Contrast induced nephropathy management and prevention
"contrast induced nephropathy" prevention management
Contrast-Induced Nephropathy (CIN) / Post-Contrast Acute Kidney Injury (PC-AKI)
Terminology Clarification
- PC-AKI (Post-Contrast AKI): Any deterioration in renal function within 48 hours of intravascular iodinated contrast, regardless of cause - a correlative diagnosis.
- CIN (Contrast-Induced Nephropathy): A causative subset of PC-AKI where the contrast is directly responsible. It excludes AKI from other concurrent insults (infection, nephrotoxic drugs, etc.).
Definition
- Serum creatinine rise ≥ 0.5 mg/dL (absolute), or ≥ 25% above baseline, within 48 hours of contrast - persisting 2-5 days.
- SCr rise ≥ 0.3 mg/dL (> 26.4 µmol/L)
- SCr rise ≥ 50% (1.5x baseline)
- Urine output ≤ 0.5 mL/kg/h for ≥ 6 hours
Pathophysiology
- Biphasic hemodynamic response: brief initial vasodilation (seconds to minutes) followed by prolonged vasoconstriction.
- Medullary hypoxia is worsened by contrast-induced increase in blood viscosity reducing vasa recta flow.
- Osmotic diuresis increases sodium delivery to the thick ascending loop of Henle, raising oxygen consumption for reabsorption.
- Reactive oxygen species (ROS) mediate proximal tubular injury (evidenced by low-molecular-weight proteinuria).
- Activation of the aldose reductase-fructokinase pathway (stimulated by hyperosmolarity) in the proximal tubule.
- Uricosuria may contribute to tubular injury.
- High osmolality of contrast agents amplifies both mechanisms.
Risk Factors
| Category | Specific Factors |
|---|---|
| Renal | Pre-existing CKD (eGFR < 45 mL/min/1.73 m²), diabetic nephropathy |
| Cardiovascular | Congestive heart failure, low LVEDP, haemodynamic instability |
| Volume status | Dehydration/volume depletion (most significant modifiable factor) |
| Metabolic | Hyperuricemia, multiple myeloma (in dehydrated patients) |
| Demographic | Age > 75 years, hypertension |
| Drug-related | Concurrent NSAIDs, ACE inhibitors/ARBs, diuretics |
| Procedure-related | Intra-arterial > intravenous administration, high contrast dose, repeated/closely-timed studies, hyperosmolar contrast (HOCM) |
Key point: IV contrast CT in patients with eGFR > 30 mL/min/1.73 m² carries very low CIN risk. Intra-arterial contrast (e.g., cardiac catheterisation) poses substantially higher risk due to larger required volumes and direct delivery to renal arteries.
GFR Thresholds for Risk Stratification
| eGFR (mL/min/1.73 m²) | Risk Level |
|---|---|
| > 45 | Low risk for IV contrast |
| 30-45 | Moderate risk; preventive measures indicated |
| < 30 | High risk; consider alternatives to contrast imaging |
| On dialysis | Contrast can be given; coordinate with dialysis schedule |
- ESUR (European Society of Urogenital Radiology): eGFR < 45 as the threshold for elevated risk.
- Canadian Association of Radiologists: Risk starts at eGFR < 45, significantly increases at eGFR < 30.
Prevention Strategies
1. Hydration / Volume Expansion (Most Important)
- Normal saline (0.9% NaCl) at 1-1.5 mL/kg/h for at least 6 hours before AND 6 hours after contrast administration.
- 3 mL/kg/h for 1 hour before, then 1 mL/kg/h for 6 hours after.
- Mix 154 mEq/L sodium bicarbonate in 1L D5W; give 3 mL/kg IV bolus over 1 hour pre-procedure, then 1 mL/kg/h for 6 hours post-procedure.
- Rationale: urinary alkalinization reduces hydroxyl radical generation.
- However, the PRESERVE trial (large multicenter RCT) found no benefit of bicarbonate over normal saline. The 2018 ACR guidelines do not recommend bicarbonate as preferred over saline.
- IV hydration is preferred (certainty of volume delivery); oral hydration is an acceptable alternative in outpatients with eGFR 30-45 when IV is impractical, but the evidence base is weaker.
- In heart failure patients: withhold diuretics the day before and day of contrast; delay contrast until acute decompensation resolves.
2. Choice of Contrast Agent
- Use low-osmolar contrast media (LOCM) (e.g., iopamidol/Isovue, iohexol/Omnipaque) - standard of care; high-osmolar agents (HOCM) are no longer used intravascularly due to higher adverse effect profiles.
- Iso-osmolar agents (e.g., iodixanol) have not shown clear superiority over LOCM in IV studies.
- Minimize contrast volume - limit dose, especially in high-risk patients. Avoid contrast dose > 3-4 mL/kg or above the maximum contrast dose formula (5 mL × body weight (kg) / SCr).
3. Timing Between Contrast Studies
- Allow at least 24 hours between contrast-enhanced studies (time for normal-GFR kidneys to excrete contrast). In CKD, this interval should be longer.
- Avoid repeat contrast-enhanced CT < 24 hours in high-risk patients.
4. Withhold Nephrotoxic and Haemodynamically-Active Drugs
- Withhold NSAIDs, ACE inhibitors/ARBs, diuretics 24-48 hours before contrast in high-risk patients (controversial but commonly recommended).
- Withhold metformin in eGFR < 60 mL/min before contrast, restart 48 hours after if kidney function is stable (to prevent lactic acidosis in the setting of AKI, not directly nephroprotective).
- Discontinue any other concurrent nephrotoxins where clinically feasible.
5. N-Acetylcysteine (NAC)
- Antioxidant thiol; mechanistic rationale: scavenges ROS, vasodilator.
- Oral dose: 600 mg twice daily the day before and day of contrast.
- IV dose (emergency): 150 mg/kg bolus over 30 min pre-procedure, then 50 mg/kg over 4 hours.
