Explain The menstrual cycle with applied pathology in detaill..with proper mneomonics...i want to learn and make a grip on this for reaching to a perfect diagnosis and clinically sound
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive textbook data to build a thorough, mnemonic-rich masterclass. Let me compose the complete answer.
The Menstrual Cycle - Complete Masterclass with Applied Pathology & Mnemonics
Sources: Costanzo Physiology 7e, Berek & Novak's Gynecology, Robbins & Kumar Basic Pathology, Robbins Cotran & Kumar Pathologic Basis of Disease, Rosen's Emergency Medicine
PART 1 - THE AXIS (The Master Control System)
The menstrual cycle is governed by a 4-level axis. Think of it as a military chain of command:
HYPOTHALAMUS → PITUITARY → OVARY → UTERUS
(General) (Colonel) (Major) (Battlefield)
Mnemonic: "H-P-O-U" = "He Punished Over-Users"
Hypothalamus - GnRH
- GnRH = Gonadotropin-Releasing Hormone (a decapeptide)
- Produced in the arcuate nucleus - embryologically migrates from the olfactory pit
- Must be secreted in a pulsatile fashion to work (continuous infusion = downregulation = no effect)
- Half-life only 2-4 minutes due to rapid proteolytic cleavage
- Pulse frequency differs by phase:
- Follicular phase: frequent, small-amplitude pulses
- Late follicular: increased frequency + amplitude (LH surge priming)
- Luteal phase: progressive lengthening of intervals, high amplitude
Clinical pearl: Slow GnRH pulses → favor FSH; Fast pulses → favor LH. This is exploited pharmacologically - GnRH agonists given continuously (e.g., leuprolide) SUPPRESS LH/FSH, used in endometriosis, precocious puberty, and IVF downregulation.
Mnemonic for GnRH rules: "POND"
- Pulsatile = necessary
- Oncontinuous = suppresses (downregulation)
- Nucleus arcuate = origin
- Decapeptide = structure
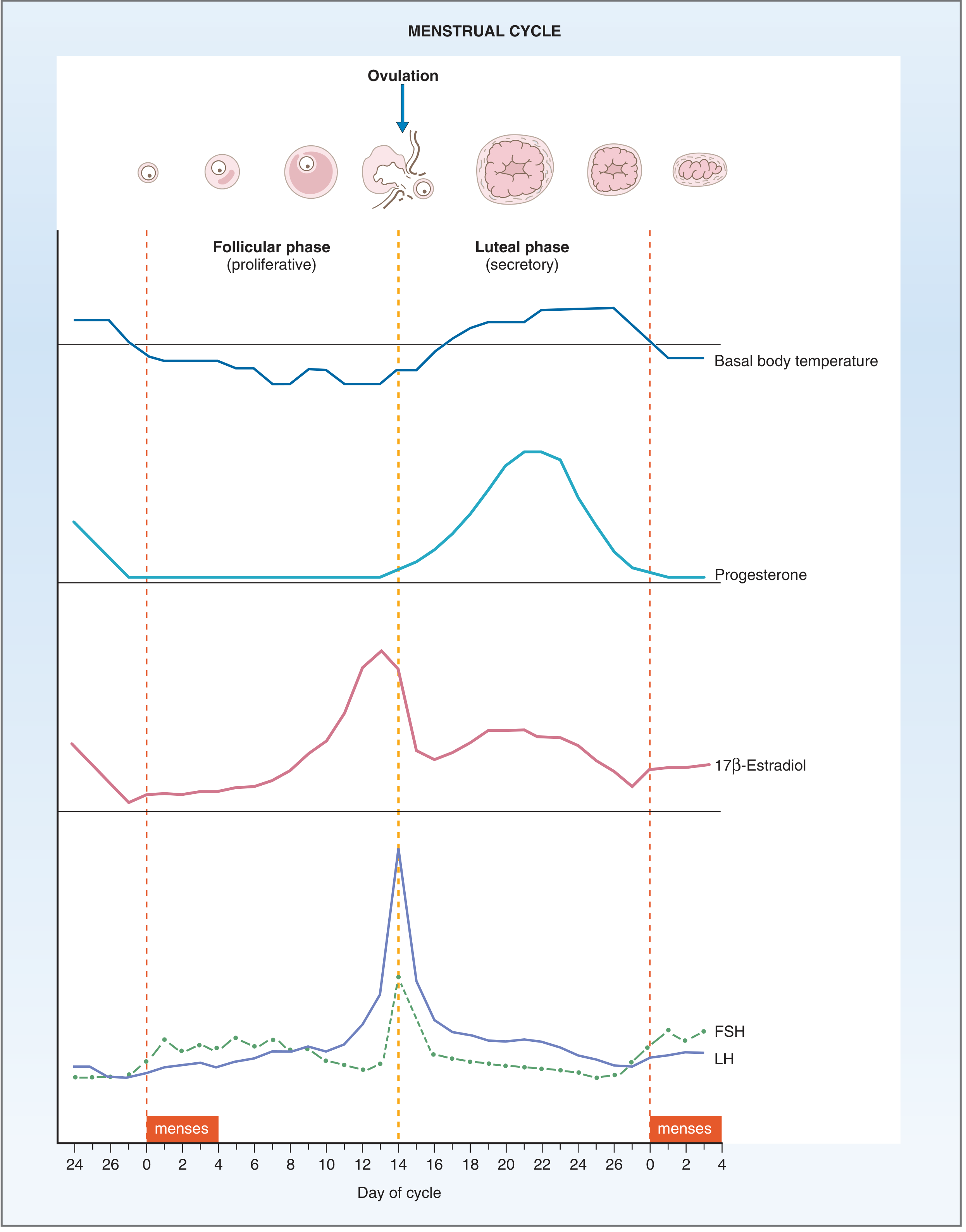
PART 2 - THE THREE PHASES (Overview)
Mnemonic: "FOM" or "Fluffy Old Madam"
| Phase | Days (28-day cycle) | Dominant hormone | Endometrium |
|---|---|---|---|
| Follicular (Proliferative) | Days 1-14 | Estrogen (17β-estradiol) | Proliferates |
| Ovulation | Day 14 | LH surge | - |
| Luteal (Secretory) | Days 14-28 | Progesterone | Secretory |
Key rule to memorize: Only the follicular phase length varies (14-21+ days). The luteal phase is always fixed at 14 days. So ovulation in a 35-day cycle is on day 21, not day 14.
PART 3 - FOLLICULAR PHASE (Days 1-14) - "ESTROGEN RULES"
What drives it?
- As the corpus luteum of the previous cycle degenerates → progesterone + inhibin A fall → FSH rises (freed from negative feedback)
- Rising FSH recruits a cohort of antral follicles
Folliculogenesis - "PPST" (Four Follicle Types)
Mnemonic: "Pretty Princesses Sometimes Transform"
- Primordial - arrested oocyte + flat granulosa cells (0.03-0.05 mm)
- Primary - cuboidal granulosa, zona pellucida forms (0.1 mm) - first FSH receptors appear
- Secondary - multi-layered granulosa, theca cells differentiate with LH receptors, neoangiogenesis (0.2 mm)
- Tertiary (antral) → Graafian (dominant) - fluid-filled antrum, most FSH receptors
The Two-Cell, Two-Gonadotropin Theory
Mnemonic: "TACT" - Theca And Cortext Together
