new ballard score by nelson book of pediatrics
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a complete overview of the New Ballard Score (NBS) based on authoritative textbook sources (Textbook of Family Medicine 9e, citing Ballard JL et al., J Pediatr. 1991;119:417-423 - the same reference used in Nelson's Pediatrics):
New Ballard Score (NBS)
The NBS is used to assess gestational age in newborns, including extremely premature infants (as early as 20 weeks). It evaluates two domains - neuromuscular maturity and physical maturity - and sums the scores to estimate gestational age.
Key rule: If gestational age by dates vs. by exam differs by >1 week, use the earlier gestational age.
Part 1: Neuromuscular Maturity
Scores range from -1 to 5 for each criterion. Assign scores with the infant relaxed and quiet.
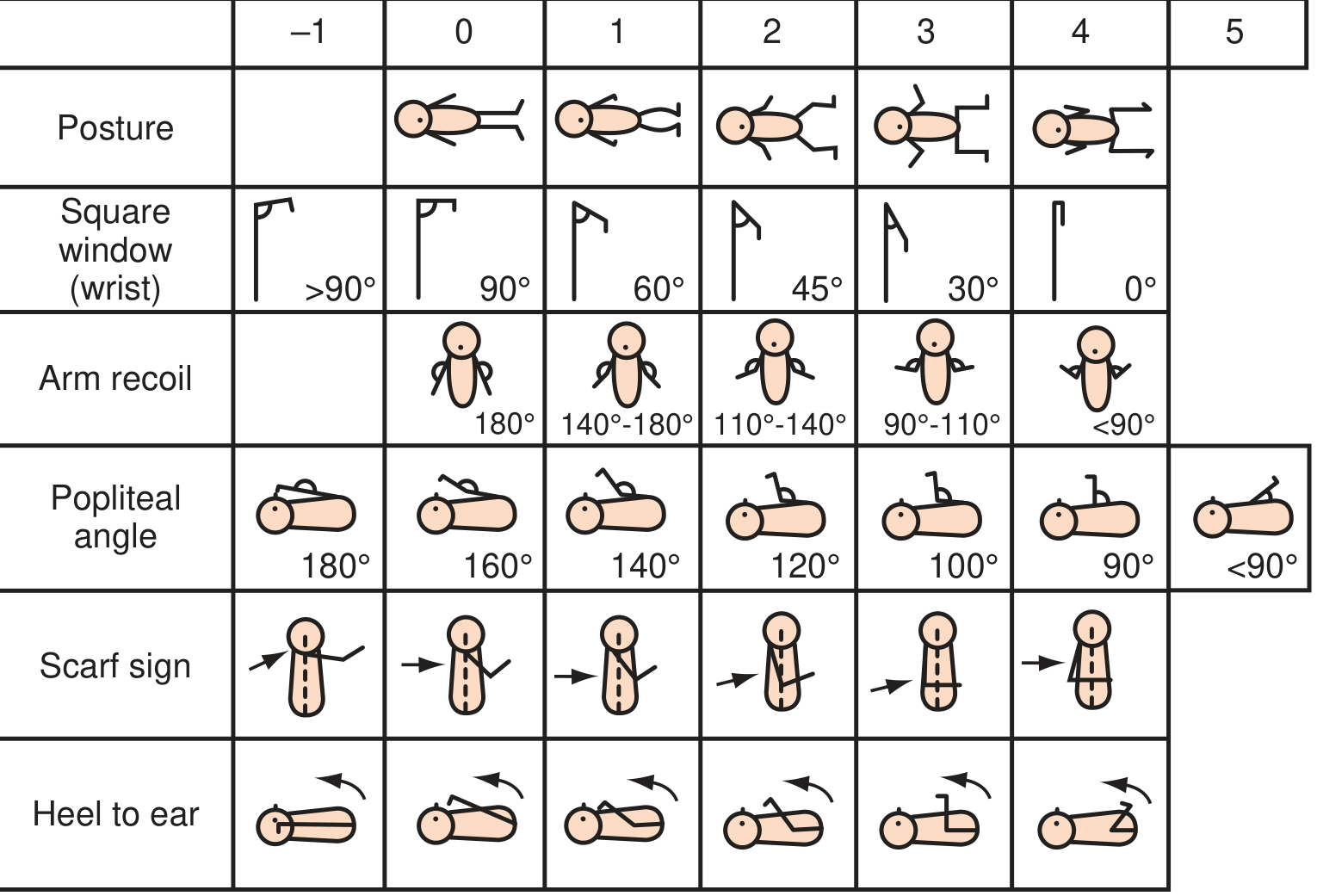
| Criterion | How to Examine | Score Progression |
|---|---|---|
| Posture | Observe infant when relaxed and quiet | Score 0 (fully extended) → 4 (fully flexed) |
| Square window (wrist) | Flex wrist between hypothenar eminence and forearm; measure angle | >90° = 0 → 90° → 60° → 45° → 30° → 0° = 4 |
| Arm recoil | Flex forearms for 5 sec, fully extend arms, release; score position | 180° = 0 → 140-180° → 110-140° → 90-110° → <90° = 4 |
| Popliteal angle | Hip fully flexed, extend knee with gentle pressure; measure popliteal angle | 180° = -1 → 160° → 140° → 120° → 100° → 90° → <90° = 5 |
| Scarf sign | Move arm over opposite shoulder; keep scapula on table | Arm crosses well past midline = -1 → arm reaches midline = 2 → cannot reach midline = 4 |
| Heel to ear | Move foot toward head; keep pelvis on table; do not force | Foot easily reaches ear = -1 → progressively more resistance with maturity |