- Evidence: Conflicting. Large RCTs (including the ACT trial) and meta-analyses show inconsistent results. The ACR does not classify NAC as proven. However, given low cost and minimal side-effect profile, some centres continue to use it alongside IV hydration.
6. Other Pharmacological Agents (Emerging/Investigational)
| Agent | Mechanism | Evidence Status |
|---|---|---|
| Statins (e.g., rosuvastatin) | Anti-inflammatory, antioxidant, pleiotropic | Promising in small RCTs; meta-analyses show benefit in PCI patients; not yet standard of care |
| Ascorbic acid | Antioxidant | Investigated; limited data |
| Fenoldopam | Dopamine-1 agonist, renal vasodilator | Early trials mixed; not recommended |
| Theophylline | Adenosine antagonist, renal vasodilator | Some benefit in small trials; not standard |
| SGLT2 inhibitors | Tubuloglomerular feedback modulation | Emerging data in PCI patients (meta-analysis PMID 41366914, 2025); potentially protective |
| Nicorandil | K-ATP channel opener, vasodilator | Meta-analysis (PMID 40340567, 2025) suggests potential benefit in coronary angiography patients |
7. RenalGuard System
- Matched urine output-guided hydration device that maintains high urine output (≥ 300 mL/h) during contrast procedures.
- A 2025 systematic review (PMID 40099270) found it beneficial in CKD patients undergoing cardiac interventions.
- Not widely available; reserved for high-risk catheterisation lab patients.
8. Consider Alternative Imaging
- Non-contrast CT for many indications
- Ultrasound for vascular and renal assessment
- MRI (note: gadolinium-based agents are contraindicated in eGFR < 30 due to nephrogenic systemic fibrosis risk with certain linear chelates)
Clinical Course & Management of Established CIN
| Timeframe | Event |
|---|---|
| 24 hours post-contrast | SCr begins to rise |
| 96 hours (4 days) | SCr peaks |
| 7-10 days | Returns to baseline in most patients |
- Continue aggressive IV hydration (unless volume overloaded).
- Stop all nephrotoxins.
- Monitor electrolytes, urine output, daily creatinine.
- Manage complications of AKI - hyperkalaemia, metabolic acidosis, fluid overload, uraemia.
- Renal replacement therapy (dialysis/haemofiltration) if: refractory hyperkalaemia, acidosis, fluid overload, or severe uraemia. Prophylactic dialysis to remove contrast is not recommended (contrast clears faster than dialysis can remove it, and dialysis itself carries risks).
- Follow-up renal function at 1 week and 1 month to confirm recovery.
Patients who develop CIN have longer hospitalisation, higher short-term mortality, and higher rates of cardiac/neurologic events compared to matched controls - though some of this association may reflect confounding by underlying comorbidity severity rather than CIN causality.
Summary Algorithm
Patient requiring contrast study
|
├── Assess eGFR
|
├── eGFR > 45 → Routine; no specific prevention needed
|
├── eGFR 30-45 → IV hydration (NS 1 mL/kg/h x 6h pre + post)
| Low-osmolar contrast; minimise volume
| Withhold nephrotoxins
| Consider NAC (600 mg PO BID x 2 days)
|
└── eGFR < 30 → Above PLUS consider alternative imaging
Discuss with nephrology
Inpatient monitoring post-procedure
Recent Evidence Update (2024-2026)
- SGLT2 inhibitors pre-PCI (meta-analysis 2025, PMID 41366914): Pre-procedure SGLT2 inhibitor use in AMI patients undergoing PCI was associated with reduced CIN incidence. Mechanism likely involves tubuloglomerular feedback normalisation. Not yet in major guidelines but biologically plausible.
- Nicorandil (meta-analysis 2025, PMID 40340567): Showed potential benefit in coronary angiography; larger trials needed.
- Left Ventricular End-Diastolic Pressure (LVEDP) (systematic review 2026, PMID 38349134): Elevated LVEDP is independently associated with CIN risk in coronary angiography patients and may guide periprocedural hydration intensity.
