I now have comprehensive, authoritative content. Let me compile the full answer.
Myasthenia Gravis (MG)
Definition
MG is the most common primary disorder of neuromuscular transmission (NMT). Autoantibodies bind to proteins at the neuromuscular junction (NMJ) - most commonly the acetylcholine receptor (AChR) - disrupting normal NMT and producing fatigable muscle weakness that worsens with activity and improves with rest.
- Bradley and Daroff's Neurology in Clinical Practice
Epidemiology
- US prevalence ~20/100,000 (~60,000 patients total)
- Women affected ~3x more than men before age 40; incidence higher in males after age 50
- Bimodal distribution: peaks in the 20s (young women) and 60s (older men)
- Prevalence has been increasing over the past 50 years, partly due to improved diagnosis and increased longevity
Pathophysiology
The NMJ lacks a blood-nerve barrier, making it vulnerable to circulating immune factors.
Mechanism of antibody-mediated injury:
- Anti-AChR antibodies (IgG) target the α-subunit of the nicotinic AChR - specifically the main immunogenic region (MIR)
- Antibodies cause disease by:
- Activating complement → lysis of the postsynaptic muscle membrane
- Cross-linking AChRs → accelerated receptor degradation
- Blocking ACh binding directly
- Net result: reduced AChR density at junctional folds → decreased amplitude of miniature endplate potentials (MEPPs) → failure of neuromuscular transmission
Antibody subtypes:
| Antibody | Frequency | Features |
|---|
| Anti-AChR | 80-90% of generalized MG; 50% of ocular MG | Gold standard |
| Anti-MuSK (muscle-specific tyrosine kinase) | ~5-8% of AChR-seronegative cases | More prominent facial/bulbar weakness, more severe |
| Anti-LRP4 (lipoprotein receptor-related protein 4) | 1-3% | Mild-moderate symptoms |
Thymus role: Thymic hyperplasia or thymoma is found in ~10% of MG patients. Thymic cells express nicotinic AChRs; thymoma-associated MG almost invariably has anti-AChR antibodies (not anti-MuSK or LRP4). Patients with thymoma may also have antibodies against titin and ryanodine receptor.
- Medical Physiology and Bradley and Daroff's Neurology in Clinical Practice
Clinical Features
Hallmark
Fatigable weakness - worst at end of day or after sustained effort, better with rest
Initial Symptoms
- Ptosis and diplopia in ~2/3 of patients at onset (virtually all develop ocular symptoms within 2 years)
- Difficulty chewing, swallowing, or talking (bulbar) in ~1/6
- Limb weakness in ~10%
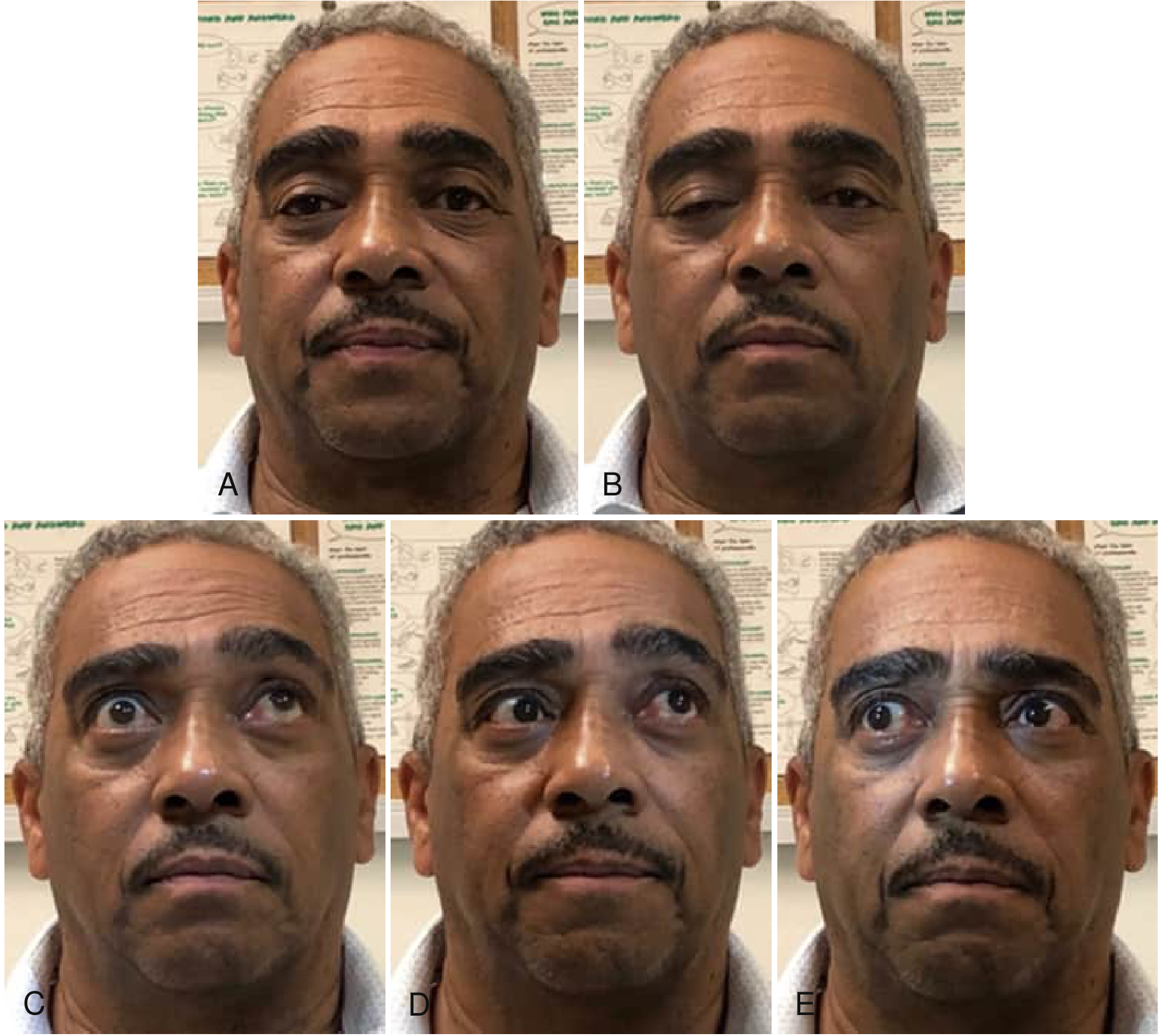
Ocular MG
- Ptosis (unilateral or bilateral, often asymmetric)
- Diplopia from ophthalmoplegia - any pattern of extraocular muscle weakness
- Remains ocular-only in ~10-15% (up to 58% in Asian populations, especially children)
Fig: Ocular motility abnormalities in MG - progressive right lid ptosis during sustained forward gaze (A→B), incomplete upward gaze (C), skew deviation on left lateral gaze (D), and incomplete movement on right lateral gaze (E). - Bradley and Daroff's Neurology
Generalized MG
- Progresses to facial, oropharyngeal, and limb muscles in most patients
- Maximum weakness within the first year in 2/3 of patients
- Bulbar symptoms: dysphagia (oral, pharyngeal, esophageal), dysarthria, dysphonia
- Aspiration (often silent) in ≥35% of MG patients with dysphagia
- Facial weakness: expressionless, "snarling" smile
- Neck weakness: difficulty holding head up
- Limb weakness: proximal > distal
Factors that worsen MG
Emotional upset, systemic illness (especially viral respiratory infections), hypothyroidism or hyperthyroidism, pregnancy, menstrual cycle, surgery, fever, and certain medications (aminoglycosides, fluoroquinolones, beta-blockers, magnesium, neuromuscular blocking agents)
