10 common ECG findings with explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks (Harrison's, Goldman-Cecil, Tintinalli's, Medical Physiology). Here is the detailed answer:
10 Common ECG Findings - With Full Explanations
1. ST-Segment Elevation (STEMI)
What it looks like: ST segment elevated ≥1 mm above baseline in ≥2 contiguous leads (≥2 mm in V1-V3).
Mechanism: Transmural myocardial injury causes persistent depolarization in the affected zone, so its cells fail to fully repolarize - this creates a current of injury that shifts the ST segment upward.
Lead localization:
| Territory | Elevated leads |
|---|---|
| Anterior | V1-V4 |
| Inferior | II, III, aVF |
| Lateral | I, aVL, V5-V6 |
| Posterior | Tall R in V1-V2, ST depression anteriorly |
Clinical meaning: Acute transmural coronary occlusion - treat as STEMI, activate catheterization lab emergently.
(Tintinalli's Emergency Medicine, Table 49-4)
2. ST-Segment Depression
What it looks like: ST segment displaced ≥0.5-1 mm below baseline (horizontal or downsloping is more significant than upsloping).
Mechanism: Subendocardial ischemia (innermost layer is most vulnerable because coronary perfusion pressure is lowest there). The subendocardium depolarizes normally but repolarizes abnormally.
Patterns:
- Horizontal/downsloping ST depression = ischemia or NSTEMI
- Upsloping ST depression = less specific, seen in tachycardia
- ST depression in V1-V4 with inferior STEMI = reciprocal change or posterior MI
Clinical meaning: Active myocardial ischemia, NSTEMI, or reciprocal changes. ST depression ≥1 mm in ≥2 contiguous leads in the context of chest pain indicates high-risk ACS.
(Harrison's Principles of Internal Medicine 22E)
3. Atrial Fibrillation (AF)
What it looks like:
- No identifiable P waves (replaced by chaotic fibrillatory baseline)
- Irregularly irregular ventricular rhythm
- Narrow QRS (unless aberrant conduction or pre-excitation present)
- Ventricular rate typically 100-180 bpm if uncontrolled
Mechanism: Multiple re-entrant wavelets circulate chaotically through the atria, producing 350-600 disorganized atrial impulses per minute. The AV node acts as a gatekeeper, conducting impulses randomly - hence the irregularly irregular rhythm.
Clinical meaning: Most common sustained arrhythmia. Risk of thromboembolism (stroke), hemodynamic compromise, tachycardia-induced cardiomyopathy. CHA₂DS₂-VASc score guides anticoagulation.
(Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine)
4. Right Bundle Branch Block (RBBB)
What it looks like:
- QRS duration ≥ 120 ms (complete RBBB)
- rSR' (or rsR') pattern in V1 - the classic "M-shape"
- Wide, slurred S wave in leads I and V6
- Discordant ST/T changes in V1-V2
Mechanism: Conduction block in the right bundle branch means the right ventricle is depolarized late via slow cell-to-cell spread from the left ventricle. This delayed rightward terminal force produces the characteristic R' in V1 and terminal S in lateral leads.
Clinical meaning: Can be a normal variant (isolated RBBB), or associated with right heart strain (PE, RVH), myocarditis, or structural heart disease. New RBBB with chest pain warrants investigation.
(Goldman-Cecil Medicine, Table 42-3)
5. Left Bundle Branch Block (LBBB)
What it looks like:
- QRS duration ≥ 120 ms
- Broad, notched (W-shaped) R wave in V5-V6, I, aVL (no septal q waves)
- rS or QS complex in V1 (broad, deep S)
- Discordant ST-T changes throughout V1-V6
Mechanism: The left bundle branch normally activates the septum first (left-to-right). When blocked, both septum and left ventricle depolarize via slow myocardial spread from the right. This reverses normal septal activation and delays overall LV activation, producing wide, bizarre QRS complexes.
Clinical significance: LBBB is almost always pathological. New LBBB with chest pain is treated as a STEMI equivalent (Sgarbossa criteria help identify MI in LBBB). Underlying causes include CAD, cardiomyopathy, hypertension, and aortic stenosis.
(Goldman-Cecil Medicine; Harrison's Principles)
ECG example (RBBB - top; LBBB - bottom):
6. Left Ventricular Hypertrophy (LVH)
What it looks like:
- Sokolow-Lyon criteria: SV1 + RV5 (or RV6) > 35 mm
- RaVL > 20 mm (women) or > 28 mm (men)
- ST-segment depression + T-wave inversion in lateral leads (I, aVL, V5-V6) = "strain pattern"
- Left axis deviation and left atrial enlargement often coexist
Mechanism: Hypertrophied LV muscle mass generates larger electrical forces oriented leftward and posteriorly. The increased muscle and altered geometry also cause secondary repolarization abnormalities (the "strain" pattern), which are not ischemia per se but reflect altered action potential duration.
Clinical meaning: A major non-invasive marker of increased cardiovascular risk, including sudden cardiac death. Seen in hypertension, aortic stenosis, and hypertrophic cardiomyopathy. Echocardiography is more definitive for diagnosis.
(Harrison's Principles of Internal Medicine 22E)
7. Pathological Q Waves (Old Myocardial Infarction)
What it looks like:
- Q wave ≥ 0.04 s (1 small box) wide
- Depth ≥ 25% of the R wave amplitude in the same lead
- Present in the territory corresponding to the infarct
Mechanism: Dead myocardium does not generate electrical activity. The overlying electrode therefore "sees" depolarization moving away from it (from the opposite ventricular wall), producing an initial negative deflection - the pathological Q wave. This is a window effect through electrically silent scar tissue.
Normal vs pathological: Small septal q waves in I, V5-V6 are normal (septal depolarization). Q waves in aVR are normal. Pathological Q waves appear in infarct territories.
Clinical meaning: Marker of prior full-thickness MI. Can persist for years. New Q waves suggest acute or evolving infarction.