LH → THECA CELLS → Androgens (androstenedione, testosterone)
↓ (diffuse into granulosa)
FSH → GRANULOSA CELLS → Aromatase → Estrogens (estradiol)
- Theca produces androgens under LH; Granulosa converts them to estrogen under FSH
- Dominant follicle wins by having the most FSH receptors → produces more estrogen → survives even as FSH drops
Endometrial Changes (Proliferative)
- Estradiol → endometrial growth, gland elongation, spiral arteries elongate
- Cervical mucus: copious, watery, elastic, "ferning" pattern on glass slide (channels form that allow sperm penetration)
Mnemonic for Estrogen's Uterine Effects: "GCSE"
- Growth of endometrium
- Cervical mucus watery (ferning, sperm-friendly)
- Spiral arteries elongate
- Endometrial glands elongate
PART 4 - OVULATION (Day 14)
Trigger Sequence:
- Dominant follicle's rising estradiol reaches a threshold (~200 pg/mL for >36 hrs)
- Positive feedback switch: estrogen now stimulates GnRH → FSH + LH surge
- LH surge → ovulation within 36-40 hours
- LH disrupts gap junctions between granulosa cells and oocyte → meiosis I resumes (was arrested in dictyate/diplotene stage of prophase I since fetal life)
- Egg released as secondary oocyte (meiosis II completes only if fertilized)
Mnemonic: "PLOT"
- Positive feedback from estradiol peak
- LH surge triggers ovulation
- Oocyte resumes meiosis (exits prophase I arrest)
- Temperature (basal body temperature rises 0.5°C after ovulation due to progesterone - thermogenic)
Signs of Ovulation (Clinically Useful)
- Mittelschmerz - mid-cycle pelvic pain (follicle rupture)
- Basal body temperature RISES (progesterone is thermogenic)
- Cervical mucus becomes watery and shows "ferning" (pre-ovulation estrogen peak)
- LH urine surge detectable 24h before ovulation (basis of OPKs)
PART 5 - LUTEAL/SECRETORY PHASE (Days 14-28)
Corpus Luteum Formation
- Granulosa and theca cells luteinize under LH → corpus luteum
- Produces: Progesterone (dominant) + Estradiol + Inhibin A
- Corpus luteum survives 12-16 days if no pregnancy; then → corpus albicans (fibrous scar)
Progesterone's Actions (Secretory Phase):
Mnemonic: "STAB-C"
- Secretory transformation of endometrium (glands tortuous, glycogen vacuoles, increased mucus)
- Temperature rises (hypothalamic set point elevated - thermogenic)
- Arteries become coiled (spiral arteries hypertrophy)
- Blocking cervical mucus (thick, non-elastic, non-ferning - now sperm-hostile)
- Contractility of uterus decreases (maintains implantation environment)
What happens if NO pregnancy:
- Corpus luteum regresses → progesterone + estradiol fall → endometrial ischemia → menstruation
- Mechanism: spiral artery vasoconstriction (mediated by prostaglandins) → ischemia → necrosis → sloughing = menses
What happens if PREGNANCY occurs:
- Implanting trophoblast secretes hCG (mimics LH) → rescues corpus luteum
- Corpus luteum maintains progesterone until luteal-placental shift (~5-7 weeks gestation)
PART 6 - FEEDBACK LOOPS (MUST KNOW)
Mnemonic: "PENS-N" (Positive/Negative depending on level)
| Estrogen level | Feedback effect | Result |
|---|---|---|
| Low (early follicular) | Negative | FSH/LH suppressed moderately |
| Rising/sustained high (late follicular, >200 pg/mL >36h) | POSITIVE | LH SURGE → ovulation |