Part 2: Physical Maturity
Scores range from -1 to 4 or 5 depending on criterion.
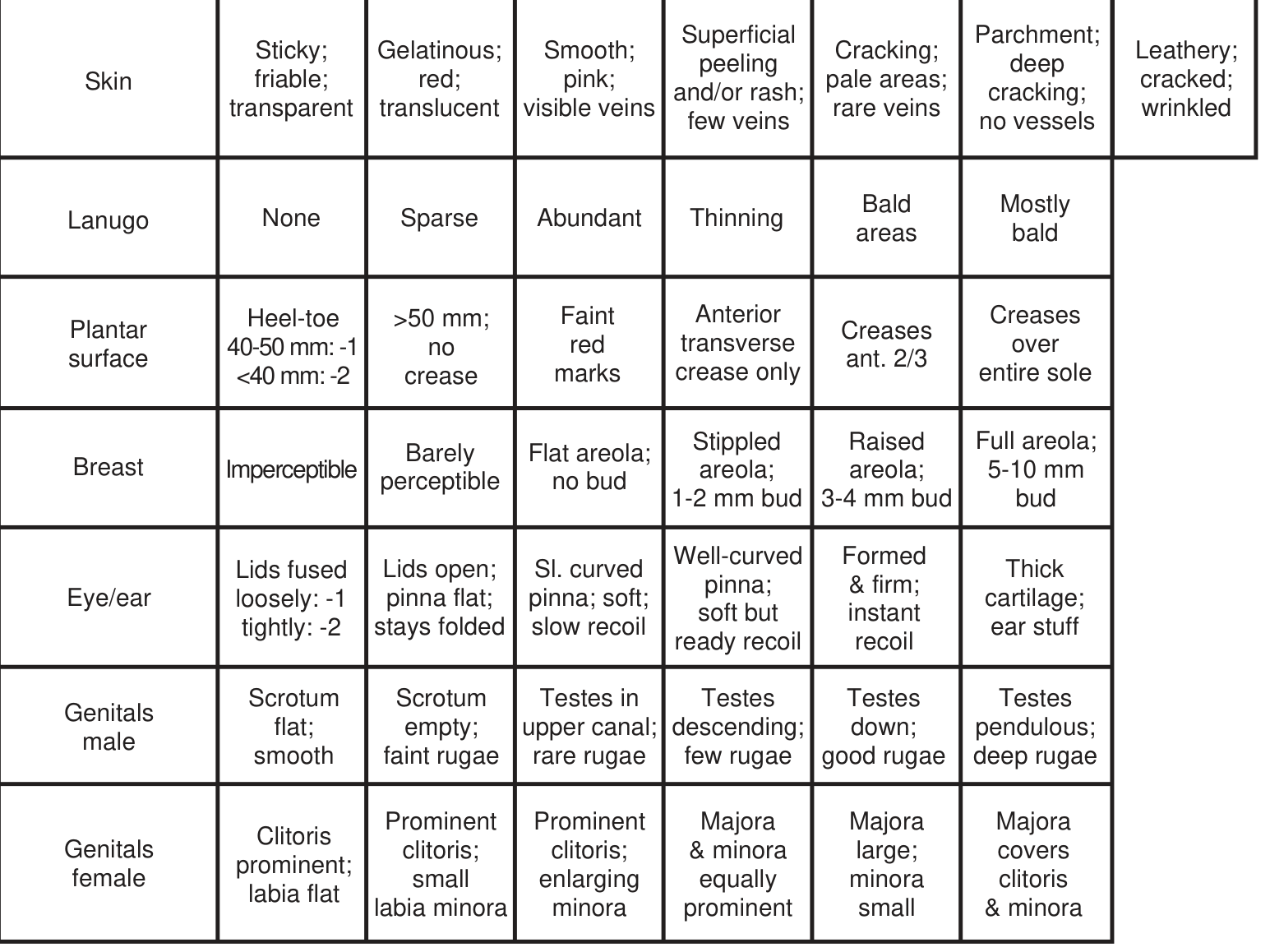
| Criterion | Immature → Mature |
|---|---|
| Skin | Sticky, friable, transparent → Gelatinous, red, translucent → Smooth, pink, visible veins → Superficial peeling/rash, few veins → Cracking, pale areas, rare veins → Parchment, deep cracking, no vessels → Leathery, cracked, wrinkled |
| Lanugo (over back/scapulae) | None → Sparse → Abundant → Thinning → Bald areas → Mostly bald |
| Plantar surface (tip of great toe to back of heel) | Heel-toe <40 mm = -2; 40-50 mm = -1 → >50 mm, no crease → Faint red marks → Anterior transverse crease only → Creases over anterior 2/3 → Creases over entire sole |
| Breast | Imperceptible → Barely perceptible → Flat areola, no bud → Stippled areola, 1-2 mm bud → Raised areola, 3-4 mm bud → Full areola, 5-10 mm bud |
| Eye/Ear | Lids fused tightly = -2; loosely = -1; Lids open, pinna flat, stays folded = 0 → Slightly curved pinna, soft, slow recoil → Well-curved, soft but ready recoil → Formed & firm, instant recoil → Thick cartilage, ear stiff |
| Genitals (Male) | Scrotum flat, smooth → Empty, faint rugae → Testes in upper canal, rare rugae → Testes descending, few rugae → Testes down, good rugae → Testes pendulous, deep rugae |
| Genitals (Female) | Clitoris prominent, labia flat → Prominent clitoris, small labia minora → Prominent clitoris, enlarging minora → Majora & minora equally prominent → Majora large, minora small → Majora covers clitoris & minora |
Part 3: Maturity Rating (Score → Gestational Age)
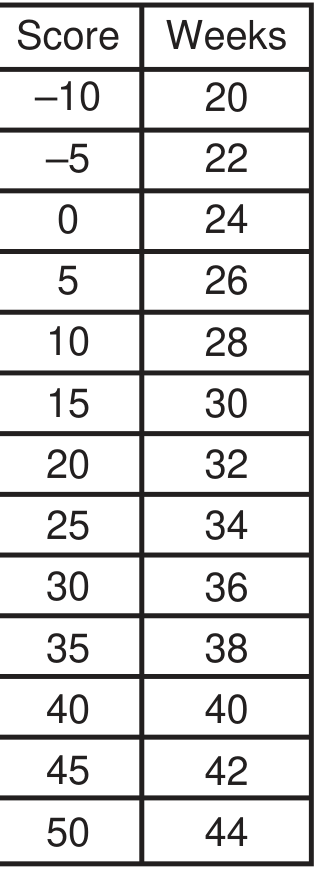