(Tintinalli's Emergency Medicine)
8. Prolonged QT Interval
What it looks like:
- Corrected QT (QTc) > 450 ms in men, > 460 ms in women (using Bazett's formula: QTc = QT / √RR)
- T wave may be broad, notched, or biphasic
Mechanism: The QT interval reflects ventricular repolarization duration. Prolongation means the ventricular action potential is longer than normal. This creates a vulnerable window in which early afterdepolarizations can trigger spontaneous depolarization - the substrate for Torsades de Pointes (polymorphic VT).
Causes:
- Congenital: Long QT syndromes (LQTS types 1-3, channelopathies affecting Na⁺/K⁺ channels)
- Acquired: Drugs (antipsychotics, macrolides, quinolones, sotalol), hypokalemia, hypomagnesemia, hypocalcemia, hypothyroidism
Clinical meaning: Prolonged QTc predisposes to life-threatening Torsades de Pointes and ventricular fibrillation. QTc > 500 ms is considered high risk.
(Fuster and Hurst's The Heart, 15th Edition)
9. First-Degree AV Block
What it looks like:
- PR interval > 200 ms (> 1 large box) in every beat
- Every P wave is followed by a QRS (1:1 conduction maintained)
- Regular rhythm
Mechanism: Slowed conduction through the AV node (most common site) or, less often, through the His-Purkinje system. The impulse is simply delayed, not blocked.
Clinical meaning: Often benign - seen in athletes, with vagal tone, digoxin use, or myocarditis. In isolation it requires no treatment, but a new prolonged PR should prompt evaluation for myocarditis (e.g., Lyme disease), ischemia, or drug effects.
(Medical Physiology - Boron & Boulpaep)
10. Right Ventricular Strain (Acute Cor Pulmonale / Pulmonary Embolism Pattern)
What it looks like:
- Sinus tachycardia (most common finding in PE)
- S1Q3T3 pattern: Prominent S wave in lead I, Q wave in lead III, T-wave inversion in lead III
- Right axis deviation
- New RBBB
- T-wave inversions in V1-V4
- ST changes simulating anterior ischemia
Mechanism: Acute RV pressure overload (from PE, severe hypoxia, or ARDS) causes acute RV dilation. This shifts the electrical axis rightward and anteriorly, stretches the right bundle, and produces the classic pattern. The right-to-left septal shift also alters precordial forces.
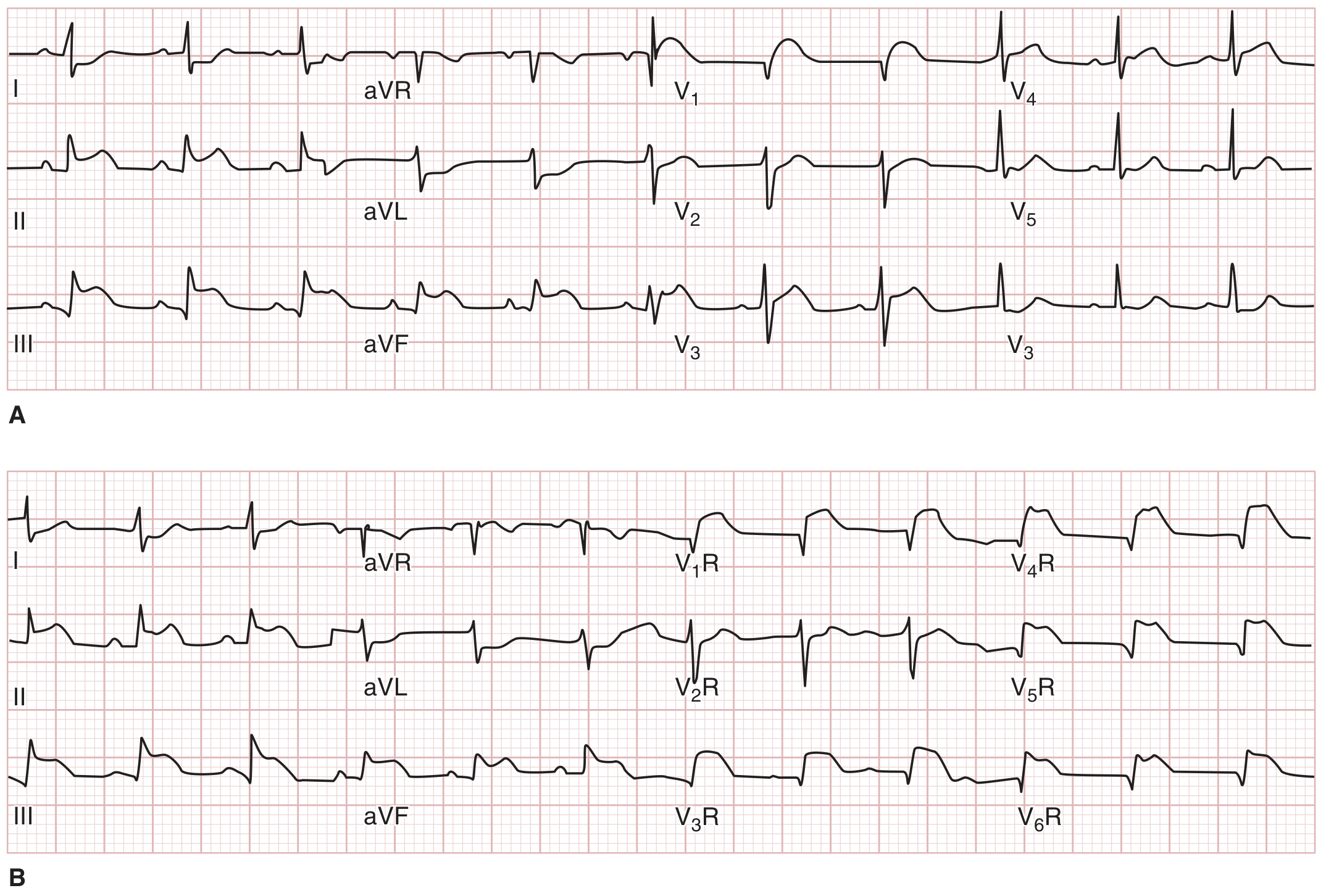
ECG example (Inferior STEMI with RV infarction on standard leads [top] and right-sided leads [bottom]):
Clinical meaning: S1Q3T3 has low sensitivity (~20%) but high specificity for PE. Always interpret in clinical context. The most common ECG finding in PE is simply sinus tachycardia. Confirm with CT pulmonary angiography.