Myasthenic Crisis
Life-threatening respiratory failure from respiratory muscle weakness. Dysphagia is a major precipitant in ~56% of crises. Requires ICU admission, mechanical ventilation, and urgent immunotherapy (plasma exchange or IVIG).
Diagnosis
1. Clinical pattern - fatigable, fluctuating weakness in characteristic distribution
2. Serological testing
- Anti-AChR antibodies (binding, blocking, modulating)
- Anti-MuSK (if AChR negative)
- Anti-LRP4 (if both negative)
3. Electrophysiology
- Repetitive nerve stimulation (RNS): decremental response (>10% decrement at 3 Hz) - characteristic of postsynaptic NMJ disorder
- Single-fiber EMG (SFEMG): most sensitive test - increased jitter and blocking
4. Edrophonium (Tensilon) test - short-acting AChE inhibitor; transient improvement in ptosis/diplopia confirms NMJ disorder (less used now due to side effects)
5. Imaging - CT/MRI chest for thymoma in all patients
Treatment
1. Symptomatic: Acetylcholinesterase (AChE) Inhibitors
- Pyridostigmine (Mestinon) - first-line symptomatic treatment
- Inhibits AChE → prolongs ACh availability at the reduced number of receptors
- Caution: overdose causes cholinergic crisis (overstimulation → prolonged depolarization → Na+ channel inactivation → synaptic blockade)
2. Immunosuppression (long-term disease modification)
- Corticosteroids (prednisone) - most commonly used first-line immunosuppressant
- Azathioprine - slow onset (6-12 months), effective steroid-sparing agent
- Mycophenolate mofetil
- Methotrexate
- Cyclosporine/Tacrolimus
- Rituximab - particularly effective in anti-MuSK MG (see recent evidence below)
3. Rapid Immunomodulation (crisis/perioperative)
- Plasma exchange (PLEX/plasmapheresis) - removes circulating antibodies; effect within days
- IV Immunoglobulin (IVIG) - similar efficacy to PLEX; safer in patients with hemodynamic instability
4. Novel Biologics (expanding rapidly)
- Eculizumab (anti-C5 complement inhibitor) - approved for AChR+ generalized MG
- Efgartigimod (FcRn antagonist - reduces IgG levels including AChR antibodies)
- Rozanolixizumab, Nipocalimab (other FcRn antagonists)
- Zilucoplan (anti-C5)
5. Thymectomy
- Recommended for all patients with thymoma
- Also beneficial in non-thymomatous generalized AChR+ MG (especially age <60, within 5 years of onset) - improves long-term outcomes
MG Classification (Osserman/MGFA)
| Class | Description |
|---|
| I | Ocular only |
| II | Mild generalized |
| III | Moderate generalized |
| IV | Severe generalized |
| V | Myasthenic crisis (intubation) |
Recent Evidence (2024-2026)
A
2025 Cochrane systematic review on rituximab for MG and a
2025 network meta-analysis comparing novel biologics show expanding evidence for targeted therapies - particularly rituximab in MuSK+ MG and FcRn antagonists (efgartigimod, rozanolixizumab) showing strong efficacy for generalized MG with favorable safety profiles. These newer agents are increasingly being positioned earlier in the treatment algorithm for refractory or severe cases.
Key Differentials
| Feature | MG | Lambert-Eaton (LEMS) | Botulism |
|---|
| Antibody target | Postsynaptic AChR | Presynaptic VGCC | Presynaptic (toxin) |
| Reflexes | Normal | Reduced (improve post-exercise) | Reduced |
| Autonomic features | No | Yes | Yes |
| Associated cancer | Thymoma | SCLC | No |
| Response to repetitive stim | Decrement | Increment | Decrement |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Medical Physiology (Boron & Boulpaep)