| Total Score | Gestational Age (weeks) |
|---|---|
| -10 | 20 |
| -5 | 22 |
| 0 | 24 |
| 5 | 26 |
| 10 | 28 |
| 15 | 30 |
| 20 | 32 |
| 25 | 34 |
| 30 | 36 |
| 35 | 38 |
| 40 | 40 |
| 45 | 42 |
| 50 | 44 |
Summary of Scoring
- Neuromuscular criteria: 6 items (Posture, Square window, Arm recoil, Popliteal angle, Scarf sign, Heel to ear)
- Physical criteria: 6 items (Skin, Lanugo, Plantar surface, Breast, Eye/Ear, Genitalia)
- Total possible score: -10 to +50
- Covers gestational age range: 20 to 44 weeks
The NBS was expanded from the original Ballard Score to include extremely premature infants (as young as 20 weeks / score -10), which is its key advantage over the older version.
Source: Textbook of Family Medicine 9e, p. 527, citing Ballard JL, Khoury JC, Wedig K et al. New Ballard Score, expanded to include extremely premature infants. J Pediatr. 1991;119:417-423.
APGAR TABLE FROM NELSON OR BATES
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have all the data. Here is the complete APGAR Score Table from both sources:
APGAR Score
Devised by Virginia Apgar in 1952, it provides a standardized method to assess the physical condition of newborns immediately after birth and their response to resuscitation.
The APGAR Table
Each of the 5 signs is scored 0, 1, or 2. Maximum possible score = 10.
| Sign | 0 | 1 | 2 |
|---|---|---|---|
| Heart Rate | Absent | <100 bpm | ≥100 bpm |
| Respiratory Effort | Absent | Irregular / slow | Strong, crying |
| Muscle Tone | Limp | Some flexion of extremities | Active motion / good flexion |
| Reflex Irritability (response to stimulation / nose suction) | No response | Grimace | Cough, sneeze, or cry |