- The concept that IV contrast routinely causes clinically significant nephropathy in patients with preserved renal function has been substantially challenged by propensity-matched studies - risk may have been significantly overstated historically, particularly for IV (as opposed to intra-arterial) administration.


Abdomen pic with skin lesion
Clinical Image Analysis - Abdominal Skin Lesions
- Numerous small (1-3 mm), discrete, hyperpigmented brown macules/papules scattered diffusely across the abdominal skin
- The lesions appear folliculocentric - each one appears to correspond to a hair follicle opening
- Distribution is relatively uniform, non-confluent
- Skin background appears otherwise intact, without erythema, scaling, or excoriation
- The navel (umbilicus) is visible in the second image, confirming this is the anterior abdomen/periumbilical region
- A single small red/erythematous lesion is also visible in image 2 (mid-lower abdomen)
- No vesicles, bullae, or plaques visible
Differential Diagnosis
1. Keratosis Pilaris (KP) with Post-Inflammatory Hyperpigmentation - Most Likely
2. Comedones (Open/Closed) - Acne vulgaris / Truncal Acne
3. Milia
4. Darier Disease (Keratosis Follicularis) - Consider if Persistent
- The Fitzpatrick textbook describes the lesions as: "discrete, greasy, yellowish-brown keratotic papules... predilection for seborrheic areas including central chest, upper back, scalp, neck, and skin creases (axillae, groins, perineum)" - Fitzpatrick's Dermatology
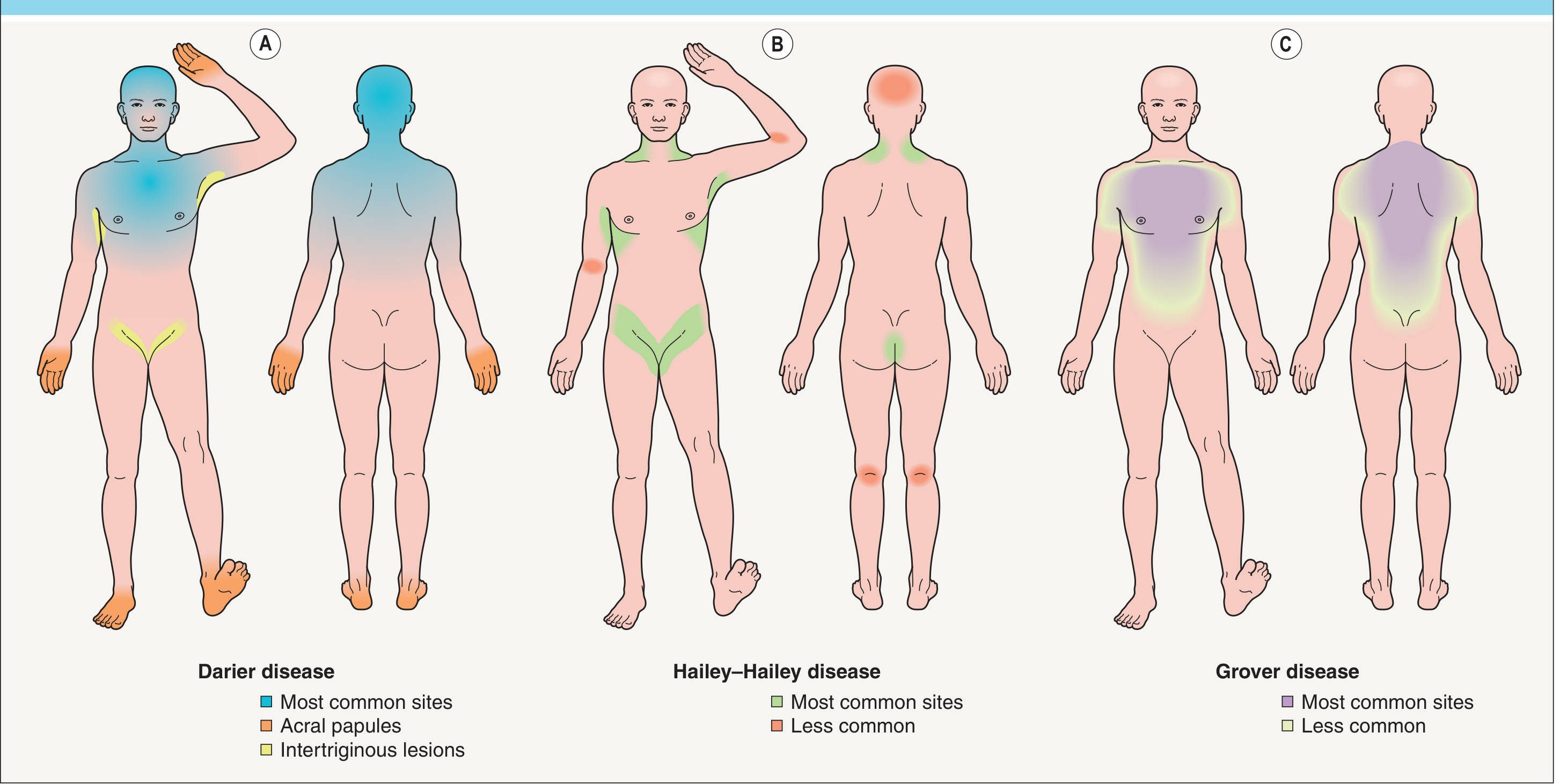
5. Grover Disease (Transient Acantholytic Dermatosis)
6. Sebaceous Hyperplasia / Follicular Cysts
7. Tinea Versicolor (Pityriasis Versicolor)
Recommended Clinical Assessment
| Step | Action |
|---|---|
| History | Duration, pruritus (Grover's is pruritic; KP/Darier's less so), family history (Darier's is autosomal dominant), acne history, prior similar lesions |
| Full skin exam | Check nails (Darier's), scalp, palms/soles, axillae, mucous membranes |
| Wood's lamp | Tinea versicolor fluoresces yellow-green |
| KOH scraping | If scale present - "spaghetti and meatballs" on KOH = Malassezia |
| Dermoscopy | Can distinguish follicular keratotic plugs (KP/Darier) from pigmented macules (PIH) |
| Skin biopsy | If Darier disease or Grover disease is suspected - shows acantholysis with corps ronds and corps grains (Darier) or similar changes (Grover) |
Summary
Important disclaimer: This is a visual analysis for educational and differential-diagnostic purposes only. A formal dermatological examination, dermoscopy, and potentially skin biopsy are required for definitive diagnosis. Please consult a dermatologist.
Also complaining of bl sole burning and numb sensations
Integrating the Full Clinical Picture
- Multiple small folliculocentric brown macules/papules on the abdomen
- Bilateral sole burning and numbness (new symptom)
Top Unifying Diagnoses
1. Diabetes Mellitus - Most Likely Unifying Diagnosis
- Diabetic skin lesions include multiple findings visible on the abdomen: diabetic dermopathy (brown macules), follicular hyperkeratosis, and acanthosis nigricans in skin folds. The scattered brown follicular macules fit diabetic dermopathy well.
- Diabetes is also directly associated with Darier-like follicular keratosis patterns in some patients.
- Diabetic peripheral neuropathy (DPN) is the most common cause of bilateral burning/numb feet worldwide.
- It follows a classic length-dependent, stocking-glove pattern - starting in the soles and ascending.
- Characterised by small-fiber involvement initially: burning, heat sensation, dysesthesias, followed by numbness as large fibers are progressively lost.
- Adams & Victor's Principles of Neurology lists diabetes as the leading identifiable cause of painful sensory neuropathy.