| Luteal (with progesterone) | Negative | FSH/LH both suppressed |
This is unique - estrogen can do BOTH positive and negative feedback depending on level and duration. That's why combined OCP (high constant estrogen + progestin) = sustained negative feedback = no LH surge = no ovulation.
PART 7 - APPLIED PATHOLOGY (The Clinical Payoff)
FRAMEWORK: PALM-COEIN Classification for Abnormal Uterine Bleeding (AUB)
This is the current standard (FIGO 2011) - replaces the obsolete term "dysfunctional uterine bleeding (DUB)."
Mnemonic: "PALM COEIN" - Think of a palm tree in a coin!
PALM = Structural causes COEIN = Non-structural causes
P - Polyp C - Coagulopathy
A - Adenomyosis O - Ovulatory dysfunction
L - Leiomyoma (SM vs Other) E - Endometrial
M - Malignancy/Hyperplasia I - Iatrogenic
N - Not yet classified
STRUCTURAL CAUSES (PALM)
P - Polyps
- Focal endometrial/cervical overgrowths
- Cause: intermenstrual spotting, menorrhagia
- Diagnosis: sonohysterography, hysteroscopy
- Associated with: unopposed estrogen, tamoxifen use
A - Adenomyosis
- Endometrial glands/stroma within myometrium (not outside uterus - that's endometriosis)
- Causes: dysmenorrhea + menorrhagia + globular "boggy" uterus
- Mnemonic: "Adenomyosis = Endo IN the muscle" (vs Endometriosis = Endo OUTSIDE)
- Diagnosis: MRI (gold standard), USS (junctional zone >12mm)
L - Leiomyoma (Fibroids)
- Submucosal > intramural > subserosal for causing bleeding
- Submucosal fibroids distort the cavity → most symptomatic bleeding
- Estrogen-dependent (grow in reproductive years, regress post-menopause)
M - Malignancy/Hyperplasia
- Most common cancer of female genital tract in high-income countries = endometrial carcinoma
- Two pathways:
Mnemonic: "Type 1 vs Type 2 = Young vs Old"
| Feature | Type 1 (Endometrioid) | Type 2 (Serous) |
|---|---|---|
| Background | Estrogen excess, hyperplasia | Endometrial atrophy |
| Age | Perimenopausal | Older postmenopausal |
| Gene mutation | PTEN (most common) | TP53 |
| Behavior | Indolent, good prognosis | Aggressive, poor prognosis |
| Percentage | ~80% of cases | ~10-15% |
Risk factors for Type 1 (Endometrioid): "OPEN-DOES"
- Obesity (adipose tissue converts androgens → estrogens via aromatase)
- PCOS
- Early menarche/late menopause
- Nulliparity
- Diabetes/metabolic syndrome
- Ovarian tumors (granulosa-theca cell - estrogen-producing)
- Exogenous estrogen (unopposed)
- Sterility
Endometrial Hyperplasia:
- Without atypia: 1-3% risk of progression to carcinoma
- With atypia (EIN - Endometrial Intraepithelial Neoplasia): HIGH risk, carries PTEN mutations - same as carcinoma
- Treatment: atypia → hysterectomy (or progestins if fertility desired)
NON-STRUCTURAL CAUSES (COEIN)
C - Coagulopathy
- Up to 20% of women with heavy menstrual bleeding have an underlying coagulopathy
- Von Willebrand disease = most common (up to 13% of AUB cases)
- Often presents at menarche with first heavy period
- Screen: family history of bleeding disorders, easy bruising, gum bleeding
O - Ovulatory Dysfunction
This is the MOST IMPORTANT non-structural category. Anovulation leads to unopposed estrogen → irregular, heavy, unpredictable bleeding.
