Choledochoduodenostomy Steps anatomy indications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have everything needed for a thorough answer. Here is the full structured response:
Choledochoduodenostomy
A side-to-side anastomosis between the common bile duct (CBD) and the first or second part of the duodenum, creating a biliary-enteric bypass that diverts bile flow around a distal CBD obstruction.
Relevant Anatomy
The procedure exploits the proximity of the supraduodenal CBD to the postbulbar duodenum:
- Common bile duct: Runs in the hepatoduodenal ligament (anterior to portal vein, lateral to hepatic artery). The supraduodenal segment is the operative target - it is anterior and medial, accessible once the peritoneum over it is incised.
- Postbulbar duodenum (D1-D2 junction): Lies immediately adjacent and slightly inferior/posterior to the CBD. The retroduodenal portion is the ideal anastomotic site.
- Kocher maneuver: Mobilization of the duodenum medially by incising the lateral peritoneal reflection is mandatory - it brings the postbulbar duodenum into proximity with the CBD without tension, and allows full assessment of the distal duct.
- Ductal blood supply: Runs at the 3 o'clock and 9 o'clock positions along the bile duct. Longitudinal choledochotomy (rather than transverse) avoids devascularization.
- Hepatic artery: The right hepatic artery typically crosses behind the CBD - injury risk during duct exposure must be kept in mind.
Indications
Per Fischer's Mastery of Surgery, the indications are:
| Indication | Detail |
|---|---|
| Dilated CBD from benign distal obstruction | CBD >2 cm indicates prolonged obstruction/loss of tone with biliary stasis; size alone is a relative indication |
| Failed endoscopic sphincterotomy | When ERCP has not cleared the obstruction - this is now the primary scenario since endoscopy is first-line |
| Recurrent CBD stones post-cholecystectomy | Not amenable to repeat endoscopic clearance |
| Numerous CBD stones | >15 stones, or intrahepatic stones |
| Primary CBD stones | Especially after a prior choledochotomy |
| Distal CBD stricture from chronic pancreatitis | Benign inflammatory stricture causing obstruction |
| Previous failed choledochotomy | Unable to clear the duct via exploration alone |
