Give a detailed explanation of flial chest it's etiology pathogenesis clinical features management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"flail chest" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive answer. Let me compile it.
Flail Chest
Definition
Flail chest is the most severe form of blunt thoracic chest wall injury. It occurs when double fractures of three or more contiguous ribs (fracture at two points along each rib), or the combination of sternal and rib fractures, uncouple a segment of the rib cage from the rest of the thoracic wall. The result is a free-floating ("flail") segment that moves independently and paradoxically with respiration. Up to 25% of all rib injuries result in flail chest. — Murray & Nadel's Textbook of Respiratory Medicine
A related but distinct entity is the "non-integrated chest wall": multiple single-plane rib fractures to contiguous ribs that partially — but not fully — uncouple a chest wall segment, producing similar respiratory morbidity.
Etiology
| Cause | Notes |
|---|---|
| Blunt chest trauma (most common) | Motor vehicle accidents and falls account for the vast majority |
| Aggressive CPR | Rib fractures from resuscitation compressions |
| Pathologic rib fractures | Multiple myeloma, metastatic disease |
| Corrective rib resection | Rare iatrogenic cause |
| Congenital rib abnormalities | Extremely rare |
Note on children: Flail chest is uncommon in children because the pediatric chest wall is more compliant. When it does occur in a child, it signifies a far greater degree of trauma than in adults.
— Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's
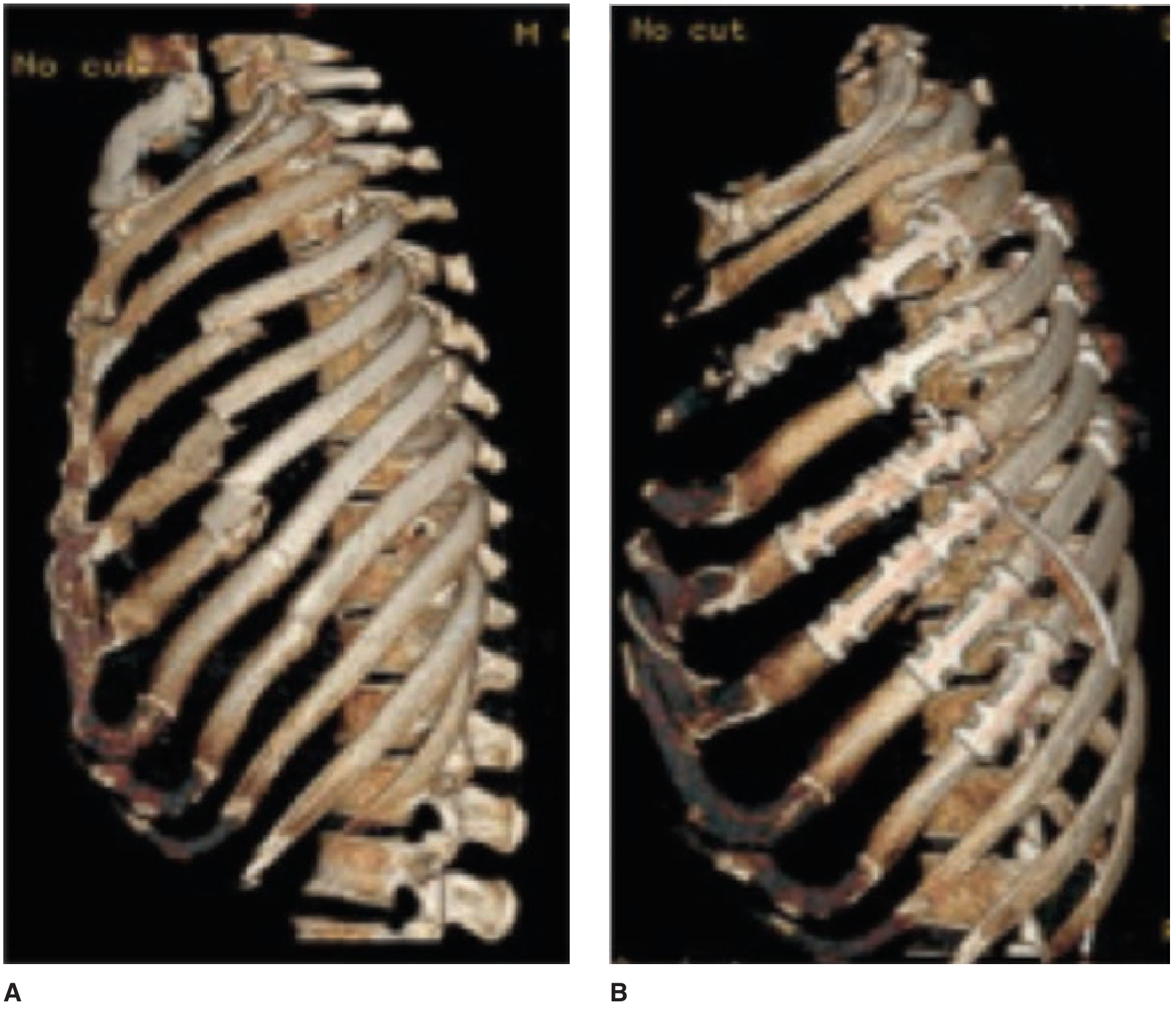
Anatomy of the Flail Segment
Fractures can be anterior, lateral, or posterior:
- Lateral flail — most common location; highest propensity for dislocation after surgical fixation
- Anterior flail — results from separation between the sternum and ribs; costal cartilage separation (costochondral) can also produce it