(Harrison's Principles of Internal Medicine 22E)
Quick Reference Summary
| # | Finding | Key ECG Feature | Main Cause |
|---|---|---|---|
| 1 | ST elevation | ≥1 mm ST elevation in ≥2 leads | Acute STEMI |
| 2 | ST depression | Horizontal/downsloping ST depression | NSTEMI / ischemia |
| 3 | Atrial fibrillation | No P waves, irregularly irregular | AF, hyperthyroidism, etc. |
| 4 | RBBB | rSR' in V1, wide S in I/V6, QRS ≥120 ms | RVH, PE, normal variant |
| 5 | LBBB | Broad notched R in V5-V6, QS in V1, QRS ≥120 ms | CAD, cardiomyopathy, HTN |
| 6 | LVH | SV1 + RV5 > 35 mm, lateral strain | HTN, AS, HCM |
| 7 | Pathological Q waves | Q ≥ 40 ms wide and ≥25% R depth | Prior MI (scar) |
| 8 | Long QT | QTc > 450/460 ms | Drugs, electrolytes, congenital |
| 9 | 1st degree AV block | PR > 200 ms | Vagal tone, drugs, myocarditis |
| 10 | RV strain | S1Q3T3, sinus tachycardia, T-inv V1-V4 | Pulmonary embolism, cor pulmonale |
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart, 15th Edition; Medical Physiology (Boron & Boulpaep)
Please give pictures for all
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the images. Here is the complete illustrated guide:
10 Common ECG Findings - With Pictures
1. ST-Segment Elevation (STEMI)
Key features: ST elevated ≥1 mm above baseline in ≥2 contiguous leads. Represents acute transmural myocardial injury - infarcting cells fail to fully repolarize, creating a "current of injury" that lifts the ST segment. Location of elevation tells you which artery is occluded (inferior = RCA; anterior = LAD; lateral = LCx).
Anterior MI from proximal LAD occlusion: ST elevation in V1-V3, with reciprocal ST depression in II, III, aVF. (Tintinalli's Emergency Medicine)
2. ST-Segment Depression
Key features: ST segment displaced ≥0.5-1 mm below baseline. Horizontal or downsloping patterns are most significant. Indicates subendocardial ischemia (the innermost layer of myocardium is most vulnerable to ischaemia because perfusion pressure is lowest there) or NSTEMI. Also appears as reciprocal change opposite a STEMI zone.
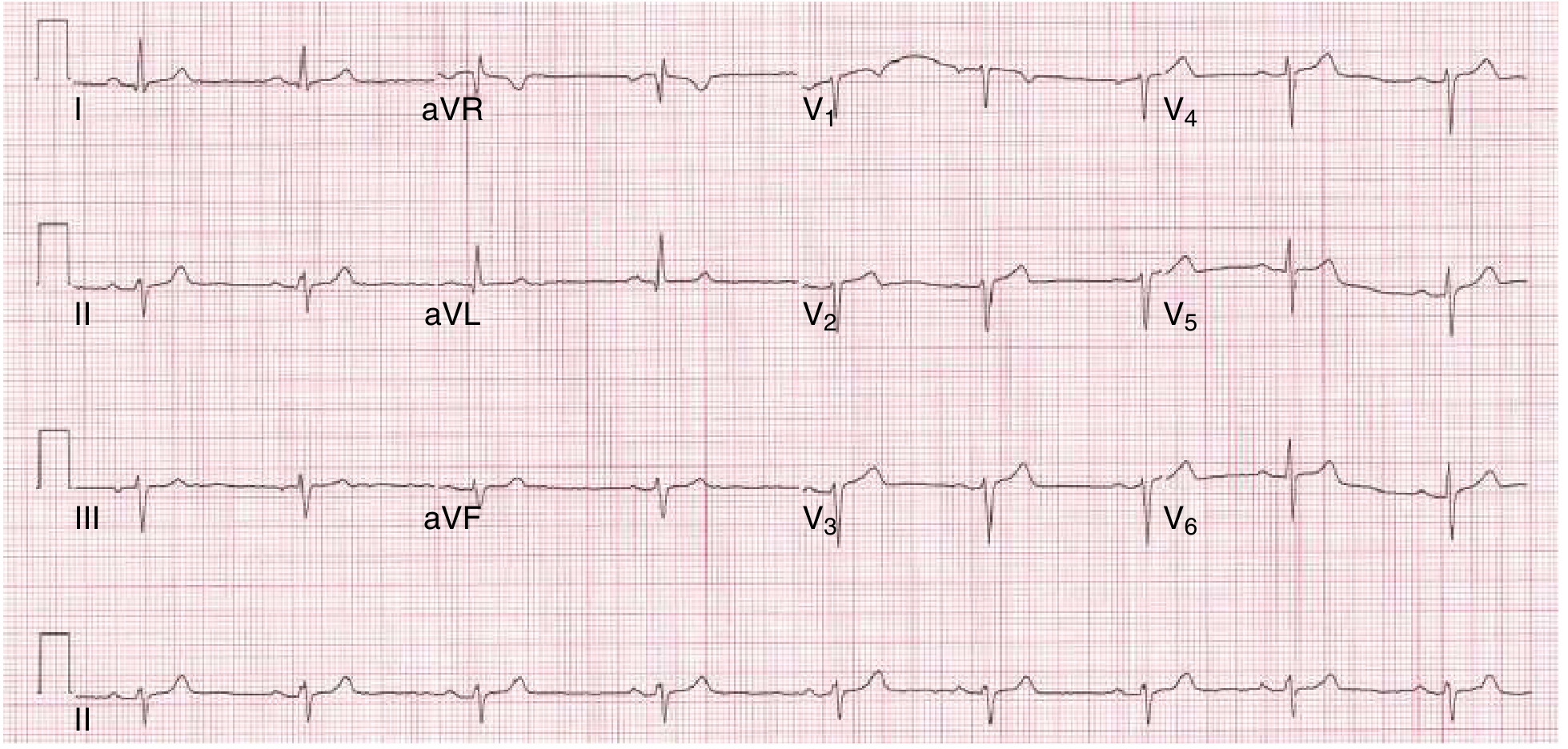
Inferior STEMI with reciprocal ST depression in anterior leads V1-V4, suggesting concurrent posterior wall involvement. (Tintinalli's Emergency Medicine)
3. Atrial Fibrillation
Key features: No identifiable P waves (replaced by chaotic, low-amplitude fibrillatory baseline), irregularly irregular QRS rhythm, narrow QRS (unless aberrant conduction). Rate typically 100-180 bpm if uncontrolled. Multiple re-entrant wavelets circulate chaotically through the atria at 350-600/min; the AV node conducts impulses randomly, producing the classic irregular rhythm.