Historically required in ~1% of all biliary operations; more common in elderly patients (mean age 61 years); ~60% are secondary procedures.
Contraindications
- CBD diameter <15 mm - absolute contraindication (anastomosis too small; high risk of stricture and sump syndrome)
- Malignant distal obstruction - these are better managed with Roux-en-Y hepatico- or choledochojejunostomy
- Active pancreatitis (acute or chronic with obstruction) - does not address the underlying cause
- Note: An impacted distal CBD stone was historically considered a contraindication (fear of pancreatitis), but series have shown the risk is quite low
Surgical Technique (Open)
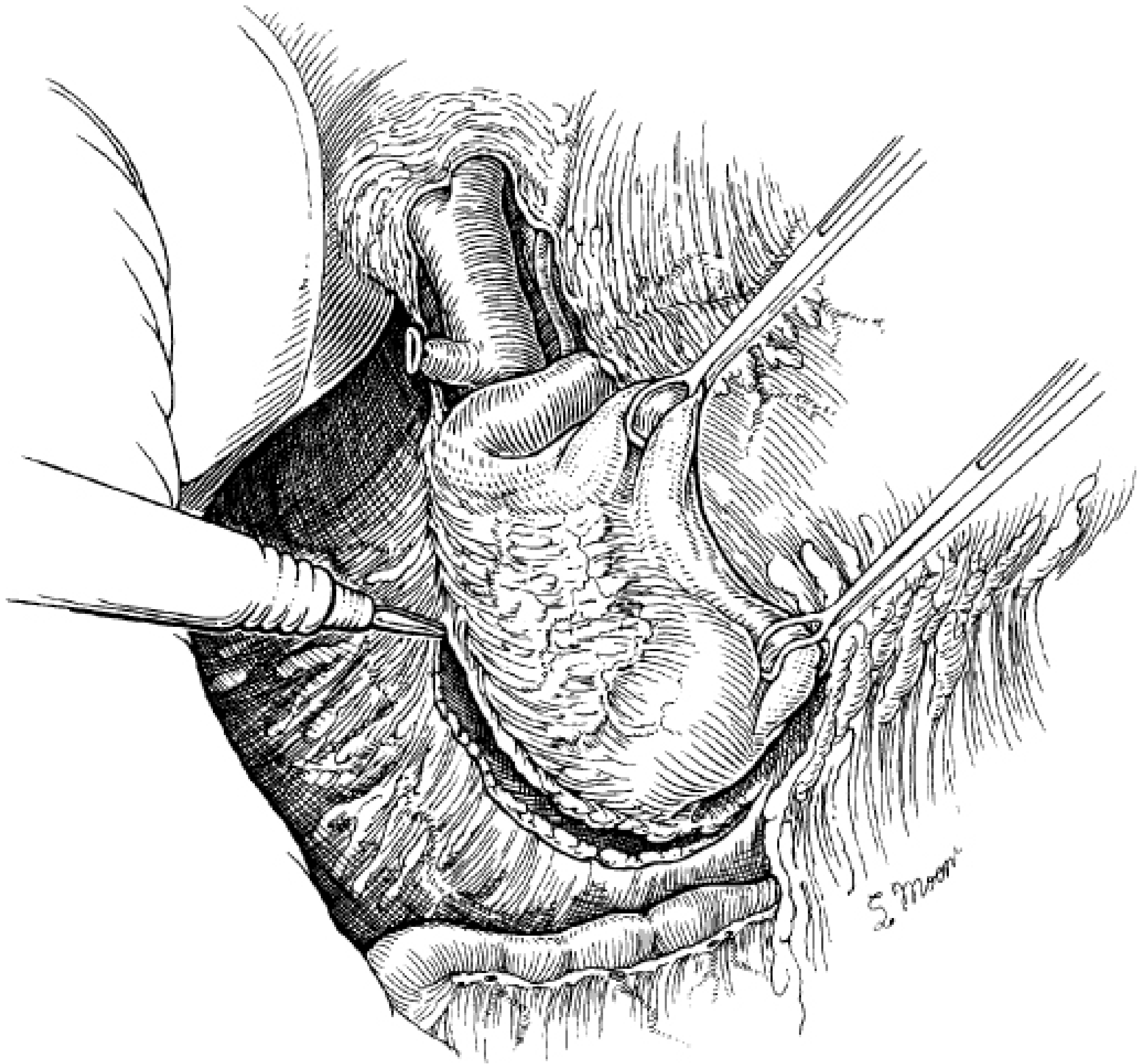
Fig. 168.5 - Wide Kocher maneuver exposes the operative field:
Step-by-Step
Step 1 - Cholecystectomy
Remove the gallbladder first to eliminate cystic duct reflux and decompression issues.
Step 2 - Expose the CBD
Incise the overlying peritoneum of the hepatoduodenal ligament to expose the supraduodenal CBD.
Step 3 - Kocher maneuver
Perform an extended Kocher maneuver - mobilize the duodenum and head of pancreas medially by incising the lateral peritoneal attachment. This is mandatory for adequate exposure and tension-free anastomosis.
Step 4 - Choledochotomy
Open the CBD longitudinally in the supraduodenal location. If findings confirm the indication, extend the incision to 2.0-2.5 cm in the longitudinal axis (this typically extends up to the common hepatic duct). Complete the CBD exploration.
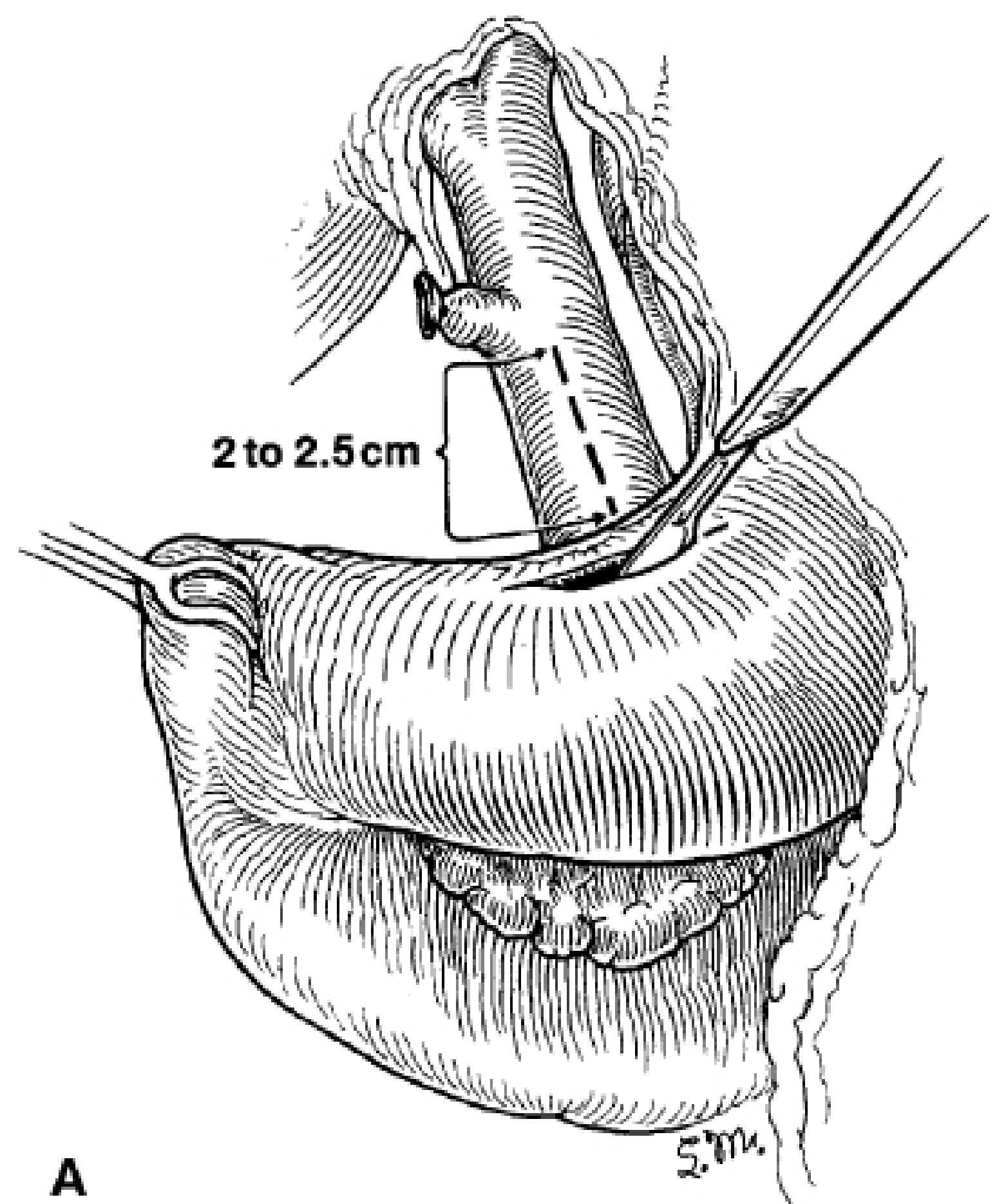
Fig 168.6A: The 2.0-2.5 cm longitudinal choledochotomy and the planned duodenotomy are shown.
Step 5 - Duodenotomy
Make a longitudinal incision in the postbulbar duodenum. Make this incision slightly smaller than the planned stomal size, as duodenal elasticity can over-stretch and cause technical difficulty.
Step 6 - Stay sutures
Place stay sutures at the corners of the planned choledochoduodenal anastomosis. These pass from the end of the duodenal incision. A bisecting suture is placed at the lower end of the choledochotomy at the midpoint of the adjacent duodenum.
Step 7 - Posterior row
Place posterior row of sutures with 4-0 absorbable material (polyglycolic acid), with knots on the internal (luminal) aspect of the anastomosis.