- Posterior flail — least clinically severe; paraspinal muscles provide significant splinting, limiting paradoxical motion
The 3D CT images below show a flail chest before (A) and after (B) surgical repair with osteosynthesis plates:
Pathogenesis
Respiratory Mechanics (the core mechanism)
Normally, rib cage expansion during inspiration results from coordinated contraction of the diaphragm and intercostal muscles increasing thoracic volume, making pleural pressure subatmospheric. In flail chest, the free segment is uncoupled from this coordinated expansion:
- Inspiration: Pleural pressure decreases (becomes more negative) → flail segment is pulled inward (paradoxical inward motion) while the rest of the chest wall expands outward
- Expiration: Pleural pressure increases (more positive) → flail segment is pushed outward while the rest of the chest wall contracts
This paradox is amplified when lung compliance decreases (from pulmonary contusion or atelectasis), because larger pleural pressure swings are needed for a given tidal volume, worsening the extent of paradoxical motion. Similarly, increased airway resistance (secretions, bronchospasm) worsens the mechanics.
The historical concept of pendelluft (gas swinging back and forth between the injured and uninjured hemithorax) was once thought to cause respiratory failure — this has now been refuted. Paradoxical motion and muscle dysfunction are the key mechanisms. — Murray & Nadel's; Fishman's
How Respiratory Failure Develops (multifactorial)
The pathogenesis of respiratory failure is best understood through the cascade shown below:
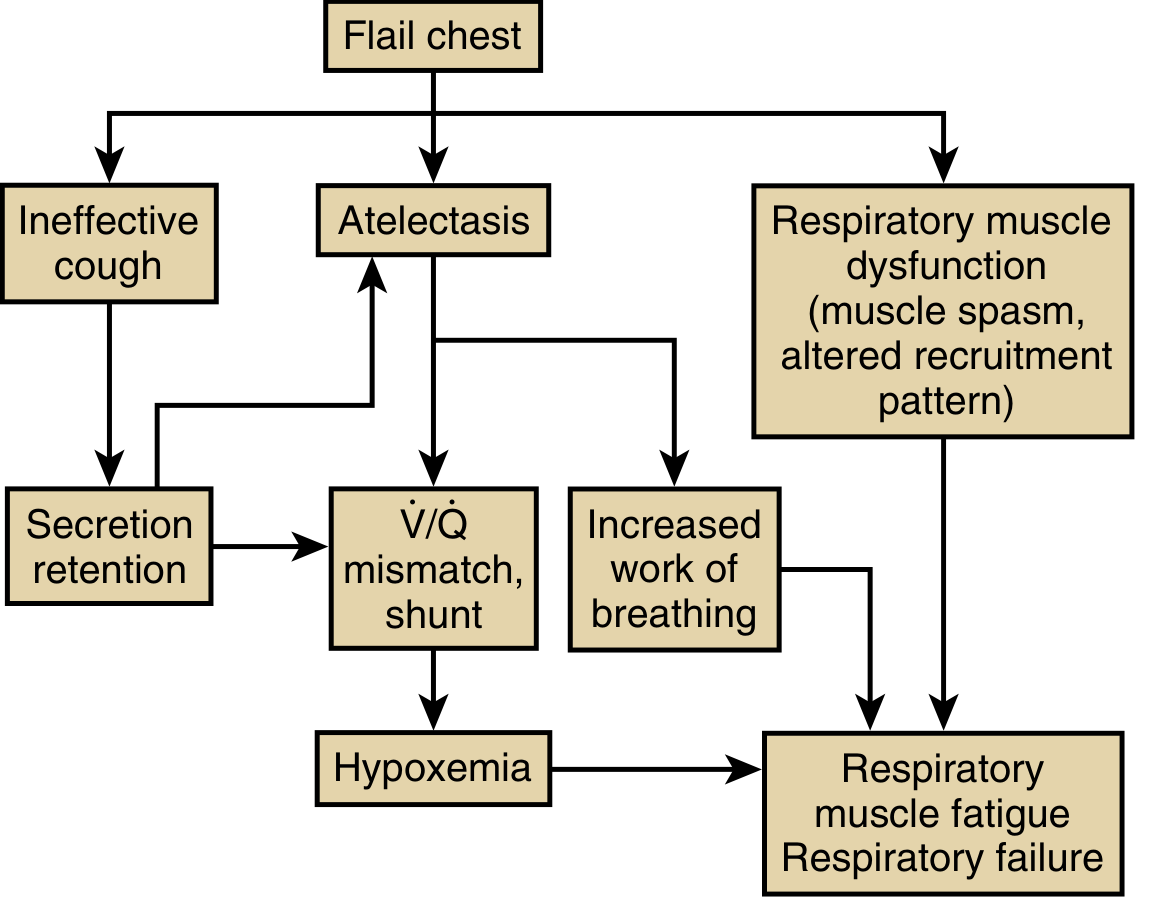
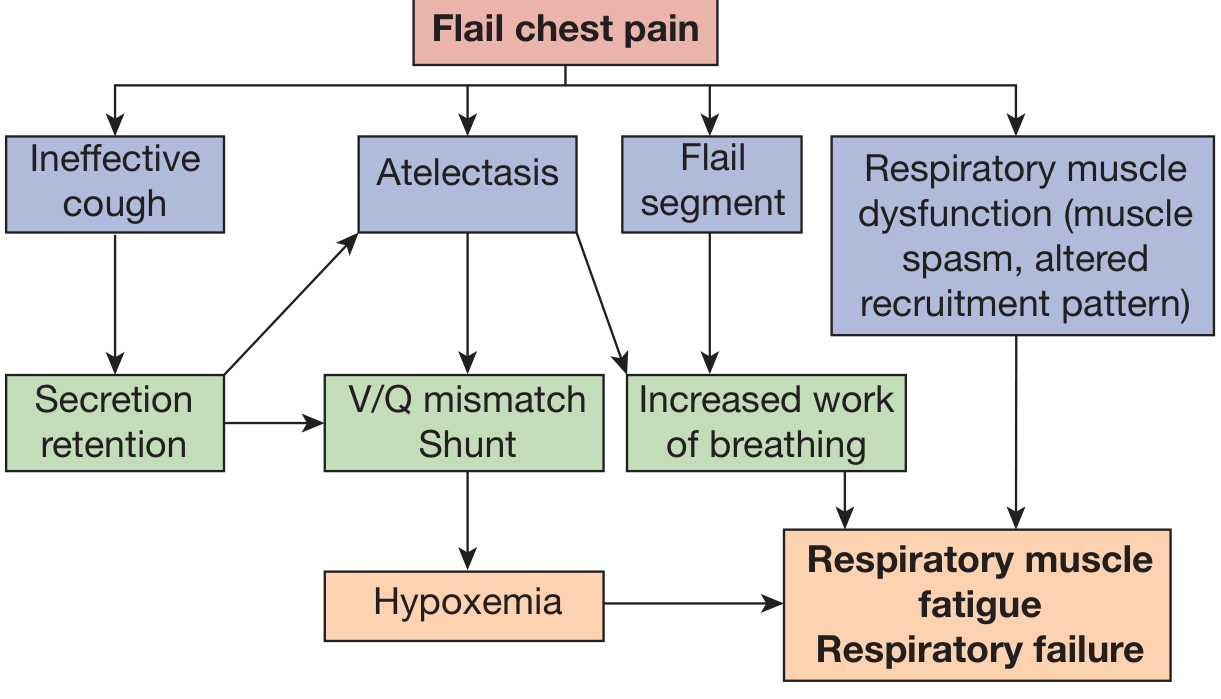
Key mechanisms:
- Pain → shallow breathing → atelectasis: Severe chest wall pain causes patients to take rapid, shallow breaths, impairing cough, promoting mucus plugging, and causing dependent atelectasis