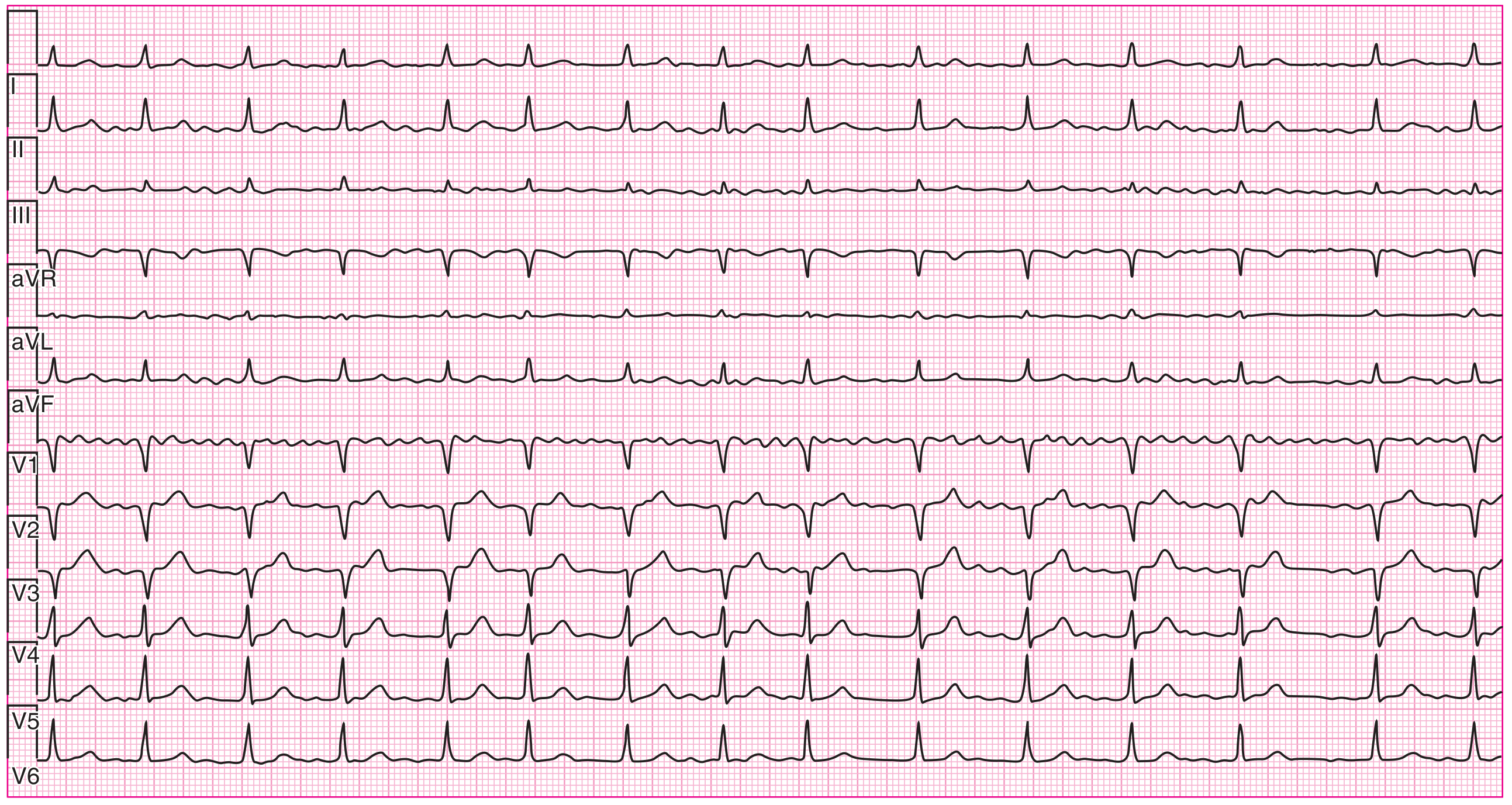
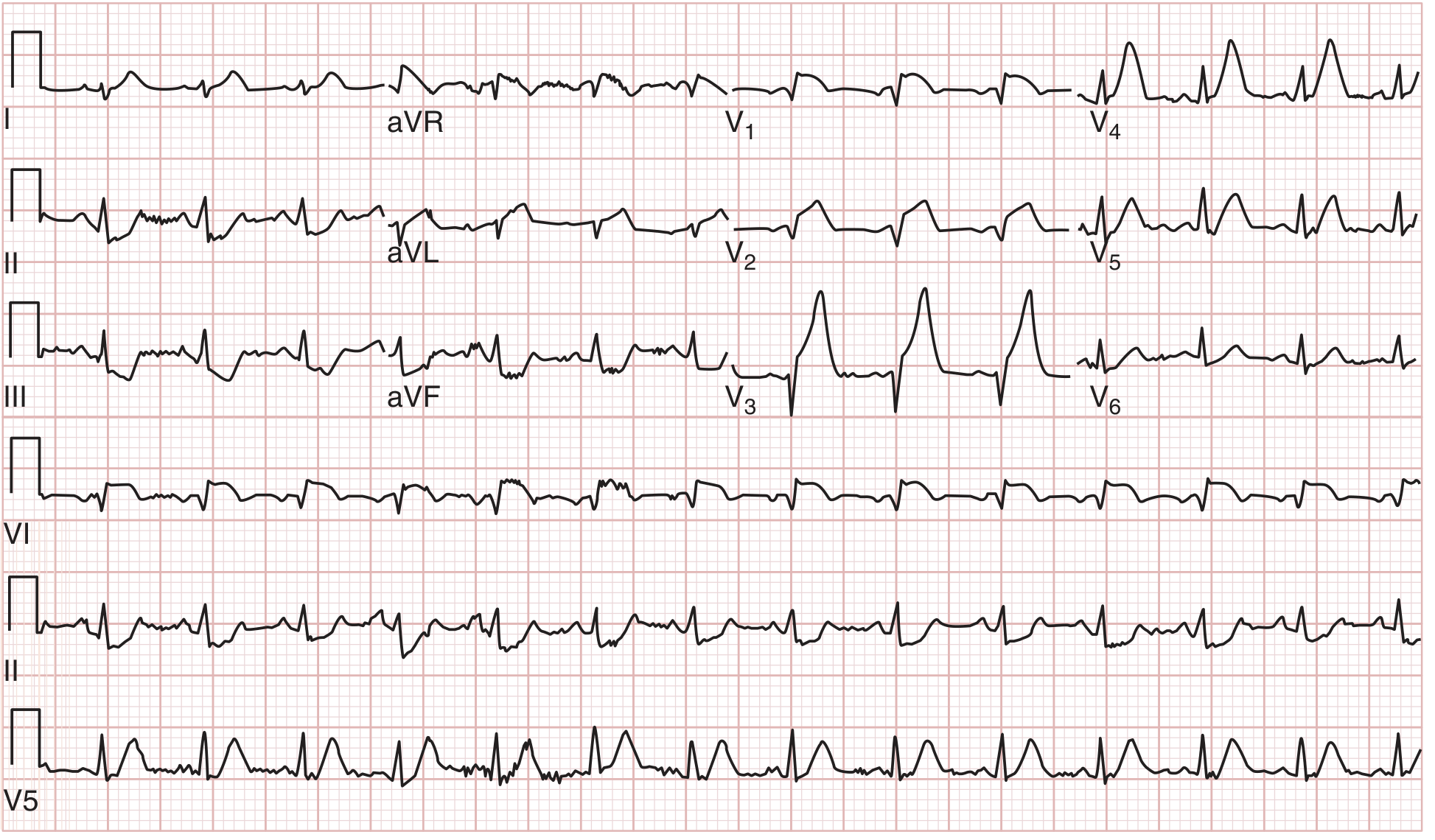
12-lead ECG of atrial fibrillation: absent P waves, irregularly irregular ventricular response best appreciated in V1 and the rhythm strip. (Harrison's Principles of Internal Medicine 22E)

Single-lead (II) ECG of AF: ventricular QRS and T waves visible; no P waves; variable R-R intervals. (Guyton & Hall Textbook of Medical Physiology)
4. Right Bundle Branch Block (RBBB)
Key features: QRS ≥120 ms; classic rSR' ("M-shape") in V1; wide slurred S wave in leads I and V6; discordant ST-T changes in V1-V2. The right bundle is blocked so the RV depolarizes late via slow cell-to-cell spread from the LV, producing a delayed rightward terminal force (the R' in V1 and terminal S in lateral leads).