Causes of Anovulation: "HEAP"
- Hyperprolactinemia (prolactin suppresses GnRH → low LH/FSH)
- Endocrine (thyroid disease, adrenal disorders)
- Androgenic excess / Anorexia nervosa / any systemic illness
- PCOS (most common in reproductive age)
Most common by age group:
| Age | Most Common Cause |
|---|---|
| Prepuberty | Precocious puberty |
| Adolescence | Anovulatory cycles (HPO axis immature) + coagulation disorders |
| Reproductive age | PCOS, pregnancy complications, fibroids, polyps |
| Perimenopause | Anovulatory cycles (HPO axis waning) |
| Postmenopause | Endometrial carcinoma/atrophy |
PCOS (Polycystic Ovary Syndrome)
The most common endocrine disorder in women of reproductive age.
Diagnostic criteria (Rotterdam - 2 of 3):
Mnemonic: "HAO"
- Hyperandrogenism (clinical: hirsutism, acne; or biochemical: elevated androgens)
- Anovulation (oligomenorrhea/amenorrhea)
- Ovary appearance (polycystic on USS: >12 follicles 2-9mm OR volume >10 mL)
Pathophysiology Loop:
↑LH:FSH ratio
→ ↑Theca androgen production
→ Partial aromatization → ↑Estrone (constant, not cyclic)
→ Positive feedback on LH, negative on FSH
→ More androgen, less FSH → follicle arrest → anovulation
Associations: insulin resistance, metabolic syndrome, type 2 diabetes, obesity
E - Endometrial (Primary endometrial dysfunction)
- Defects in local endometrial hemostatic mechanisms
- Normal ovulatory cycles but abnormal bleeding
- Mechanism: impaired prostaglandin balance, deficient tissue factor expression
I - Iatrogenic
- Hormonal contraceptives (breakthrough bleeding, especially progestin-only)
- IUDs (copper → heavy bleeding; levonorgestrel IUD → amenorrhea)
- Anticoagulants
- Post-cesarean scar defect (isthmocele)
PART 8 - ENDOMETRIOSIS (Special Topic)
Definition: Presence of endometrial glands AND/OR stroma outside the uterus
Sites (in order of frequency) - Mnemonic: "O-UL-RC-SML-C-V-L":
Think "Our Unique Lab Rarely Creates Some Meaningless Confusing Variables Lately"
- Ovaries (most common - "chocolate cysts")
- Uterine ligaments
- Ligament (rectovaginal septum)
- Rectovaginal septum
- Cul de sac
- Serosa of bowel/appendix
- Mucosa of cervix/vagina
- Laparotomy scars
Classic Triad: "DIP"
- Dysmenorrhea (painful periods - cyclical pelvic pain)
- Infertility
- Pelvic pain (chronic)
Pathogenesis Theories - Mnemonic: "REMS":
- Regurgitation (Sampson's theory) - retrograde menstruation → implantation
- Embolism (benign metastasis) - lymphatic/vascular spread
- Metaplasia - coelomic epithelium → endometrium
- Stem cells - bone marrow-derived progenitors
Chocolate cyst = endometrioma of ovary (degenerated blood = "chocolate" = old hemosiderin)
PART 9 - TERMINOLOGY QUICK REFERENCE (For Diagnosis)
Mnemonic: "MOMS HELP OLDER PATIENTS"
| Term | Definition |
|---|---|
| Menorrhagia | Heavy regular periods (>80mL/cycle or >7 days) |
| Metrorrhagia | Irregular intermenstrual bleeding |
| Menometrorrhagia | Heavy AND irregular bleeding |
| Oligomenorrhea | Cycles >35 days |
| Polymenorrhea | Cycles <21 days |
| Amenorrhea (primary) | No periods by age 16 (with secondary characteristics) |
| Amenorrhea (secondary) | Cessation of periods for >3 months in previously menstruating woman |
| Dysmenorrhea | Painful periods |
| Hypomenorrhea | Very light periods |
Primary amenorrhea causes - Mnemonic: "TOGA"
- Turner syndrome (45,X) - commonest chromosomal cause
- Outflow tract obstruction (imperforate hymen, vaginal atresia)
- Gonadal dysgenesis (other)
- Androgen insensitivity syndrome (46,XY - complete AIS)
Secondary amenorrhea - "PHAT P" (most to less common)
- Pregnancy (ALWAYS rule out first!)