- Increased elastic load: Atelectasis and pulmonary contusion reduce lung compliance, increasing the work the respiratory muscles must do
- Respiratory muscle inefficiency: The inspiratory muscles must shorten more for a given tidal volume because the flail segment "steals" displacement. This extra shortening does not generate airflow at the mouth (wasted work), reduces the mean operating length of inspiratory muscles, and reduces their efficiency — the EMG activity of the external intercostals in the flail region increases more than threefold
- Increased oxygen cost of breathing: Combination of extra work + inefficiency + hypoxemia increases the metabolic demand of the respiratory muscles
- V/Q mismatch and shunt: Atelectasis, secretion retention, and pulmonary contusion all generate intrapulmonary shunts, worsening hypoxemia
- Respiratory muscle fatigue → failure: Hypoxemia feeds back to worsen muscle fatigue; eventually the system decompensates
Pulmonary function tests: Vital capacity (VC) and functional residual capacity (FRC) are acutely reduced to as low as 50% of predicted. In patients with pulmonary contusion complicating flail chest, these reductions may persist for up to 4 years due to fibrosis in the contused area. — Fishman's
Associated Injuries
Flail chest rarely occurs in isolation. The force required to create a flail segment is massive and typically produces:
| Thoracic | Extrathoracic |
|---|---|
| Pulmonary contusion (most important — in up to 60%) | Closed traumatic brain injury (most frequent extrathoracic injury) |
| Hemothorax | Aortic arch rupture |
| Pneumothorax | Splenic/hepatic laceration |
| — | Long bone fractures |
Pulmonary contusion + flail chest carries mortality as high as 56%. — Fishman's
Clinical Features
Symptoms
- Severe chest pain, worse on breathing and movement
- Dyspnea (may develop immediately or progress over several hours — beware late respiratory decompensation)
- Anxiety, air hunger
Signs
| Sign | Detail |
|---|---|