- Fasting blood glucose, HbA1c, OGTT
- Urine microalbumin
2. Nutritional / Vitamin Deficiency Neuropathy
| Deficiency | Skin Findings | Neuropathy |
|---|---|---|
| B3 (Niacin/Pellagra) | Photosensitive dermatitis, hyperpigmented skin lesions | Small-fiber neuropathy - classic "burning feet"; dysesthesias and paresthesias |
| B12 (Cobalamin) | Hyperpigmentation (especially in darker skin tones) | Subacute combined degeneration + painful sensory neuropathy |
| B1 (Thiamine) | Non-specific | Classic burning feet / beri-beri neuropathy |
| B5 (Pantothenic acid) | Non-specific | Small-fiber neuropathy with "burning feet" - direct quote from Goldman-Cecil Medicine |
- Serum B12, folate, B1, B3 (niacin) levels
- Full blood count (macrocytic anaemia in B12 deficiency)
- Dietary history - malnutrition, alcohol use, malabsorption
3. Fabry Disease - Important Rare Diagnosis Not to Miss
- Angiokeratomas - small dark red-brown papules on the trunk/abdomen (which can be mistaken for simple pigmented macules, especially in early disease or darker skin)
- Burning neuropathic pain in extremities - typically described as burning/tingling in the hands and feet; this is often the first symptom in young patients
- Corneal verticillata, renal disease, cardiomyopathy develop later
- Alpha-galactosidase A enzyme activity (leukocytes) - males
- GLA gene mutation testing - females and equivocal cases
- Urine sediment for lipid-laden cells
4. Darier Disease + Incidental Small Fiber Neuropathy
5. Pellagra (Niacin/B3 Deficiency)
- Dermatitis - photosensitive, hyperpigmented skin (can appear as brownish macular pigmentation)
- Diarrhea
- Dementia/neuropsychiatric symptoms
- Death (if untreated)
6. HIV/AIDS-Related
Recommended Workup - Prioritised
Tier 1 (Do Immediately)
| Test | Rationale |
|---|---|
| HbA1c + fasting glucose | Diabetes - most common unifying cause |
| Serum B12, folate | B12 neuropathy + hyperpigmentation |
| Full blood count | Macrocytic anaemia (B12/folate), anaemia |
| Serum B1, B3, B5 levels | Nutritional neuropathy |
| Renal function, eGFR | Uraemic neuropathy |
| LFTs + GGT | Alcohol-related, hepatic |
Tier 2 (Based on Tier 1 Results / Clinical Suspicion)
| Test | Rationale |
|---|---|
| Alpha-galactosidase A | Fabry disease |
| HIV serology | HIV neuropathy |
| Nerve conduction studies (NCS) + EMG | Characterise neuropathy type (axonal vs demyelinating; length-dependent) |
| Skin biopsy (punch biopsy) for intraepidermal nerve fiber density (IENFD) | Diagnose small fiber neuropathy specifically |
| ANA, ANCA, anti-Ro/La, anti-Sm | Connective tissue disease (Sjögren's, SLE) |
| Serum protein electrophoresis (SPEP) | Paraproteinaemia/amyloidosis |
| Thyroid function (TSH, free T4) | Hypothyroid neuropathy |
Tier 3 (Specialist Referral)
- Dermatology - Skin biopsy of the abdominal lesions
- Neurology - Formal neuropathy workup
- Ophthalmology - Corneal slit-lamp exam if Fabry disease suspected (corneal verticillata)
Summary: Clinical Synthesis
Bilateral sole burning/numbness
+
Truncal folliculocentric brown macules
↓
THINK SYSTEMICALLY:
1. Diabetes mellitus (most common)
2. Nutritional deficiency (B1/B3/B5/B12)
3. Fabry disease (rare but treatable - don't miss)
4. HIV
5. Connective tissue disease
Start with: HbA1c, B12, FBC, RFT, LFTs, TSH
Refer: Dermatology + Neurology
Important note: Bilateral burning and numbness of the soles represents a small-fiber neuropathy pattern until proven otherwise. The most important immediate step is to exclude diabetes (HbA1c) and nutritional deficiencies (B12, B1, B3) - both of which are common, treatable, and directly explain the skin and neurological findings together.
Her reports
python3 -c " import pdfplumber with pdfplumber.open('/home/daytona/workspace/attachments/a7cf4574-3f46-43d5-81d9-f5df06bcf83c/60502200662.pdf') as pdf: print(f'Pages: {len(pdf.pages)}') for i, page in enumerate(pdf.pages): print(f'--- PAGE {i+1} ---') text = page.extract_text() if text: print(text) tables = page.extract_tables() for j, table in enumerate(tables): print(f'[Table {j+1}]') for row in table: print(row) "
Lab Report Analysis - Ramilaben Valera, F/57 (Dated: 24-May-2026)
Complete Results Summary
| Test | Result | Reference | Status |
|---|---|---|---|
| Haemoglobin | 12.0 g/dL | 12.0-15.0 | Low-normal (borderline) |
| PCV | 35.96% | 36.0-46.0 | LOW ↓ |
| MCV | 93.4 fL | 83-101 | Normal |
| WBC | 8130 /µL | 4000-10000 | Normal |
| Platelets | 312,000 /µL | 150k-410k | Normal |
| ESR | 20 mm/hr | 3-30 | Normal |
| Fasting Glucose | 97.37 mg/dL | 70-100 | Normal |
| HbA1c | 5.78% | <5.7 Normal / 5.7-6.4 Prediabetes | PREDIABETES ⚠️ |
| Urea | 27.83 mg/dL | 18-55 | Normal |
| Creatinine | 0.57 mg/dL | 0.5-1.1 | Normal |
| Uric acid | 4.87 mg/dL | 2.3-6.1 | Normal |
| Sodium/K/Cl | All normal | Normal | |
| LFT (ALT/AST/ALP/GGT) | All normal | Normal | |
| Total Cholesterol | 220.5 mg/dL | <200 | HIGH ↑ |
| HDL Cholesterol | 36.7 mg/dL | 40-60 | LOW ↓ |
| LDL Cholesterol | 144.49 mg/dL | <100 | HIGH ↑ |
| Triglycerides | 196.53 mg/dL | 40-200 | High-normal (borderline) |
| VLDL | 39.31 mg/dL | 10-40 | Borderline high |
| Chol/HDL ratio | 6.01 | <4.1 | HIGH ↑ (atherogenic) |
| Vitamin B12 | 351.2 pg/mL | 187-883 | Normal |
| Vitamin D (25-OH) | 25.3 ng/mL | 30-100 Normal; 20-30 Insufficiency | INSUFFICIENT ↓ |
| Calcium | 9.07 mg/dL | 8.4-10.2 | Normal |
| Urine | All negative | Normal | |
| ANA (IIF) | PENDING | Result awaited |
Key Abnormalities - Clinical Interpretation
1. HbA1c 5.78% - PREDIABETES
- HbA1c 5.78% places her firmly in the prediabetes range (5.7-6.4%).
