collateral vessels |
| (D) | CW Doppler echo | Peak velocity 4.18 m/s = gradient 69.89 mmHg; diastolic tail (pink star) = severe obstruction |
- Grainger & Allison's Diagnostic Radiology
Image 5: Echocardiography - Suprasternal Arch View + Color Doppler
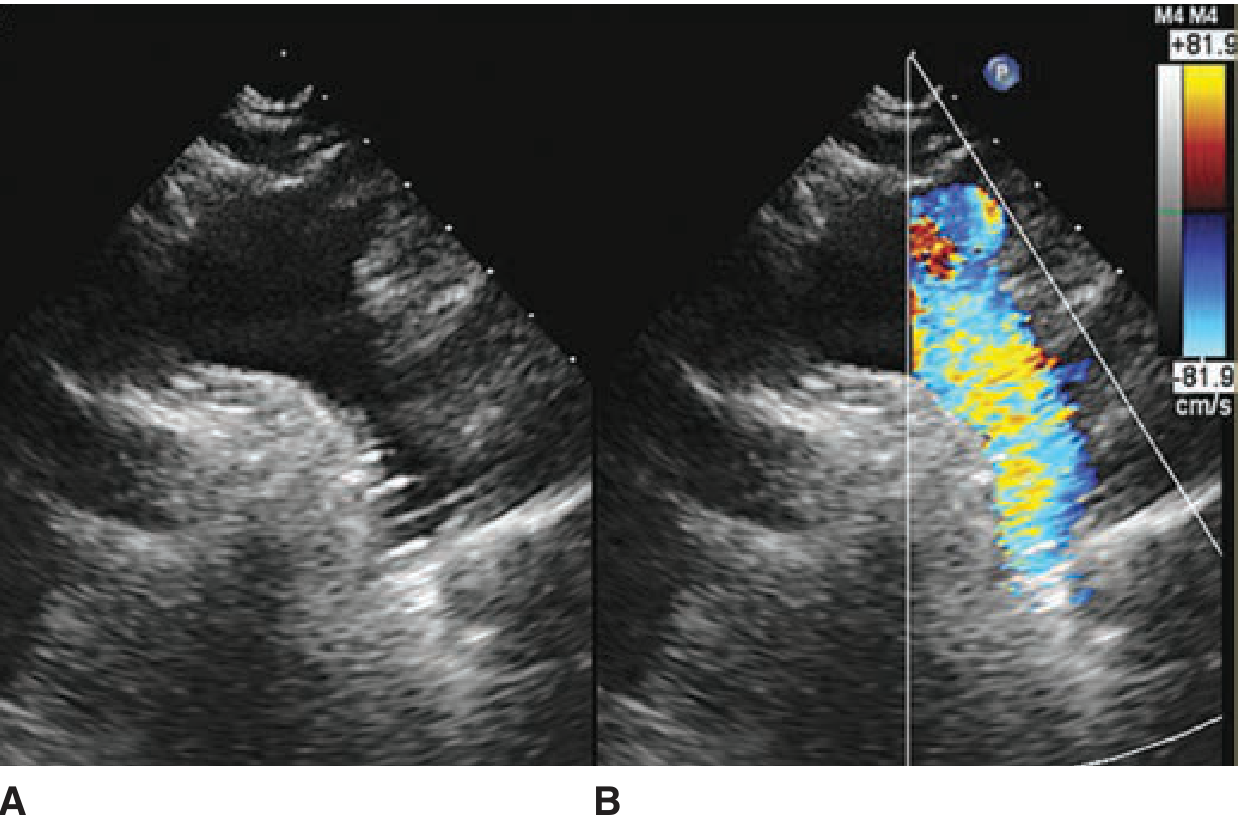
Fig. 68-17 - Transthoracic echocardiography from suprasternal notch view:
- (A) 2D image of the aortic arch - shows the arch anatomy
- (B) Color flow Doppler overlay - turbulent aliased flow (mosaic pattern of red/yellow/blue) at the coarctation site in the descending aorta
- Fuster and Hurst's The Heart, 15th Ed.
Summary of What to Look for on CXR
| Sign | Location | Significance |
|---|---|---|
| Rib notching | Inferior surface, ribs 3-9 | Collateral intercostal arteries (takes years to develop) |
| "Figure 3" sign | Left mediastinal border | Pre + post-stenotic aortic dilatation flanking the coarctation |
| Cardiomegaly | Cardiac silhouette | LV hypertrophy / failure |
| Flat/absent aortic knuckle | Aortic arch region | Obliterated by coarctation indentation |
| Internal mammary shadow | Behind sternum (lateral CXR) | Enlarged collateral vessels |
This is a shared conversation. Sign in to Orris to start your own chat.