| Paradoxical chest wall movement | The hallmark — affected segment moves in during inspiration, out during expiration. May only be detected by palpation in subtle cases |
| Tachypnea with shallow breathing | Splinting pattern |
| Tachycardia | Pain + hypoxemia |
| Hypoxemia | SpO₂ ↓, PaO₂ < 80 mmHg on air |
| Hypercapnia (late sign) | Indicates ventilatory failure, impending collapse |
| Crepitus over fractures | Palpable/audible |
| Surgical emphysema | If pneumothorax/alveolar rupture present |
| Reduced breath sounds | Hemothorax, pneumothorax, or consolidation |
In the mechanically ventilated and sedated patient, paradoxical motion may be completely absent and diagnosis is delayed until sedation is withdrawn and spontaneous breathing resumes. — Murray & Nadel's
The RibScore (severity stratification)
Points are assigned for:
- ≥6 rib fractures
- ≥3 bicortical displaced fractures
- ≥1 fracture in each anatomic area
- Flail chest
- Bilateral fractures
- First rib fracture
Higher scores predict adverse pulmonary outcomes and help identify patients who benefit from surgical stabilization. — Current Surgical Therapy 14e
Diagnosis
Clinical
Paradoxical rib cage motion on inspection/palpation in a spontaneously breathing patient.
Imaging
- Chest X-ray: Confirms multiple rib fractures but misses approximately 50% of fractures, especially at the costochondral junction
- CT chest with 3D reconstruction (gold standard): Best imaging modality — identifies all fractures, maps extent of injury, reveals pulmonary contusion, hemothorax, pneumothorax, and vascular injury
- CT also allows surgical planning for fixation
Pulmonary Function Monitoring
Sequential measurements of forced vital capacity (FVC), tidal volume (VT), and maximal inspiratory force are useful to predict which patients will require ventilatory support.
Management
The restoration of anatomic and functional integrity of the chest wall is the central therapeutic goal. Management is stratified by severity.