- Estimated average glucose over the past 3 months: 119 mg/dL.
- The fasting glucose of 97 mg/dL is normal (not yet impaired fasting glucose), but HbA1c tells a different story - indicating higher average glycaemia throughout the day.
Prediabetic small-fiber neuropathy is now a well-recognised entity. Bilateral burning and numbness of the soles can begin in the prediabetic stage, before frank diabetes develops. The small sensory C-fibres and Aδ-fibres in the feet are among the first to be damaged by chronic mild hyperglycaemia. This explains both the burning sensation (positive sensory symptoms = small fiber C-fiber damage) and the numbness (loss of sensation = progressive fiber loss).
- Lifestyle intervention NOW - dietary modification, weight management, regular exercise can reverse prediabetes and halt neuropathy progression
- Repeat HbA1c in 3-6 months
- Oral glucose tolerance test (OGTT) to better characterise glucose metabolism
- Refer to diabetologist/endocrinologist
2. Dyslipidaemia - Atherogenic Pattern
| Finding | Value | Significance |
|---|---|---|
| Total cholesterol 220.5 | HIGH | +20.5 above upper limit |
| LDL 144.49 mg/dL | HIGH | 44 points above the <100 target |
| HDL 36.7 mg/dL | LOW | Below the protective threshold |
| Chol/HDL ratio 6.01 | HIGH | >4.1 = elevated cardiovascular risk |
| TG 196.53 | High-normal | Near the 200 cutoff |
- Statin therapy discussion (given LDL >140 + prediabetes + atherogenic ratio)
- Dietary counselling: reduce saturated fats, refined carbohydrates, increase omega-3 rich foods
- Lifestyle modification: exercise significantly raises HDL
- Repeat fasting lipid profile in 6-8 weeks after lifestyle changes
- Calculate 10-year ASCVD risk (Framingham / PCE score)
3. Vitamin D 25.3 ng/mL - INSUFFICIENCY
- Level: 25.3 ng/mL (Normal ≥30; Insufficiency = 20-<30; Deficiency <20)
- She is in the insufficiency zone.
- Vitamin D insufficiency is increasingly associated with musculoskeletal pain, fatigue, and neuropathic-type symptoms including paraesthesias and burning sensations in the feet - though this is likely a contributing/aggravating factor rather than the primary cause in her case.
- Low Vitamin D also potentiates insulin resistance and impairs beta-cell function, making her prediabetes harder to reverse.
- Low Vitamin D can worsen dyslipidaemia by upregulating HMG-CoA reductase.
- Cholecalciferol (Vitamin D3) supplementation: 60,000 IU weekly for 8-12 weeks (loading dose), then 1000-2000 IU/day maintenance
- Recheck 25-OH Vitamin D after 3 months
- Encourage sun exposure (20-30 min/day)
- Also check PTH to assess secondary hyperparathyroidism from Vit D insufficiency
4. PCV 35.96% - Borderline Low (Mild Anaemia)
- Haemoglobin is at the lower limit of normal (12.0 g/dL = exactly the lower reference limit for females).
- PCV 35.96% is just below normal (36-46%).
- MCV is normal (93.4 fL) - normocytic - so this is NOT B12 deficiency anaemia (which is macrocytic).
- B12 level is normal at 351 pg/mL - B12 neuropathy is excluded.
- Possible cause: Iron deficiency without anaemia, or mild anaemia of chronic disease. Ferritin, serum iron, TIBC not done.
- Check serum ferritin and iron studies to exclude iron deficiency
- Menstrual history (postmenopausal at 57?)
- Repeat CBC in 3 months
5. ANA (IIF) - PENDING
- Small fiber neuropathy with burning feet
- Dry skin with follicular changes
- Normal B12, normal glucose
Integrated Clinical Picture
57-year-old woman
├── SKIN: Multiple small folliculocentric brown macules, abdomen
├── NEURO: Bilateral sole burning + numbness
└── LABS:
├── HbA1c 5.78% → PREDIABETES ← MOST LIKELY CAUSE OF NEUROPATHY
├── Dyslipidaemia (LDL↑, HDL↓, Chol/HDL ratio↑) → METABOLIC SYNDROME
├── Vitamin D insufficiency → CONTRIBUTING FACTOR
├── Borderline anaemia (normocytic) → Fe studies needed
├── B12 normal → B12 neuropathy EXCLUDED
└── ANA → PENDING (rule out Sjögren's/SLE)
- Prediabetes (HbA1c 5.78%)
- Atherogenic dyslipidaemia (high LDL, low HDL, high TG)
- Vitamin D insufficiency
Priority Management Plan
| Priority | Action |
|---|---|
| Immediate | Lifestyle modification: diet, exercise, weight reduction - can reverse prediabetes |
| Immediate | Start Vitamin D3 supplementation (60,000 IU/week x 8 weeks, then maintenance) |
| Soon | Statin therapy discussion with physician - given LDL 144 + prediabetes |
| Soon | OGTT (75g oral glucose tolerance test) - better characterise glucose status |
| Soon | Serum ferritin + iron studies (for borderline anaemia) |
| Soon | Blood pressure measurement, waist circumference (complete metabolic syndrome assessment) |
| Follow up | ANA result - if positive, rheumatology referral for Sjögren's workup |
| Follow up | Repeat HbA1c in 3-6 months after lifestyle changes |
| Refer | Neurology or Diabetologist for formal neuropathy assessment (NCS/EMG, IENFD skin biopsy) |
| Refer | Dermatology for skin biopsy of abdominal lesions |
Note for the physician: The absence of frank diabetes (fasting glucose is normal at 97 mg/dL) does not exclude prediabetic neuropathy. HbA1c-based prediabetes with small-fiber neuropathy is well-documented in the literature. Early aggressive lifestyle intervention in this window can prevent progression to diabetes and potentially reverse the neuropathy.
