Gastric volvulus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastric volvulus"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have everything needed for a comprehensive, well-illustrated answer. Let me compile it.
Gastric Volvulus
Gastric volvulus is an abnormal rotation of the stomach more than 180° on its own axis, creating a closed-loop obstruction that can lead to ischemia, necrosis, and death if not corrected urgently. First described by Berti in 1866 (and the first surgical treatment in 1897), it is rare but potentially life-threatening.
Classification
By Axis of Rotation (Singleton Classification)
| Type | Axis | Frequency | Character |
|---|---|---|---|
| Organoaxial (Type I) | Long axis (GEJ to pylorus) | ~59% | Usually acute; strangulation in up to 28% |
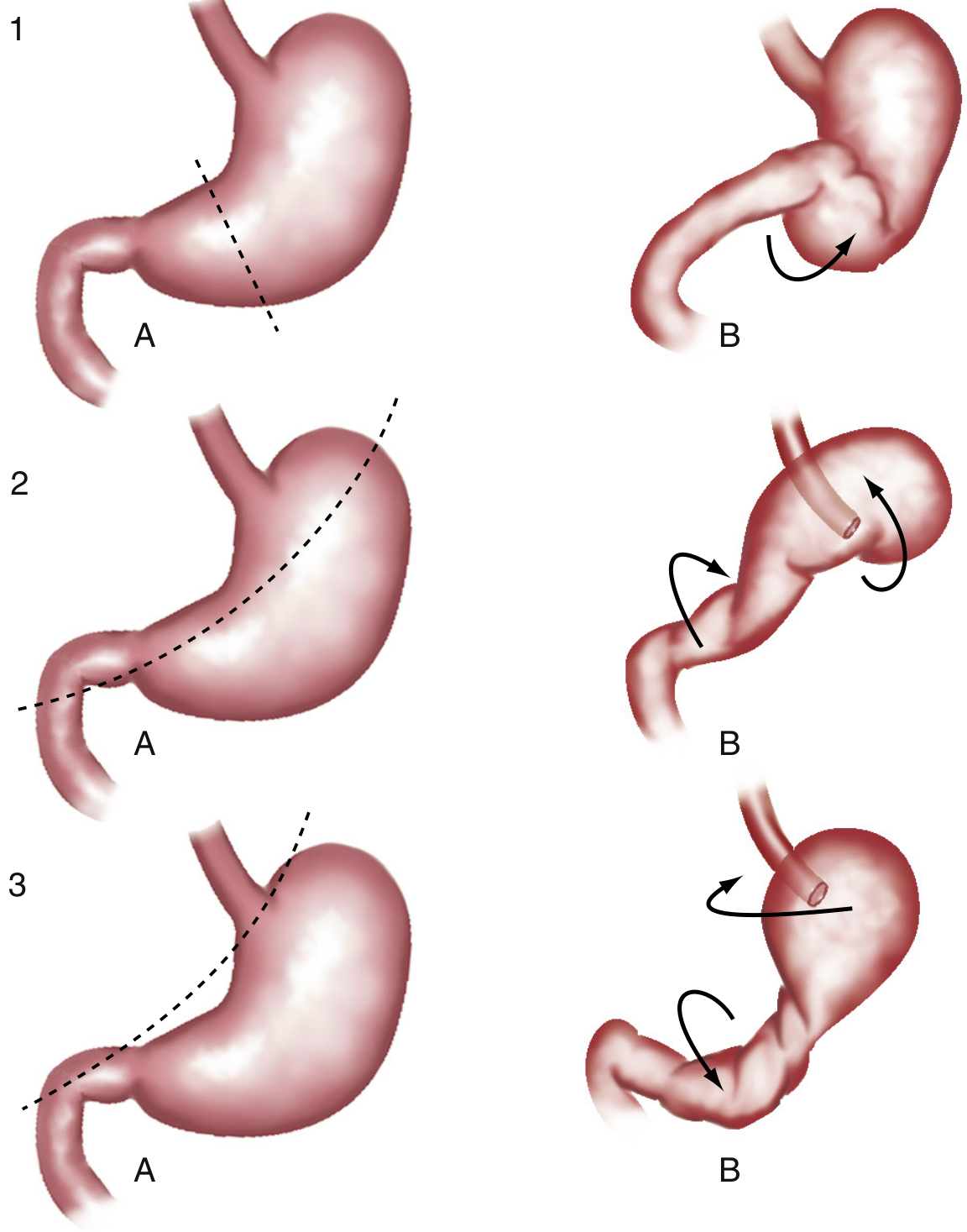
| Mesenteroaxial (Type II) | Short transgastric axis (lesser to greater curvature) | ~29% | Often incomplete and intermittent; infarction uncommon |
| Combined/Unclassified (Type III) | Both axes | ~12% | Usually chronic |
Organoaxial volvulus - the stomach twists along its long axis, with the antrum rotating anteriorly and superiorly, and the fundus posteriorly and inferiorly. It is the most common type and usually an acute event.