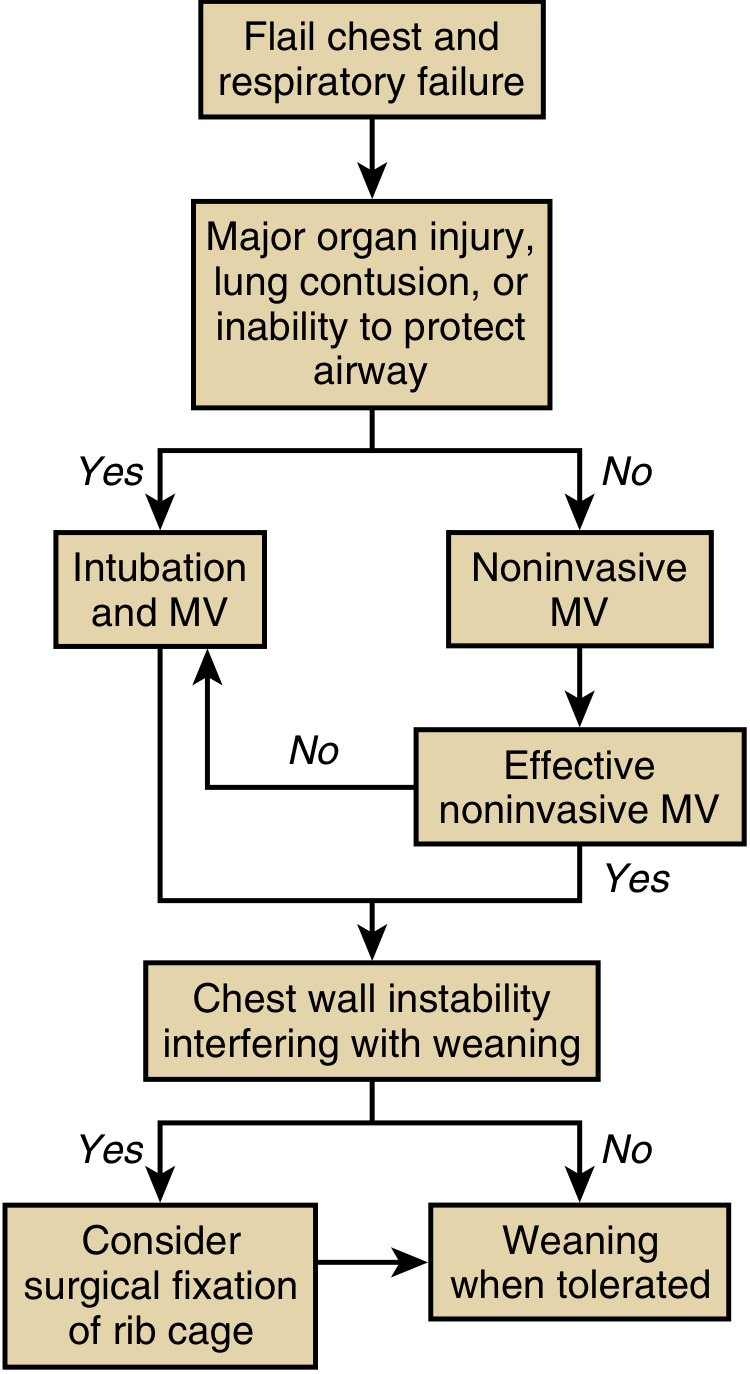
Overview Algorithm
1. Supportive / Conservative (Non-operative)
The majority of patients are managed non-operatively. This strategy is based on three pillars:
A. Pain Control (most critical)
Pain is the driver of atelectasis, secretion retention, and respiratory failure. Multimodal analgesia is preferred to reduce opioid dependence:
| Method | Notes |
|---|---|
| Epidural analgesia (preferred) | Superior to all other methods; decreases ventilator days, pneumonia, ICU/hospital stay. Strongly recommended by guidelines for patients ≥65 years with ≥4 rib fractures |
| Paravertebral / paracostal catheter | Continuous local anesthetic infusion (e.g., 0.25% bupivacaine bolus 20 mL, then 0.125% at 12 mL/h); effective alternative to epidural |
| Intercostal nerve blocks | Useful adjunct |
| IV/PCA opioids | Second-line; avoid as sole agent due to respiratory depression and dependency risk |
| NSAIDs (ibuprofen 800 mg q6h) | Part of multimodal regimen |
| Gabapentin, benzodiazepines | Adjuncts (see multimodal box) |
Absolute contraindications to epidural: raised ICP, local infection, inability to maintain position. Relative: prior spine surgery, spinal fracture, severe cardiac valvular disease, coagulopathy.
B. Pulmonary Toilet
- Aggressive incentive spirometry
- Early ambulation
- Chest physiotherapy
- Supplemental oxygen (target SpO₂ >90%)
C. Fluid Management
Cautious IV fluid replacement to avoid exacerbating pulmonary contusion edema.