Utkarsh small finance bank rating and review compared to other small finance bank and is it safe
Utkarsh Small Finance Bank credit rating financial health 2025 2026
small finance bank comparison safety rating India 2025 NPA CRAR
Utkarsh SFB vs AU Jana Equitas ESAF small finance bank comparison NPA CRAR deposits 2025 2026
https://www.careratings.com/upload/CompanyFiles/PR/202601120…
DICGC deposit insurance small finance bank safety India 5 lakh protection 2025
https://groww.in/blog/top-small-finance-bank-stocks-in-india
Utkarsh Small Finance Bank - Rating, Review & Safety Analysis
Quick Profile
| Parameter | Details |
|---|---|
| Full Name | Utkarsh Small Finance Bank Limited (USFBL) |
| Headquarters | Varanasi, Uttar Pradesh |
| Founded | 2009 (as MFI); SFB licence from RBI in 2017 |
| Listed | BSE & NSE (IPO: July 2023) |
| Market Cap | ~₹2,731 crore (Dec 2025) |
| Deposits | ₹21,087 crore (Dec 2025) |
| Loan Book | ₹18,306 crore (Dec 2025) |
| Branches | ~900+ across UP, Bihar, and other states |
| Focus | Microfinance / JLG loans + retail banking |
Credit Ratings (Most Recent - January 2026)
| Rating Agency | Instrument | Rating | Outlook | Action |
|---|---|---|---|---|
| CARE Ratings | Tier-II Bonds (₹200 cr) | CARE A | Negative | Downgraded from CARE A+; Outlook revised from Stable to Negative |
| ICRA | Subordinated Debt (₹400 cr) | [ICRA]A (Negative) | Negative | Downgraded from [ICRA]A+ (Negative) |
| ICRA | Certificates of Deposit (₹1,000 cr) | [ICRA]A1+ | - | Reaffirmed |
- 'A' rating = good credit quality, but not the highest tier
- Negative outlook = rating may be downgraded further if things don't improve
- Both major agencies downgraded the bank's long-term rating in August 2025
- Short-term liquidity (A1+) is still strong - the bank can pay its short-term obligations
Key Financial Metrics (Latest Available - Dec 2025 / H1FY26)
| Metric | Utkarsh SFB | Ideal Range |
|---|---|---|
| CRAR (Capital Adequacy) | 20.1% (Dec 2025) | RBI minimum: 15% |
| Gross NPA ratio | ~12.42% (Sep 2025) | <5% preferred |
| Net NPA ratio | Elevated | <2% preferred |
| NNPA/Net Worth | 41.10% (Sep 2025) | <20% preferred |
| Provision Coverage Ratio | ~59-69% (microfinance book) | >70% preferred |
| LCR (Liquidity Coverage) | 241% | Minimum: 100% |
| CASA ratio | ~20% (Jun 2025) | 25-30%+ preferred |
| Net Interest Margin | ~5.4% (9MFY26) | Good for SFB |
| Net Loss (H1FY26) | ₹588 crore loss | - |
| Net Loss (Q3FY26) | ₹375 crore loss | - |
Red flags clearly visible:
- GNPA of 12.42% is very high - nearly 1 in 8 loans is non-performing
- The bank reported a net loss of ₹588 crore in H1FY26 vs profit of ₹498 crore in FY24
- Stress is concentrated in its microfinance/JLG book (44% of loans), which was affected by the MFIN Guardrail 2.0 regulations from April 2025
Green flags:
- Capital adequacy at 20.1% - well above the 15% minimum; raised ₹950 crore via rights issue (Nov 2025)
- Liquidity coverage ratio at 241% - very strong; no liquidity stress
- Deposit franchise stable - deposits reached ₹21,487 crore; 74% retail deposits
- Fresh NPA slippages declining in Q3FY26 - management says stress has peaked
- Pivoting from microfinance (62% → 44%) toward secured lending (housing, MSME, CV loans)
Comparison with Other Small Finance Banks
| SFB | Market Cap | Deposits | Gross NPA | CRAR | Credit Rating | Status |
|---|---|---|---|---|---|---|
| AU SFB | ₹73,173 cr | ₹1,38,420 cr | ~2.3% | ~20%+ | AA- / High | Best in class |
| Ujjivan SFB | ₹10,501 cr | ₹42,223 cr | Moderate | Adequate | A+ range | Recovering well |
| Equitas SFB | ₹6,817 cr | ₹43,668 cr | ~2.9% | Adequate | A+ range | Good |
| Jana SFB | ₹4,395 cr | ₹33,733 cr | Elevated | Adequate | A range | Watch |
| Utkarsh SFB | ₹2,732 cr | ₹21,087 cr | ~12.4% | 20.1% | A (Negative) | Under stress |
| ESAF SFB | Small | ₹24,006 cr | Elevated | Adequate | A range | Under stress |
| Capital SFB | Small | ~₹8,000 cr | Low | Good | - | Niche/stable |
- 🟢 AU SFB - Best asset quality, largest, AA- rated
- 🟢 Equitas SFB - Good asset quality, Chennai-based
- 🟢 Ujjivan SFB - Recovering well, wide network
- 🟡 Jana SFB - Moderate stress, watch carefully
- 🟠 Utkarsh SFB - High NPA, under stress but well-capitalised
- 🟠 ESAF SFB - High microfinance exposure, similar stress profile
Is Utkarsh SFB Safe for Deposits?
For deposits up to ₹5 lakh - YES, Safe
Every depositor is insured up to ₹5,00,000 (principal + interest combined) per bank, regardless of what happens to the bank.