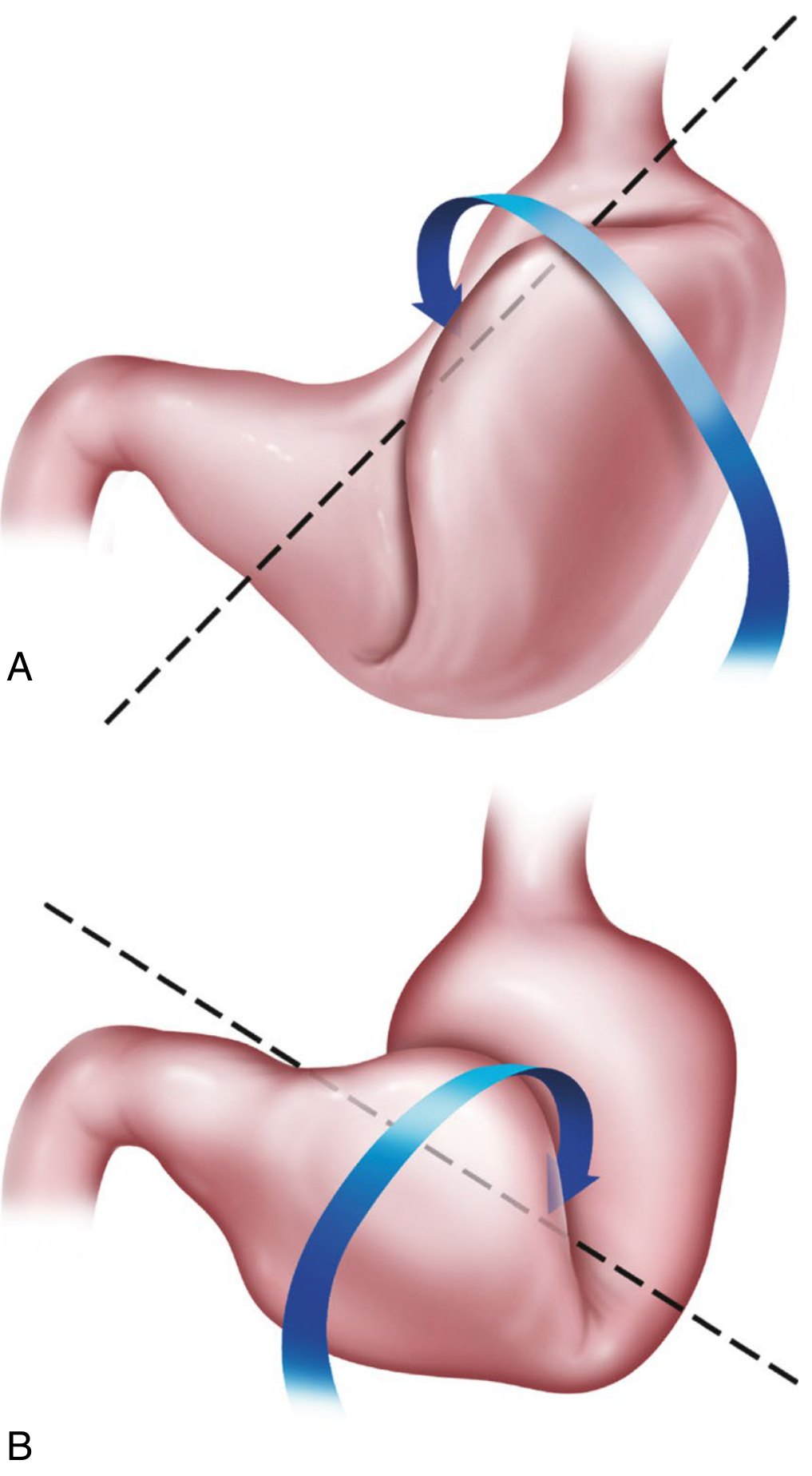
Mesenteroaxial volvulus - the stomach folds on its short axis, folding toward the right of the abdomen, producing an "upside-down stomach." This type is more commonly associated with traumatic diaphragmatic ruptures.
By Etiology
- Primary (subdiaphragmatic) - ~1/3 of cases; caused by laxity or congenital abnormality of stabilizing gastric ligaments (gastrocolic, gastrohepatic, gastrophrenic, gastrosplenic). No extrinsic defect.
- Secondary (supradiaphragmatic) - ~2/3 of cases; associated with a predisposing anatomic defect, most commonly a paraesophageal hernia. Other causes: diaphragmatic eventration or paralysis, phrenic nerve palsy, traumatic diaphragmatic rupture, adhesions, gastric tumor, extrinsic pressure from adjacent organs.
- In children: congenital defects (foramen of Bochdalek, diaphragmatic eventration) are the predominant causes.
By Onset
- Acute - sudden, complete rotation; obstruction and ischemia are immediate risks; surgical emergency.
- Chronic - partial/intermittent rotation; mild, nonspecific recurrent symptoms; often undiagnosed for years.
Epidemiology
- True incidence unknown due to intermittent, self-resolving cases.
- Peak incidence in adults: 5th-6th decade; men and women equally affected.
- ~15-20% of cases occur in children under 1 year, almost always with a congenital diaphragmatic defect.
- Associated with paraesophageal hernia in a large proportion of adult cases.
Pathophysiology
The stomach is normally anchored by:
- Gastrosplenic, gastrohepatic, gastrophrenic, and gastrocolic ligaments
- Retroperitoneal fixation of the duodenum, which provides pexy of the distal stomach
Laxity of these ligaments, loss of retroperitoneal fixation, or tethering of part of the stomach to a fixed point (adhesion, tumor, hernia sac) allows rotation. Rotation >180° causes a closed-loop obstruction at both the GEJ and the pylorus, with progressive venous congestion, ischemia, and eventual full-thickness necrosis if untreated.