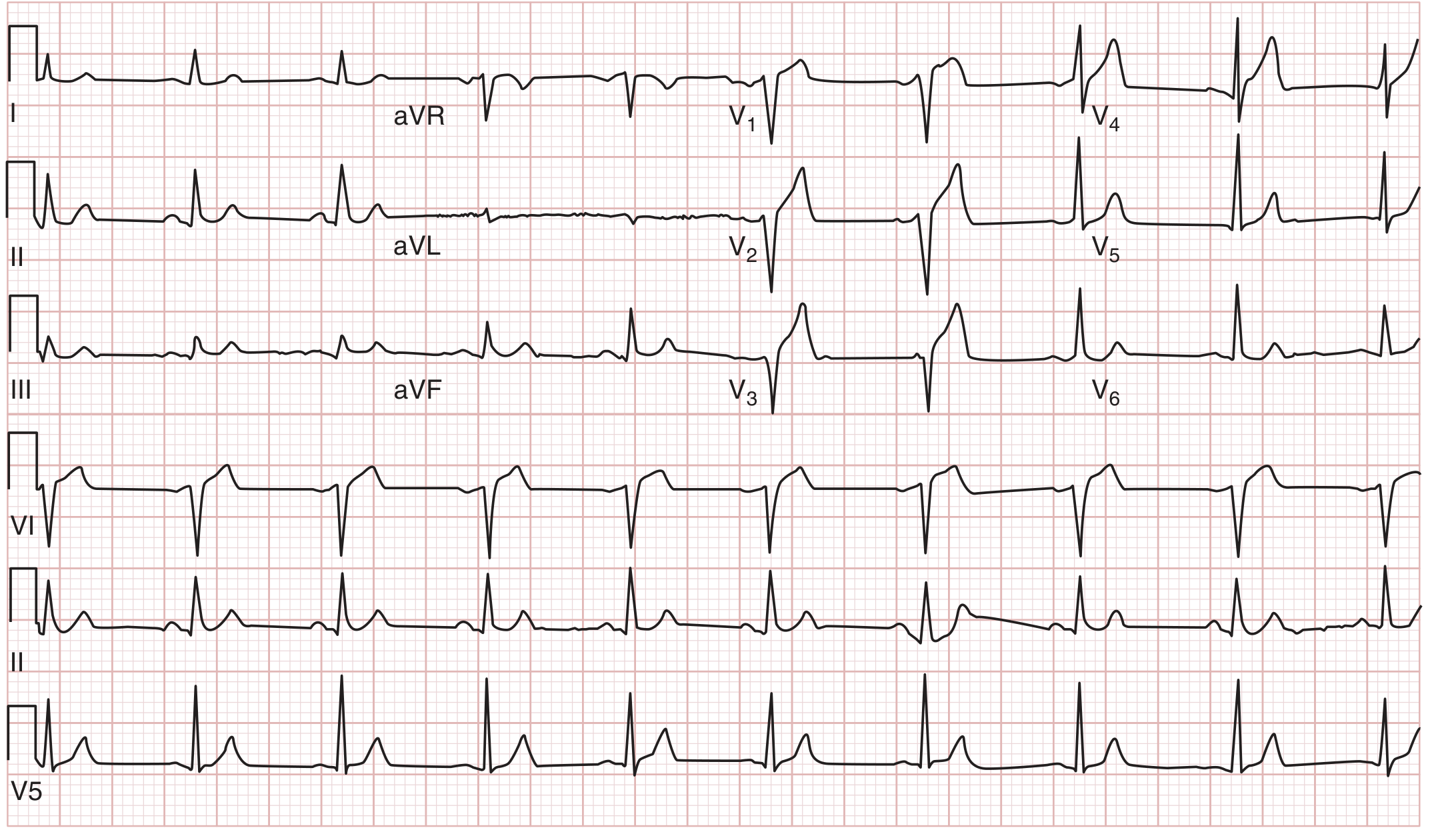
RBBB: Note the rSR' pattern in V1 (M-shape), wide S waves in I and V6, and discordant T waves in V1-V2. (Goldman-Cecil Medicine)
5. Left Bundle Branch Block (LBBB)
Key features: QRS ≥120 ms; broad notched (W-shaped) R wave in V5, V6, I, aVL; rS or QS in V1; absence of septal q waves in lateral leads; discordant ST-T changes throughout. LBBB reverses normal septal activation and delays LV depolarization entirely via slow myocardial conduction from the RV. Almost always pathological - new LBBB with chest pain is a STEMI equivalent.