For deposits above ₹5 lakh - Exercise Caution
- GNPA of 12.42% is a significant concern - among the highest in the SFB sector
- The bank is posting net losses (₹375 crore in Q3FY26 alone)
- Both CARE and ICRA have Negative outlooks, meaning further downgrades are possible
- The microfinance sector stress is industry-wide, but Utkarsh has higher exposure than peers
- Capital adequacy (20.1%) is robust - the bank has a substantial buffer to absorb losses
- Liquidity is strong (LCR 241%) - no risk of a liquidity crisis
- ₹950 crore rights issue completed in November 2025 - shareholders have backed the bank
- RBI-regulated and monitored - SFBs face stricter oversight than cooperative banks
- Fresh NPAs declining - management reports Q3FY26 stress is peaking out
Practical Guidance
| Situation | Recommendation |
|---|---|
| FD under ₹5 lakh | Safe (DICGC insured). Utkarsh offers competitive FD rates (typically 7.5-9%+). Can consider. |
| FD above ₹5 lakh | Consider spreading across multiple banks to stay within ₹5L per bank, or choose a higher-rated bank (AU SFB, Equitas) for the excess amount |
| Large corporate/institutional deposits | Not recommended currently given Negative outlook |
| Long-term FD (3-5 years) | Be cautious - wait for Q4FY26 results to see if NPA trend reverses before committing large sums |
| Savings account | Fine for regular use |
Bottom Line
- For small depositors (≤₹5 lakh): It is fully safe due to DICGC insurance, and its FD rates are attractive.
- For larger deposits: AU SFB or Equitas/Ujjivan are safer choices at this time.
- The bank's recovery depends on whether its microfinance NPA stabilises in Q4FY26 and FY27 - watch for the next quarterly results.
What about sarvoday and Shivalik
Suryoday Small Finance Bank rating NPA CRAR financial health 2025 2026 ICRA CARE
Shivalik Small Finance Bank rating NPA CRAR financial performance 2025 2026
https://infomericstorage.blob.core.windows.net/uploads/pr_Sh…
Suryoday & Shivalik Small Finance Banks - Full Analysis
SURYODAY Small Finance Bank
Quick Profile
| Parameter | Details |
|---|---|
| HQ | Navi Mumbai, Maharashtra |
| Started as SFB | 2017 |
| Listed | BSE & NSE (Scrip: SURYODAY) |
| Focus | Microfinance (Individual Finance / JLG), MSME, home loans |
| Geographic Strength | Maharashtra, Tamil Nadu, Odisha |
| Customers | ~38 lakh clients |
| Deposits | ~₹13,000 crore (Dec 2025) |
| Advances | ~₹12,000 crore (Dec 2025) |
| Total Assets | ₹17,039 crore |
Credit Ratings (March 2026 - Most Recent)
| Agency | Instrument | Rating | Outlook | Action |
|---|---|---|---|---|
| ICRA | Subordinated Debt (₹100 cr) | [ICRA]A (Stable) | Stable | Reaffirmed |
| ICRA | Certificates of Deposit (₹130 cr) | [ICRA]A1+ | - | Reaffirmed |
Key difference from Utkarsh: Suryoday's outlook is Stable, not Negative. This means ICRA does not expect further downgrades in the near term.
Key Financial Metrics
| Metric | FY2024 | FY2025 | 9M FY2026 (Dec 25) |
|---|---|---|---|
| CRAR | 28.4% | 25.8% | 21.9% |
| Tier I (CET1) | 26.5% | 24.5% | 21.0% |
| Gross NPA | 2.9% | 7.2% | 6.7% ↓ improving |
| Net NPA | 0.9% | 4.6% | 4.3% |
| PAT (Profit) | ₹216 cr | ₹115 cr | ₹102 cr (9 months) |
| ROA | 1.9% | 0.8% | 0.8% |
| CASA ratio | ~20% | 21% | 21% |
| Net profit Q3FY26 | - | - | ₹36.56 cr ↑ (up 9.79% YoY) |
Strengths
- Still profitable - unlike Utkarsh which posted huge losses, Suryoday is making a profit, albeit smaller than before (₹36.56 cr in Q3FY26, up 9.79% YoY)
- GNPA is improving - peaked at 7.2% in March 2025, now declining to 6.7% in Dec 2025
- CGFMU guarantee cover - a standout feature: 98% of its microfinance portfolio is covered by the Credit Guarantee Fund for Micro Units (CGFMU). This means the government backstops most microfinance losses - a significant risk mitigant not shared by all SFBs
- CRAR of 21.9% - well above 15% minimum; Tier I at 21%, very strong
- Stable outlook on ICRA rating - no imminent downgrade risk
- Strong deposit growth - deposits up 32.5% YoY to ~₹13,000 crore
- Slippages reducing sharply - ₹206 cr → ₹155 cr quarter-on-quarter in Q3FY26
- X-bucket collection efficiency at 99.5% (Dec 2025) - nearly fully collecting on current loans
Weaknesses
- GNPA of 6.7% is still elevated (though improving)
- CASA ratio of 21% is low - means higher cost of funds
- Profitability still under pressure vs pre-stress levels (ROA at 0.8% vs 1.9% in FY24)
- Concentrated in Maharashtra/Tamil Nadu/Odisha - geographic concentration risk
FD Rates (Indicative, April 2026)
- Regular: ~8.25% p.a. (1-year)
- Senior Citizens: ~8.75% p.a.