Clinical Features
Acute Gastric Volvulus
Borchardt Triad (present in up to 70% of patients):
- Sudden severe epigastric pain and upper abdominal distension
- Violent, unproductive retching (nonproductive vomiting - little to no vomitus)
- Inability to pass a nasogastric tube
Additional features:
- Inability to swallow (dysphagia)
- Nonbilious vomiting before obstruction becomes complete
- Hematemesis (rare - suggests esophageal tear or mucosal ischemia)
- In secondary volvulus with diaphragmatic hernia: predominant chest pain, back/shoulder pain, dyspnea
- In children: up to 25% present with life-threatening events (apnea, cyanosis, acute respiratory distress)
Chronic Gastric Volvulus
- Intermittent mild epigastric discomfort, postprandial bloating
- Dysphagia, early satiety, heartburn, eructation
- Symptoms present for months to years; may go unrecognized
Diagnosis
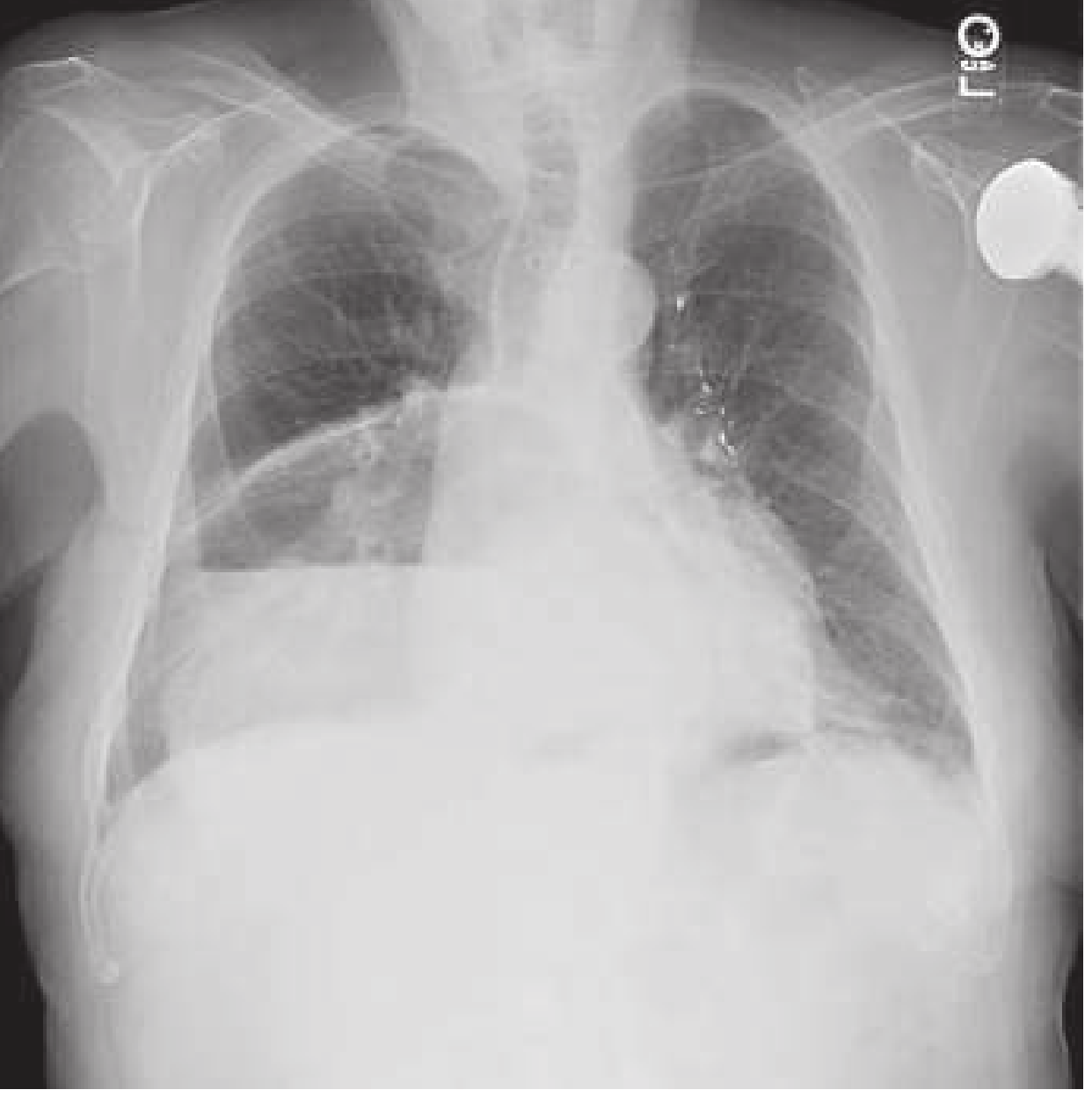
Plain Radiography
- Large gas-filled viscus in the chest or upper abdomen with air-fluid level
- Lack of distal bowel gas (closed-loop obstruction)
- "Upside-down stomach" appearance (greater curvature superior to lesser curvature)
CT Scan (investigation of choice in the ED)
- Dilated stomach in the chest (in secondary volvulus)
- Whirl/swirl sign of the esophagus and stomach at the point of torsion
- Identifies associated anatomical defects (paraesophageal hernia, diaphragmatic defect)
- Signs of gastric necrosis: pneumatosis (gas in stomach wall), free air (perforation)
- Defines vascular compromise
Barium Upper GI Study
- Confirms diagnosis; shows the axis and degree of rotation
- "Upside-down stomach" in organoaxial volvulus (greater curvature above lesser curvature)
- Often unnecessary when CT + classic Borchardt triad are present
Upper Endoscopy
- Twisting of gastric folds at the point of torsion
- Allows assessment of mucosal ischemia
- Can be used for decompression (with care to limit insufflation)
Labs
- No specific lab findings
- Elevated amylase and alkaline phosphatase have been reported
- Leukocytosis, lactic acidosis, metabolic alkalosis (from vomiting)
Complications
- Gastric ischemia and infarction (5-28% for organoaxial type)
- Perforation
- Hemorrhage / hematemesis
- Pancreatic necrosis
- Omental avulsion