LBBB: Broad notched R waves in I, V5-V6; QS in V1; no septal q waves; discordant ST-T changes across the precordium. (Goldman-Cecil Medicine)
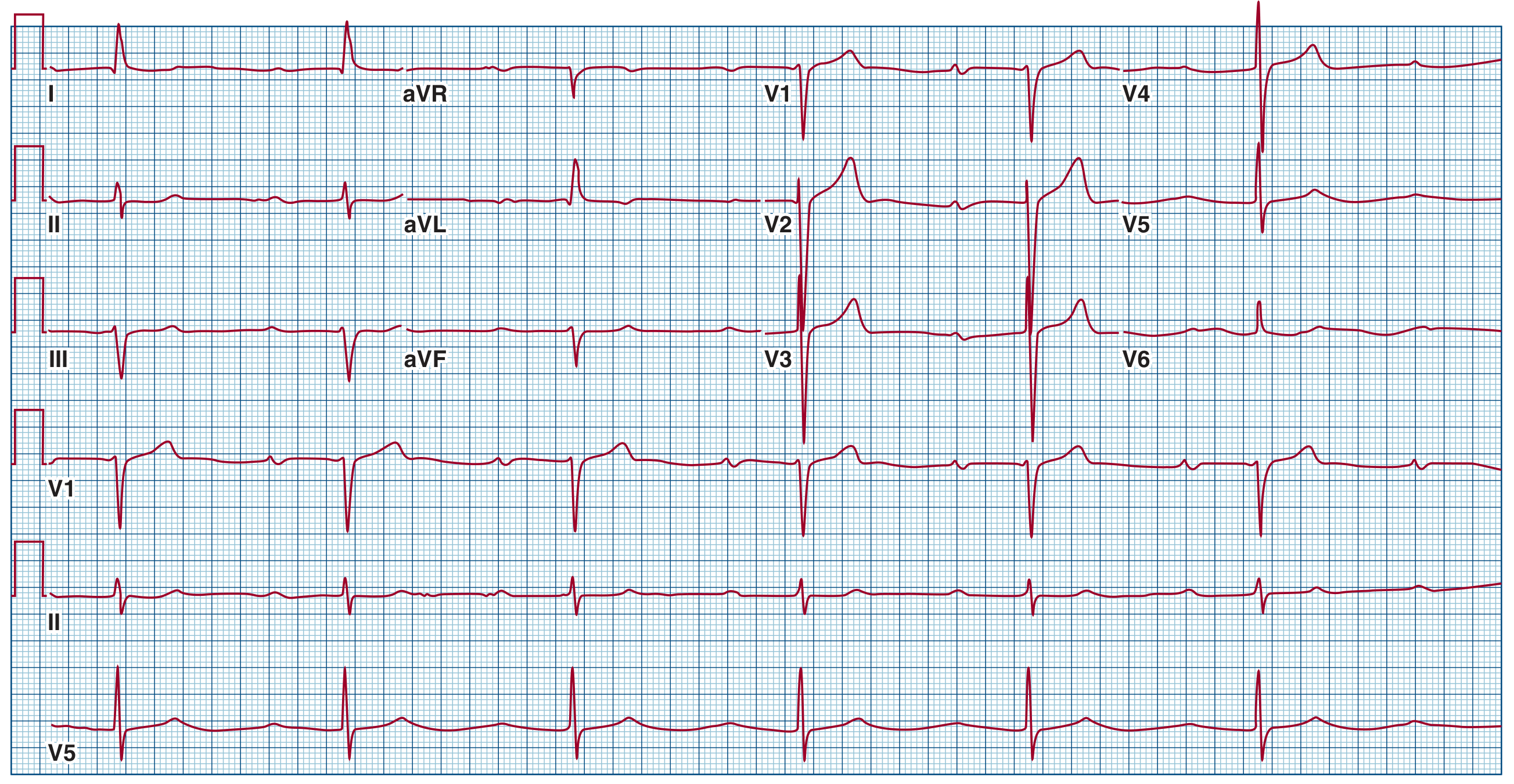
6. Left Ventricular Hypertrophy (LVH)
Key features: SV1 + RV5 (or RV6) > 35 mm (Sokolow-Lyon); tall R in aVL; ST depression + T-wave inversion in lateral leads ("strain" pattern). The hypertrophied LV generates larger electrical forces directed leftward and posteriorly. The "strain" pattern reflects secondary repolarization abnormality due to altered action potential duration in thick myocardium, not ischaemia per se.