- Hypothalamic dysfunction (stress, weight loss, exercise - "functional hypothalamic amenorrhea")
- Anterior pituitary (hyperprolactinemia, Sheehan's syndrome, tumors)
- Thyroid / adrenal disease
- PCOS / premature ovarian insufficiency
PART 10 - CLINICAL DIAGNOSTIC APPROACH TO AUB
Step-by-step: "RIPE" Framework
R - Rule out pregnancy first (urine hCG in ALL women of reproductive age)
I - Investigate based on age:
- Adolescent: coagulation screen (VWD), hormonal workup
- Reproductive: USS (fibroids, polyps), hormonal panel (FSH, LH, TSH, prolactin, androgens)
- Perimenopausal: endometrial biopsy if >45 years or risk factors
- Postmenopausal: endometrial biopsy + USS (endometrial thickness >4mm = investigate)
P - PALM-COEIN classify
E - Examine + Endometrial biopsy if indicated
MASTER SUMMARY TABLE
| Phase | Days | Key Hormone | Endometrium | Cervix | Clinical Relevance |
|---|---|---|---|---|---|
| Menstruation | 1-5 | Falling E + P | Sloughing | - | Dysmenorrhea, endometriosis pain peaks |
| Proliferative | 5-14 | Estrogen | Proliferates (glands elongate) | Watery, ferning | Estrogen excess → hyperplasia |
| Ovulation | ~14 | LH surge | - | Most watery/open | Mittelschmerz; OPK window |
| Secretory | 14-28 | Progesterone | Secretory (tortuous glands, glycogen) | Thick, non-ferning | Progesterone deficiency → PMS, luteal phase defect |
| Pre-menstrual | 26-28 | Both falling | Ischemia begins | - | PMS/PMDD; if no pregnancy → menses |
FINAL MNEMONICS CHEAT SHEET
| Topic | Mnemonic |
|---|---|
| The axis | H-P-O-U (Hypothalamus → Pituitary → Ovary → Uterus) |
| Phases | FOM (Follicular, Ovulation, Menstrual) |
| GnRH rules | POND (Pulsatile, cOntinuous suppresses, Nucleus arcuate, Decapeptide) |
| Estrogen effects | GCSE (Growth, Cervix watery, Spirals elongate, Endometrial glands grow) |
| Progesterone effects | STAB-C (Secretory, Temperature, Arteries coiled, Blocks cervix, Contractility↓) |
| Ovulation trigger | PLOT (Positive feedback, LH surge, Oocyte meiosis, Temperature rise) |
| AUB classification | PALM-COEIN |
| Endometriosis triad | DIP (Dysmenorrhea, Infertility, Pelvic pain) |
| Anovulation causes | HEAP (Hyperprolactinemia, Endocrine, Androgens/Anorexia, PCOS) |
| PCOS diagnosis | HAO (Hyperandrogenism, Anovulation, Ovaries polycystic) |
| Secondary amenorrhea | PHAT P (Pregnancy, Hypothalamic, Anterior pit, Thyroid, PCOS/POI) |
| AUB diagnostic approach | RIPE (Rule out pregnancy, Investigate by age, Palm-coein, Examine) |
References: Costanzo Physiology 7e (pp. 479-480); Berek & Novak's Gynecology (pp. 264-294); Robbins & Kumar Basic Pathology (Table 17.2, Sections on AUB, Endometrial Hyperplasia, Carcinoma); Robbins Cotran & Kumar Pathologic Basis of Disease (pp. 929-932); Rosen's Emergency Medicine - PALM-COEIN classification
1 and 3
Asking for Preferences
Most likely you're referring to Parts 1 and 3 from the previous answer - The Axis and The Follicular Phase. Let me go deeper on both with more detail, clinical correlations, and additional mnemonics.
PART 1 - THE H-P-O-U AXIS (Deep Dive)
The 4-Level Hierarchy
HYPOTHALAMUS
↓ GnRH (portal blood)
PITUITARY
↓ FSH + LH (systemic blood)
OVARY
↓ Estrogen + Progesterone + Inhibin
UTERUS (end organ)
Every clinical disorder of the menstrual cycle can be traced to a failure at one of these 4 levels. That is why knowing the axis = knowing the diagnosis.
Level 1 - Hypothalamus
GnRH - The Master Switch
- Full name: Gonadotropin-Releasing Hormone (also called LHRH)
- Structure: Decapeptide (10 amino acids)
- Origin: Arcuate nucleus of the hypothalamus
- Embryology: GnRH neurons originate in the olfactory pit and migrate to the arcuate nucleus during fetal life
Clinical pearl - Kallmann Syndrome: Failure of GnRH neurons to migrate from olfactory pit → hypogonadotropic hypogonadism + anosmia. Patient has no periods AND cannot smell. The link between smell and reproduction is because of this shared embryological origin.