| Color | Blue or pale (all cyanotic) | Acrocyanosis (blue extremities, pink body) | Completely pink |
Mnemonic - APGAR: Appearance (color), Pulse (heart rate), Grimace (reflex irritability), Activity (muscle tone), Respiration
When to Assess
| Timing | Action |
|---|---|
| 1 minute | First score - reflects intrauterine/intrapartum condition |
| 5 minutes | Second score - reflects response to resuscitation |
| Every 5 min up to 20 min | If score remains <7 at 5 min, repeat at 5-min intervals while resuscitation continues |
Score Interpretation
| Score | Interpretation | Action |
|---|---|---|
| 7 - 10 | Normal / reassuring | Routine newborn care |
| 4 - 6 | Moderately depressed | Stimulation + supplemental oxygen; reassess |
| 0 - 3 | Severely depressed | Immediate resuscitation required |
Important Clinical Notes
- Do not delay assessment of airway, breathing, and circulation to calculate the Apgar score - resuscitation always takes priority.
- The score can be affected by: gestational age, maternal medications, neurologic/cardiorespiratory conditions, trauma, infection, and ongoing resuscitation.
- A low score (0-3) does not predict neurologic outcome and cannot determine if a hypoxic event occurred in utero.
- A score of 0-3 at 5 minutes may correlate with increased neonatal death.
- It is considered negligence to omit Apgar scoring of a newborn, especially low birth weight infants.
Sources: Textbook of Family Medicine 9e, p. 526-527 (citing AAP/AHA Neonatal Resuscitation, 2011); The Harriet Lane Handbook 23e, Table 18.2 (citing Apgar V, Anesth Analg 1953;32:260); Park's Textbook of Preventive and Social Medicine, Table 3.
This is a shared conversation. Sign in to Orris to start your own chat.