Step 8 - Anterior row
Place anterior row sutures without tying them. Traction holds them in place until all are placed - this prevents inadvertent closure of the posterior wall. Then tie them, starting at the medial side of the anastomosis.
Step 9 - Single layer only
Do not use a double-layer closure - a second layer narrows the anastomotic orifice and defeats the purpose of a wide stoma.
Step 10 - Drain
Place a closed suction drain posterior to the choledochoduodenostomy.
Laparoscopic Approach (Advanced)
- Same principles apply; requires skilled intracorporeal suturing
- A transverse (rather than longitudinal) choledochotomy can be used laparoscopically - but care must be taken not to devascularize the duct (blood supply runs medially and laterally)
- Duodenum is incised longitudinally after Kocher maneuver; side-to-side anastomosis created with 4-0 polyglycolic acid interrupted sutures
- Median operative time ~300 min (vs. ~180 min open) - Maingot's Abdominal Operations
Postoperative Care
- Start with clear liquids, advance to solids as tolerated
- Remove drain when output is non-bilious and low volume
- Monitor for standard postoperative complications (bleeding, DVT, PE, SSI)
Complications
| Complication | Notes |
|---|---|
| Anastomotic stricture | Long-term; manageable endoscopically |
| Sump syndrome | Debris/food collects in the distal blind-end CBD segment below the stoma - causes recurrent cholangitis. Managed with ERCP to clear the distal duct. |
| Anastomotic leak | Treat with IR-guided external drainage |
| Bile reflux / gastritis | More common than with Roux-en-Y hepaticojejunostomy |
Major morbidity rate is ~11% (compared to ~20% for transduodenal sphincteroplasty).
CDD vs. Roux-en-Y Hepaticojejunostomy
- CDD is simpler, faster, and avoids a jejunal limb
- HJ is preferred for malignant obstruction and when the CBD is non-dilated
- Both have better long-term patency than cholecystojejunostomy for benign disease
- HJ has less risk of sump syndrome and bile reflux
Sources: Fischer's Mastery of Surgery, 8th ed., pp. 4655-4658; Maingot's Abdominal Operations, pp. 1105-1106; Mulholland and Greenfield's Surgery, 7th ed., p. 3080
This is a shared conversation. Sign in to Orris to start your own chat.