The Pulsatile Imperative
This is the single most testable fact about GnRH:
Mnemonic: "Pulse or Nothing"
| GnRH pattern | Effect on pituitary | Clinical application |
|---|---|---|
| Pulsatile | Upregulates receptors → FSH + LH secreted normally | Normal physiology; pulsatile GnRH used to TREAT Kallmann's |
| Continuous | Downregulates receptors → FSH + LH suppressed | GnRH agonists (leuprolide, goserelin) used to SUPPRESS in endometriosis, prostate cancer, precocious puberty, IVF downregulation |
Mnemonic: "PULSE = PRODUCE; CONTINUOUS = CASTRATE"
GnRH Pulse Frequency Across the Cycle
| Phase | Pulse frequency | FSH:LH ratio effect |
|---|---|---|
| Early follicular | Moderate frequency, small amplitude | Favors FSH (recruits follicles) |
| Late follicular | High frequency + amplitude | Favors LH (primes for surge) |
| Luteal | Slow frequency, high amplitude | FSH rises again (preparing next cycle) |
Slow pulses → favor FSH; Fast pulses → favor LH This is why in the late luteal phase (slow pulses), FSH quietly rises to begin recruiting the next cohort of follicles even BEFORE the current period begins.
What modulates GnRH?
Mnemonic: "KISSPEPTIN is the BOSS of GnRH"
- Kisspeptin (from KNDy neurons in arcuate nucleus) is the primary stimulator of GnRH release
- Kisspeptin neurons also respond to estrogen feedback - this is HOW estrogen both suppresses AND surges GnRH depending on level
- Neurokinin B (stimulates kisspeptin) and Dynorphin (inhibits kisspeptin) also modulate the system
Inhibitors of GnRH (and thus the whole axis):
- Stress → CRH → cortisol → suppresses GnRH (explains amenorrhea in athletes/anorexics)
- Prolactin excess → suppresses GnRH (explains amenorrhea with hyperprolactinemia, and lactational amenorrhea)
- Opioids (endogenous and exogenous) → suppress GnRH pulses
- High estrogen + progesterone (combined OCP) → negative feedback
Level 2 - Anterior Pituitary
FSH and LH - Structure & Differences
Both are glycoprotein heterodimers with:
- Identical α-subunit (shared with TSH and hCG - this is why hCG can mimic LH!)
- Unique β-subunit (determines specificity)
Mnemonic: "Same Alpha, Different Beta" = SADB
| Hormone | Primary target cell | Primary action |
|---|---|---|
| FSH | Granulosa cells | Follicle growth; aromatase induction |
| LH | Theca cells | Androgen production; ovulation trigger; corpus luteum support |
The LH Surge - Mechanism
Triggered when estradiol sustains >200 pg/mL for >36 hours → switches from negative to positive feedback:
Estradiol peak
↓
GnRH pulse amplitude ↑ (positive feedback via kisspeptin)
↓
Massive LH release (10-fold rise within 36-48h)
↓
Ovulation ~36-40 hours later
Why does estrogen switch from negative to positive feedback?
- At low levels: estrogen inhibits kisspeptin → suppresses GnRH
- At high, sustained levels: estrogen upregulates kisspeptin receptors in the hypothalamus AND directly upregulates LH receptors in pituitary gonadotrophs → positive feedback kicks in
Level 3 - Ovary
Inhibins - The Fine-Tuners
Often forgotten but clinically important:
| Inhibin | Source | Regulates | Clinical use |
|---|---|---|---|
| Inhibin B | Granulosa cells (early follicular) | Suppresses FSH specifically | Low in diminished ovarian reserve |
| Inhibin A | Corpus luteum (luteal phase) | Suppresses FSH in luteal phase | Elevated in Down syndrome (maternal serum screening) |
Mnemonic: "B for Beginning (follicular), A for After (luteal)"
Ovarian Disorders at the Axis Level
| Disorder | Level | Hormonal pattern |
|---|---|---|
| Hypothalamic amenorrhea (stress, anorexia) | Hypothalamus | Low GnRH → Low FSH, Low LH, Low E2 |
| Hyperprolactinemia | Hypothalamus/Pituitary | High PRL → Low GnRH → Low FSH, LH |
| Kallmann syndrome | Hypothalamus | Low GnRH → Low FSH, LH, E2; no smell |
| Pituitary tumor/Sheehan's | Pituitary | Low FSH, Low LH, Low E2 |
| PCOS | Ovary/Hypothalamus | High LH, normal/low FSH (LH:FSH >2:1), High androgens |
| Premature Ovarian Insufficiency (POI) | Ovary | High FSH, High LH (no negative feedback from failed ovary) |
| Menopause | Ovary | High FSH, High LH (FSH >40 IU/L diagnostic) |
The most important diagnostic principle: FSH level tells you WHERE the problem is:
- FSH low = problem is above the ovary (hypothalamus or pituitary) = hypogonadotropic hypogonadism
- FSH high = problem is at the ovary level (ovarian failure) = hypergonadotropic hypogonadism
Mnemonic: "LOW FSH = LOW DOWN problem (brain); HIGH FSH = HIGH UP (ovary screaming for help)"
Level 4 - Uterus (End Organ)
The uterus can fail independently even with a normal axis. This is called outflow tract pathology.