D. Treatment of Complications
- Hemothorax / pneumothorax: tube thoracostomy
2. Ventilatory Support
If conservative measures fail to maintain adequate gas exchange, positive-pressure ventilation is required. It functions as a pneumatic splint, maintaining positive pleural pressure and abolishing paradoxical motion.
Indications for Early Intubation/Ventilation:
- Shock
- Severe head injury
- Comorbid pulmonary disease
- ≥8 rib fractures
- Age >65 years
- PaO₂ <80 mmHg on supplemental O₂
- Major associated injuries
- Rising respiratory rate + falling tidal volumes
Early intubation reduces mortality compared with waiting until respiratory failure has occurred. — Tintinalli's Emergency Medicine
Noninvasive Ventilation (NIV) — preferred when feasible:
- CPAP/BiPAP via nasal or face mask
- Used in spontaneously breathing patients who can protect their airway and have no major organ injury
- NIV combined with PCA improves gas exchange, allows physiotherapy, and significantly reduces morbidity and mortality vs. invasive ventilation
- A low-impedance ventilator mode (minimizing subatmospheric pleural pressure swings) is optimal when invasive ventilation is used
Invasive Mechanical Ventilation:
- For patients with major organ injury, inability to protect airway, or NIV failure
- Positive-pressure ventilation splints the flail segment, recruits atelectatic lung, and supports the contused parenchyma
- Invasive ventilation solely for chest wall stability (without other indication) is not recommended due to associated morbidity
3. Surgical Stabilization of Rib Fractures (SSRF)
SSRF has gained significant evidence over the past 15 years and is increasingly recommended for selected patients.
Indications (Box 6 — Current Surgical Therapy 14e)
- Flail chest
- Crushed chest with marked chest wall deformity
- Inability to wean from mechanical ventilation due to chest wall instability
- Persistent paradoxical respiratory movement
- Intractable pain
- Open rib fracture
- Rib fracture non-union with chest wall deformity
- Patient undergoing thoracotomy for concurrent injuries
Evidence:
Meta-analyses and RCTs consistently show SSRF (vs. conservative management) achieves:
- Shorter duration of mechanical ventilation
- Shorter ICU and hospital length of stay
- Lower incidence of pneumonia
- Lower mortality rate
- Less need for tracheostomy
- Less chest wall deformity
With surgical stabilization, VC typically returns to normal range within 3 months, vs. the prolonged impairment seen with conservative management.
Surgical Approach:
- Anterior fractures: Submammary incision, pectoralis flap elevation
- Lateral fractures (3–5 ribs): 8–10 cm longitudinal incision over anterior border of latissimus dorsi; serratus anterior split
- Extensive lateral/posterior fractures (≥5 ribs): Standard posterolateral thoracotomy
- Minimally invasive: Thoracoscopic SSRF — growing evidence; allows complete pleural irrigation and evacuation of hemothorax
- Implants used: Judet struts, titanium plates (e.g., claw-type), medullary wires/nails
Complication rate of surgery: 10.3% overall; wound infection ~2.2%; mortality 2.9% (none directly SSRF-related). — Current Surgical Therapy 14e
Prognosis and Outcomes
| Outcome | Data |
|---|---|
| ICU admission rate | >80% |
| Mechanical ventilation rate | >50–59% |
| Overall mortality | 16–33% (higher with pulmonary contusion) |
| Pulmonary contusion + flail mortality | Up to 56% |
| Age >65 years | Strongly associated with increased mortality |
| Long-term disability | Chest tightness, pain, exertional dyspnea in survivors |
| VC impairment with contusion | Can persist up to 4 years |
Summary
Flail chest is a life-threatening chest wall injury defined by paradoxical motion of an uncoupled rib segment. Its pathophysiology revolves around pain-driven atelectasis, V/Q mismatch, respiratory muscle inefficiency, and — critically — associated pulmonary contusion rather than the flail motion itself. Management requires aggressive multimodal analgesia (epidural preferred), pulmonary toilet, and early escalation to ventilatory support when needed. SSRF has emerged as a superior option to conservative management in appropriate candidates, with consistent evidence showing improved respiratory and clinical outcomes.
Sources: Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Current Surgical Therapy 14e; Tintinalli's Emergency Medicine; Goldman-Cecil Medicine. Recent meta-analyses: PMID 38945079 (2024), PMID 39910551 (2025).
Hydropneumothorax mbbs surgery explanation for 5m
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
hydropneumothorax chest X-ray air fluid level
Finding Sources
Loading Image
Loading Image
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Make a comparison table: hydropneumothorax vs tension pneumothorax vs simple pneumothorax
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.