Suryoday Safety Assessment
| Factor | Status |
|---|---|
| DICGC Insurance (≤₹5L) | ✅ Fully protected |
| Rating | A (Stable) - Good |
| Capital Buffer | ✅ Very strong (CRAR 21.9%) |
| Profitability | ⚠️ Reduced but still positive |
| NPA trend | ✅ Improving (peaked and declining) |
| Unique protection | ✅ 98% microfinance covered by CGFMU guarantee |
SHIVALIK Small Finance Bank
Quick Profile
| Parameter | Details |
|---|---|
| HQ | Saharanpur, Uttar Pradesh |
| Origin | Converted from Shivalik Mercantile Co-operative Bank (est. 1997) |
| Started as SFB | April 26, 2021 (newest among major SFBs) |
| Listed | Not publicly listed (unlisted bank) |
| Focus | MSME, agriculture, retail loans; originally Punjab/Haryana/UP focused |
| Branches | 215 branches across 105 districts, 7 states |
| Deposits | ₹4,218 crore (Dec 2025) |
| Advances | ₹4,007 crore (Dec 2025) |
| Size | Smallest among notable SFBs |
Credit Rating (February 2026 - Most Recent)
| Agency | Instrument | Rating | Outlook | Action |
|---|---|---|---|---|
| Infomerics | Tier-II Bonds (₹50 cr) | IVR A / Stable | Stable | Reaffirmed; Outlook revised from Positive → Stable |
Note: Shivalik is rated by Infomerics (smaller agency), not ICRA/CARE/CRISIL. This is because of its smaller size. The outlook was downgraded from Positive to Stable in Feb 2026 - a mild negative signal.
Key Financial Metrics
| Metric | FY2024 | FY2025 | 9M FY2026 (Dec 25) |
|---|---|---|---|
| CRAR | 20.19% | 20.95% | 20.80% |
| Gross NPA | 2.01% | 2.70% | 2.80% |
| Net NPA | 0.84% | 1.51% | 2.10% |
| PAT (Profit) | ₹2.40 cr | ₹0.95 cr | ₹4.50 cr (9 months) |
| NIM | 5.95% | 5.46% | 4.80% ↓ |
| ROA | 0.09% | 0.03% | 0.10% |
| CASA | 27.98% | 22.42% | 20.35% ↓ declining |
| LCR | - | - | 171.42% |
| Total Business | ₹4,530 cr | ₹6,131 cr | ₹8,225 cr |
Strengths
- GNPA of only 2.80% - best asset quality in this comparison; did NOT have heavy microfinance exposure, so largely escaped the 2024-26 MFI crisis
- CRAR of 20.80% - solid capital adequacy
- Profitable (₹4.50 cr PAT in 9M FY26 vs ₹0.95 cr full FY25) - recovering profitability
- LCR 171.42% - adequate liquidity
- Strong parentage - converted from a cooperative bank with 25+ years history; strong local trust base in UP/Punjab/Haryana
- SMBC Asia Rising Fund as institutional investor - adds credibility
- Rapidly growing - total business grew from ₹4,530 cr (FY24) to ₹8,225 cr (9M FY26) - nearly doubling in 2 years
- Unaffected by MFI crisis - because its loan book is predominantly MSME, agri, and secured retail, not JLG microfinance
Weaknesses
- Very small bank - ₹4,218 cr deposits vs ₹21,000+ cr for Utkarsh; limited scale
- Extremely low profitability - ROA of 0.10% is among the weakest; profits are tiny in absolute terms
- Relies on equity infusions to maintain capital - internal generation is insufficient; SMBC Asia fund keeps injecting capital (₹96 cr in FY25, ₹102 cr in 9M FY26)
- CASA declining - from 27.98% (FY24) to 20.35% (Dec 2025) - costlier deposits
- NIM compressing - from 5.95% to 4.80% - margin pressure
- Geographic concentration - still heavily Punjab/UP dependent (though expanding)
- Unlisted - no market price discovery; less transparency
- Smaller rating agency (Infomerics) - less widely tracked
Shivalik Safety Assessment
| Factor | Status |
|---|---|
| DICGC Insurance (≤₹5L) | ✅ Fully protected |
| Rating | A/Stable (Infomerics) - Adequate |
| Capital Buffer | ✅ Good (CRAR 20.80%) |
| Asset Quality | ✅ Best among stressed-SFB peers (GNPA 2.8%) |
| Profitability | ⚠️ Very thin but positive |
| Size/Scale | ⚠️ Small; limited systemic importance |
Full Comparison Table (All Major SFBs)
| SFB | GNPA | CRAR | Rating | Outlook | Profit | Size | Depositor Safety |
|---|---|---|---|---|---|---|---|
| AU SFB | ~2.3% | ~20%+ | AA-/A+ | Stable | Strong | ₹1.38L cr deposits | 🟢 Excellent |
| Ujjivan SFB | Moderate | Adequate | A+ | Stable | Good | ₹42,223 cr | 🟢 Very Good |
| Equitas SFB | ~2.9% | Adequate | A+ | Stable | Good | ₹43,668 cr | 🟢 Very Good |
| Shivalik SFB | 2.80% | 20.80% | A/Stable | Stable | Thin | ₹4,218 cr | 🟢 Good (small bank) |
| Suryoday SFB | 6.7% ↓ | 21.9% | A/Stable | Stable | Positive | ₹13,000 cr | 🟡 Moderate-Good |
| Jana SFB | Elevated | Adequate | A range | Watch | Pressure | ₹33,733 cr | 🟡 Moderate |
| Utkarsh SFB | 12.42% | 20.1% | A/Negative | Negative | Loss-making | ₹21,087 cr | 🟠 Caution (>₹5L) |
| ESAF SFB | High | Adequate | A range | Negative | Pressure | ₹24,006 cr | 🟠 Caution |
Practical Recommendation
| Your Situation | Best Choice |
|---|---|
| Safety-first depositor, ≤₹5L | Any SFB (all DICGC-insured); go for best FD rate |
| Safety-first, >₹5L | AU SFB > Equitas/Ujjivan > Suryoday > Shivalik > Utkarsh |
| Good rates + decent safety | Suryoday (8.25%) or Shivalik (competitive rates, low NPA) |
| North/UP-based, local trust | Shivalik - strong co-op legacy, low NPA |
| Recovery play (risk-tolerant) | Utkarsh or ESAF - high stress now but may recover |
Bottom line: Suryoday is better positioned than Utkarsh right now - still profitable, NPA declining, CGFMU guarantee is unique protection. Shivalik is the hidden gem for low NPA quality, but is very small. For deposits above ₹5 lakh, Suryoday or AU/Equitas are preferable over Utkarsh at this stage.