Asherman's Syndrome = intrauterine adhesions (synechiae) from uterine curettage, infection
- Normal FSH, LH, estrogen - axis is fine
- But endometrium is scarred and cannot respond
- Presents as secondary amenorrhea after D&C or postpartum hemorrhage
- Diagnosis: hysteroscopy (gold standard)
- Treatment: hysteroscopic adhesiolysis + estrogen therapy to re-grow endometrium
PART 3 - FOLLICULAR PHASE (Deep Dive)
Timeline: What Happens Day by Day
Days 1-5 (Menstruation + Early Recruitment)
- Corpus luteum of previous cycle → dead → progesterone + inhibin A fall
- FSH escapes suppression and rises - this rise happens even BEFORE the period ends
- FSH recruits a cohort of antral follicles (5-10 follicles awakened from their resting state)
- Each recruited follicle is a "tertiary/antral" follicle (already developed over the previous 3 months in a gonadotropin-independent phase)
Important: Folliculogenesis from primordial to antral takes about 85 days total. The "follicular phase" we see clinically is only the final 14-day FSH-dependent selection period.
Days 5-9 (Follicular Selection)
- All recruited follicles grow under FSH stimulation
- Each produces increasing estradiol
- Rising estradiol → negative feedback → FSH starts falling again
- Only the follicle with the most FSH receptors and best local estrogen environment survives the FSH decline = DOMINANT FOLLICLE
- All others undergo atresia (apoptosis of granulosa cells)
Mnemonic: "Survival of the Most Sensitive" - the dominant follicle is not the biggest, it's the most receptor-rich
Days 9-14 (Dominant Follicle Growth)
- Dominant (Graafian) follicle continues to grow (up to 20-25mm)
- Produces surging estradiol
- LH receptors appear on granulosa cells (FSH-induced) → granulosa cells can now respond directly to the LH surge
Folliculogenesis - 5 Stages in Detail
Full mnemonic: "People Prefer Sleeping Through All Grading"
(Primordial → Primary → Secondary → Tertiary/Antral → Graafian/Dominant)
1. Primordial Follicle
- Size: 0.03-0.05mm
- Structure: primary oocyte (arrested in prophase I of meiosis I, diplotene/dictyate stage) + single layer of flattened granulosa cells + basal lamina
- Status: dormant, no FSH receptors, no blood supply
- Numbers: ~1-2 million at birth → ~300,000-400,000 at puberty → ~1,000 at menopause
- Meiotic arrest maintained by: oocyte maturation inhibitor (OMI) from granulosa, granulosa-derived cAMP transmitted via gap junctions (connexins)
2. Primary Follicle
- Granulosa cells become cuboidal (first sign of activation/recruitment)
- Zona pellucida begins to form (extracellular glycoprotein matrix between oocyte and granulosa)
- Gap junctions (connexins) connect oocyte and granulosa
- FSH receptors appear on granulosa - but no effect yet (no vasculature)
3. Secondary Follicle
- Multiple layers of cuboidal granulosa cells
- Theca cells differentiate from stromal cells → express LH receptors
- Neoangiogenesis occurs in theca layer → follicle now exposed to circulating FSH and LH
- Two-cell two-gonadotropin system now operational
4. Tertiary (Antral) Follicle
- Antrum forms - fluid-filled space (follicular fluid = plasma filtrate + granulosa secretions, rich in estrogen)
- Cumulus oophorus - granulosa cells surrounding oocyte (projecting into antrum)
- Mural granulosa cells - line the follicle wall
- Fully FSH-dependent from this point
5. Graafian (Dominant) Follicle
- Size: 20-25mm pre-ovulation
- Massive estradiol production
- LH receptors appear on granulosa cells (FSH-induced) → ready for LH surge
- Oocyte is still arrested in prophase I until the LH surge disrupts gap junctions
The Two-Cell, Two-Gonadotropin Theory - In Detail
This is a CORE concept tested everywhere.