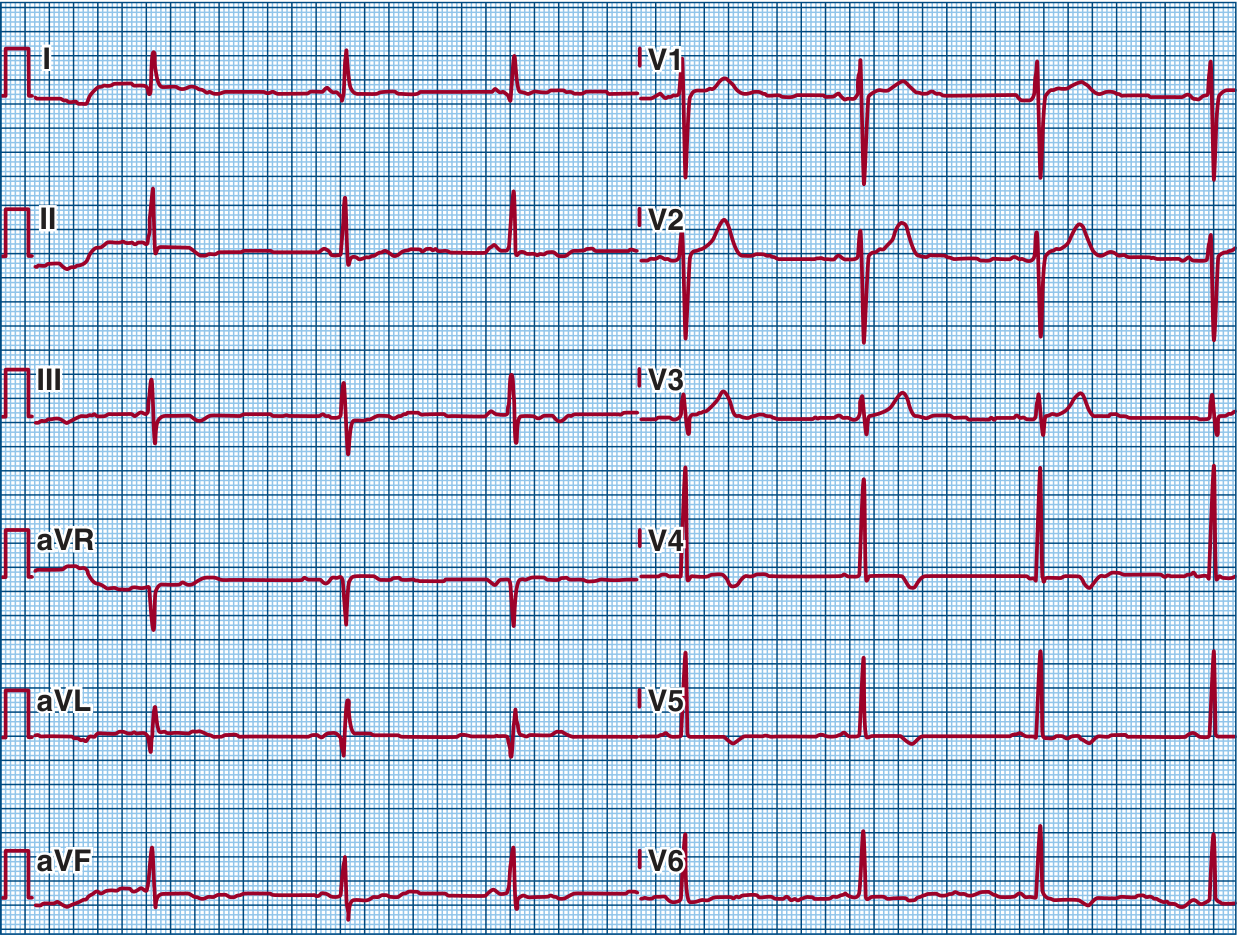
ECG from a patient with hypertrophic cardiomyopathy: prominent LVH voltages, deep negative T waves in anterior and inferior leads, and lateral pathological Q waves. (Fuster and Hurst's The Heart, 15th Edition)
7. Pathological Q Waves (Prior MI / Scar)
Key features: Q wave ≥40 ms wide AND ≥25% of the R-wave amplitude in the same lead. Present in the territory of the old infarct. Dead myocardium generates no electrical signal - the overlying electrode "sees through" electrically silent scar to detect depolarization moving away from it (window effect), producing an initial negative deflection.
(The STEMI tracings above also demonstrate early Q wave formation in the infarct territory. The image below shows deep anterior Q waves from LAD infarction.)

Anterior MI from distal LAD occlusion: ST elevation in I, V1-V3 with pathological Q waves forming - early sign of transmural necrosis. (Tintinalli's Emergency Medicine)
8. Prolonged QT Interval
Key features: Corrected QT (QTc using Bazett's formula: QT/√RR) >450 ms men, >460 ms women. The QT interval represents total ventricular repolarization time. Prolongation creates a vulnerable window where early afterdepolarizations can trigger Torsades de Pointes (TdP) - the characteristic twisting polymorphic VT that can degenerate into VF. QTc >500 ms = high risk.