- Mortality in untreated acute volvulus: up to 50%
Management
Acute Gastric Volvulus (Surgical Emergency)
Immediate steps:
- IV access, fluid resuscitation, correct electrolyte abnormalities
- Nasogastric (NG) tube decompression - attempt immediately; may occasionally spontaneously reduce the volvulus
- If NG tube placement fails at bedside: endoscopic decompression (limited insufflation, suction distal stomach, assess for ischemia, place NG tube under vision)
- Immediate surgical consultation
Indications for immediate surgery:
- Failure of NG/endoscopic decompression
- Gastric perforation
- Signs of gastric necrosis
- Severe sepsis or refractory hypotension
Surgery:
- Unstable patient: urgent open operation - detorse, assess viability, resect ischemic/necrotic segments; total gastrectomy + jejunostomy + esophagostomy if entire stomach is necrotic (with delayed reconstruction)
- Stable patient: open or laparoscopic repair (laparoscopy now considered gold standard for chronic/stable cases)
- Detorsion of the stomach
- Gastropexy - suture fixation of stomach to anterior abdominal wall or via gastrostomy tube placement
- Repair of the predisposing diaphragmatic hernia (paraesophageal hernia repair ± fundoplication)
- Primary volvulus: gastropexy alone if no hernia present
Chronic Gastric Volvulus
- Same operative principles, but elective timing allows proper preoperative workup
- Laparoscopic repair is preferred
- Associated paraesophageal hernia repaired with diaphragm closure and fundoplication
- Combined endoscopic + laparoscopic repair (e.g., percutaneous endoscopic gastrostomy as a gastropexy technique) has been reported
Prognosis
- Acute gastric volvulus: mortality ~30-50% without prompt treatment; decreases significantly with early surgical intervention
- Chronic volvulus: generally good outcomes with elective repair
- Recurrence is prevented by gastropexy and repair of the underlying predisposing defect
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease, pp. 407-408 | Sabiston Textbook of Surgery, pp. 1792-1793 | Rosen's Emergency Medicine, pp. 1231-1232 | Yamada's Textbook of Gastroenterology, 7th ed., pp. 1127-1128 | Grainger & Allison's Diagnostic Radiology, p. 513
This is a shared conversation. Sign in to Orris to start your own chat.