+-----------------------------+ +--------------------------------+
| THECA CELL | | GRANULOSA CELL |
| (has LH receptors) | | (has FSH receptors) |
| | | |
| Cholesterol | | |
| ↓ (LH) | | |
| Pregnenolone | | Receives androstenedione |
| ↓ | →→→| ↓ (FSH → aromatase) |
| Progesterone | | ESTRADIOL (E2) |
| ↓ | | |
| Androstenedione | | |
| Testosterone | | |
+-----------------------------+ +--------------------------------+
Key points:
- Theca cells CANNOT aromatize (no aromatase) → they can only make androgens
- Granulosa cells CANNOT make androgens (no 17α-hydroxylase) → they need theca's androgens as substrate
- Both cell types are needed - neither can produce estrogen alone
Clinical application:
- FSH deficiency → no aromatase induction → no estrogen despite LH being normal
- LH deficiency → no androgens → no substrate for aromatase → no estrogen
- Granulosa cell tumors → make estrogen directly → hyperestrogenism → precocious puberty in girls, endometrial hyperplasia in women
Estradiol's Actions in the Follicular Phase - Expanded
On the Endometrium (Proliferative Phase)
- Stimulates endometrial gland elongation
- Promotes stromal growth
- Elongates spiral arteries
- Increases endometrial thickness (from ~1mm at menses to ~8-12mm at ovulation)
- Induces progesterone receptors on endometrium (preparing it to respond to luteal progesterone)
On the Cervix
- Mucus becomes: copious, watery, clear, elastic
- Ferning pattern on glass slide (NaCl crystallization in estrogen-rich mucus)
- Spinnbarkeit = stretchability of cervical mucus (up to 6-8cm at ovulation)
- Cervical os opens slightly
Mnemonic: "EWCM" = Egg White Cervical Mucus (what fertile-quality mucus looks and feels like)
On Pituitary/Hypothalamus
- Low levels → negative feedback (suppresses FSH/LH)
- High sustained levels → positive feedback (triggers LH surge)
On Other Systems
- Increases hepatic production of SHBG (sex hormone binding globulin) → binds androgens → reduces free testosterone (explains why combined OCP reduces hirsutism in PCOS)
- Promotes bone density (osteoblast stimulation, osteoclast inhibition)
- Cardiovascular protection (vasodilation, favorable lipid profile)
- Increases coagulation factors (V, VII, VIII, X, fibrinogen) → explains VTE risk with OCPs
Why the Follicular Phase Length Varies (Clinical Importance)
The follicular phase can be 7 to 21+ days depending on:
- How quickly a dominant follicle develops
- FSH levels (higher FSH = faster recruitment)
- Ovarian reserve (fewer follicles = slower recruitment = longer follicular phase in perimenopause)
- Stress, illness, medications (can delay or prevent ovulation)
The luteal phase, however, is ALWAYS ~14 days (because corpus luteum lifespan is fixed at 12-16 days regardless of anything, unless rescued by hCG).
Clinical use: If a woman has a 35-day cycle, she ovulates on day ~21. If you want to do a progesterone test to confirm ovulation, draw it on day 28 (7 days after presumed ovulation, i.e., luteal mid-point). A level >3 ng/mL confirms ovulation; >10 ng/mL = adequate luteal function.
Follicular Phase Pathology Summary
| Pathology | Mechanism | Presentation |
|---|---|---|
| PCOS | ↑LH:FSH, ↑androgens → follicle arrest at antral stage (8-10mm), no dominant follicle selected | Oligomenorrhea/amenorrhea, multiple small follicles on USS, hirsutism, acne |
| Premature Ovarian Insufficiency | Follicle pool depleted or unresponsive | Amenorrhea in <40 yrs, high FSH (>25-40 IU/L), hot flashes, low E2 |
| Hypothalamic amenorrhea | Low GnRH → low FSH → follicles not recruited | Amenorrhea, low FSH, low E2, low BMI or high stress history |
| Luteal phase defect | Inadequate follicular development → poor corpus luteum → low progesterone | Short cycles, infertility, recurrent early miscarriage |
| Granulosa cell tumor | Autonomous estrogen production bypassing the axis | Precocious puberty (child), menorrhagia (adult), endometrial hyperplasia; inhibin B elevated (tumor marker) |
Final Mnemonic Summary for Parts 1 & 3
| Concept | Mnemonic |
|---|---|
| Axis levels | H-P-O-U |
| GnRH rule | "Pulse or Nothing" (pulsatile = produce; continuous = castrate) |
| FSH level interpretation | "LOW FSH = LOW DOWN (brain); HIGH FSH = HIGH UP (failing ovary)" |
| Inhibins | "B for Beginning (follicular), A for After (luteal)" |
| GnRH modifiers | KISS the GnRH (Kisspeptin is the boss) |
| Follicle stages | "People Prefer Sleeping Through All Grading" (Primordial, Primary, Secondary, Tertiary, Antral, Graafian) |
| Two-cell theory | "Theca = Androgen factory (LH-driven); Granulosa = Estrogen factory (FSH-driven)" |
| Dominant follicle selection | "Survival of the Most Sensitive" (most FSH receptors wins) |
| Cervical mucus at ovulation | EWCM + Ferning + Spinnbarkeit |
| Progesterone test timing | Day of ovulation + 7 days (mid-luteal) |
This is a shared conversation. Sign in to Orris to start your own chat.