Panel showing LQT syndromes and Torsades de Pointes: (B) LQT1 with QTc 580 ms; (C) LQT2 with notched T-waves; (D) LQT3 with delayed T-waves; (G) Acquired LQT from methadone (QTc 750 ms) with characteristic Torsades de Pointes (twisting QRS axis). (Fuster and Hurst's The Heart, 15th Edition)
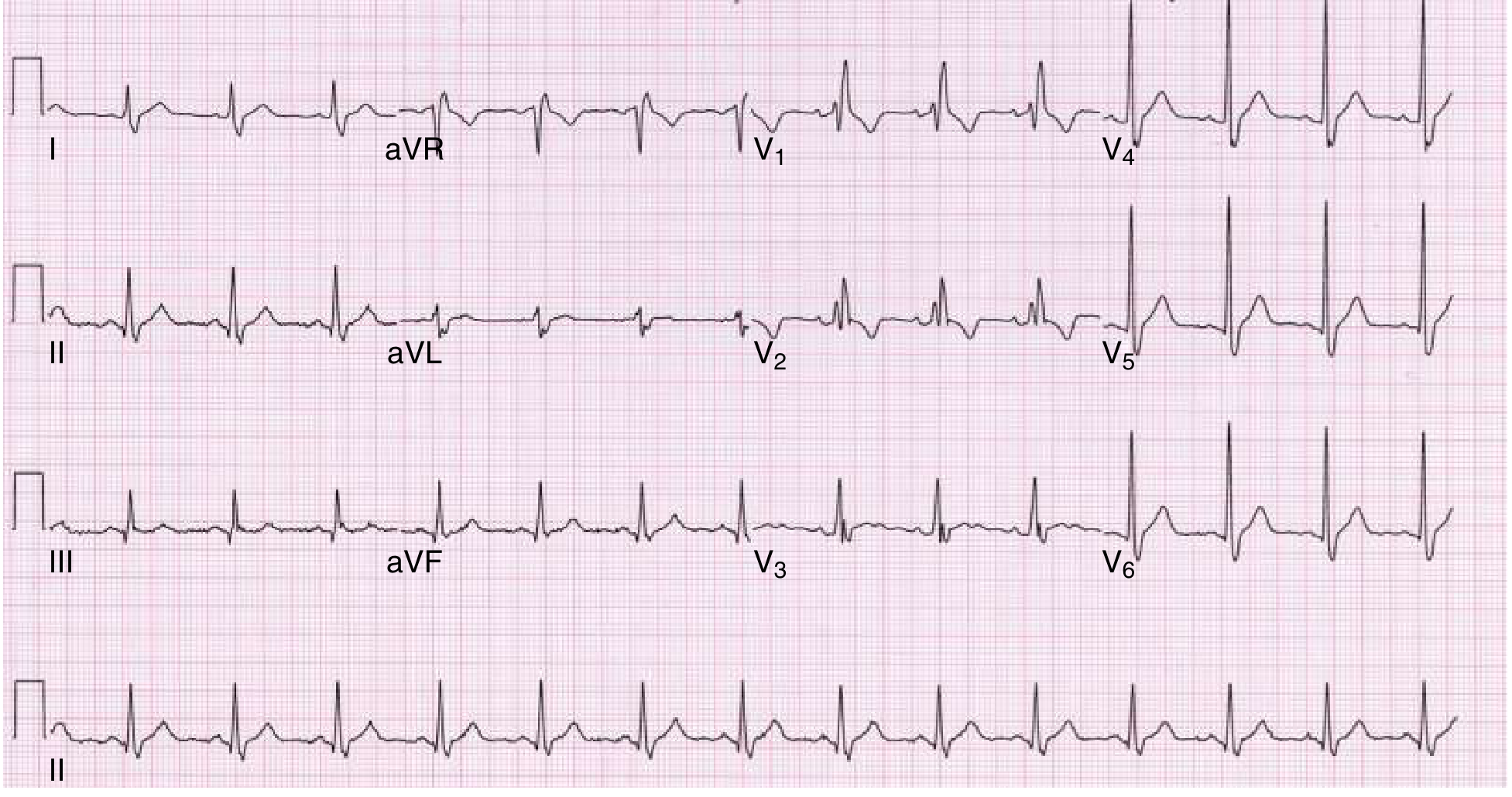
9. First-Degree AV Block
Key features: PR interval >200 ms (>1 large box) in every beat; every P wave followed by QRS; regular rhythm maintained. Slowed conduction through the AV node (most common site) - the impulse is delayed, not blocked. If QRS is narrow, the delay is almost always within the AV node itself.
First-degree AV block: 12-lead ECG demonstrating a markedly prolonged PR interval of 520 ms. Every P wave conducts - no dropped beats. (Fuster and Hurst's The Heart, 15th Edition)
10. Right Ventricular Strain (Acute Cor Pulmonale / PE)
Key features: Sinus tachycardia (most common); S1Q3T3 pattern (S wave in I, Q wave + T-wave inversion in III); right axis deviation; T-wave inversions V1-V4; new RBBB. Acute RV pressure overload from PE causes acute RV dilation, which shifts the electrical axis rightward and anteriorly, stretches the right bundle, and produces the characteristic pattern. S1Q3T3 is specific (~88%) but poorly sensitive (~20%) for PE.

(Above: Acquired LQT with Torsades de Pointes for comparison with finding #8.)
Inferior STEMI with RV involvement: Top panel shows standard leads with inferior ST elevation and right precordial elevation in V1R-V6R on right-sided leads (bottom panel) - demonstrating RV strain/infarction pattern. (Tintinalli's Emergency Medicine)
Summary Reference Table
| # | Finding | Hallmark ECG Feature | Key Mechanism |
|---|---|---|---|
| 1 | ST Elevation (STEMI) | ≥1 mm ST elevation in ≥2 leads | Transmural injury current |
| 2 | ST Depression | Horizontal/downsloping ST ↓ | Subendocardial ischaemia |
| 3 | Atrial Fibrillation | No P waves, irregularly irregular | Chaotic atrial re-entry |
| 4 | RBBB | rSR' in V1, wide S in I/V6 | Late RV depolarization |
| 5 | LBBB | Notched R in V5-V6, QS in V1 | Reversed septal + late LV activation |
| 6 | LVH | SV1+RV5 >35 mm, lateral strain | Large LV mass + repolarization change |
| 7 | Pathological Q waves | Q ≥40 ms, ≥25% R amplitude | Electrical window through scar |
| 8 | Long QT | QTc >450/460 ms | Prolonged repolarization → TdP risk |
| 9 | 1st-degree AV block | PR >200 ms, every P conducts | AV node conduction delay |
| 10 | RV Strain | S1Q3T3, T-inv V1-V4, sinus tach | Acute RV pressure overload |
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart 15th Ed; Guyton & Hall Medical Physiology
This is a shared conversation. Sign in to Orris to start your own chat.