1. All about Imaging renal tumors radiology
1. All about Imaging renal tumors radiology keep more images, benign malignant both 2. all about Imaging all renal infection and it's complications and genitourinary tb. Make more tables and flow charts
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
IMAGING OF RENAL TUMORS & RENAL INFECTIONS - COMPREHENSIVE RADIOLOGY GUIDE
Sources: Grainger & Allison's Diagnostic Radiology (9780323760751), Brenner & Rector's The Kidney (9780323532655), Campbell Walsh Wein Urology (9780323546423)
PART 1: IMAGING OF RENAL TUMORS
Overview: Imaging Modalities for Renal Masses
| Modality | Role | Key Advantage |
|---|---|---|
| Ultrasound (US) | First-line; cyst vs. solid differentiation | No radiation; widely available |
| CE-CT (multiphase) | Gold standard for detection, characterisation, staging | >90% accuracy; detects fat, calcification |
| MRI | Problem-solving; fat detection; VHL surveillance | Superior soft-tissue contrast; no iodinated contrast |
| CT Urography (CTU) | Upper tract urothelial tumours | Sensitivity 97%, specificity 93% for TCC |
| PET | Limited role in RCC | Used in metastatic staging/monitoring |
| Angiography | Spoked-wheel sign in oncocytoma; vascular mapping | Pre-op embolisation |
CT Protocol for Renal Mass
┌─────────────────────────────────────────────────────────┐
│ CT RENAL MASS PROTOCOL (4-PHASE) │
├──────────────┬──────────────────────────────────────────┤
│ UNENHANCED │ Detect calcification, fat (<-10 HU AML) │
│ │ Baseline HU measurement │
├──────────────┼──────────────────────────────────────────┤
│ CORTICO- │ ~25-40 sec post-contrast │
│ MEDULLARY │ Detect angiogenesis (clear cell RCC) │
│ PHASE │ Identify pseudotumours │
├──────────────┼──────────────────────────────────────────┤
│ NEPHRO- │ ~80-100 sec post-contrast │
│ GRAPHIC │ BEST PHASE for tumour detection │
│ PHASE │ Most tumours maximally conspicuous here │
├──────────────┼──────────────────────────────────────────┤
│ EXCRETORY/ │ ~5-10 min post-contrast │
│ PYELOGRAPHIC │ Assess collecting system, TCC │
│ PHASE │ Filling defects in renal pelvis/ureter │
└──────────────┴──────────────────────────────────────────┘
Enhancement criteria:
↑ >20 HU (unenhanced → nephrographic) = DEFINITE enhancement → NEOPLASM
↑ 10-20 HU = EQUIVOCAL → MRI or biopsy
↑ <10 HU = NO enhancement → likely cyst
Pseudoenhancement: artefact from CT reconstruction algorithms in small cysts
BENIGN RENAL TUMORS
1. Angiomyolipoma (AML)
Pathology: Benign hamartoma - fat + smooth muscle + vascular elements (±cartilage)
Imaging:
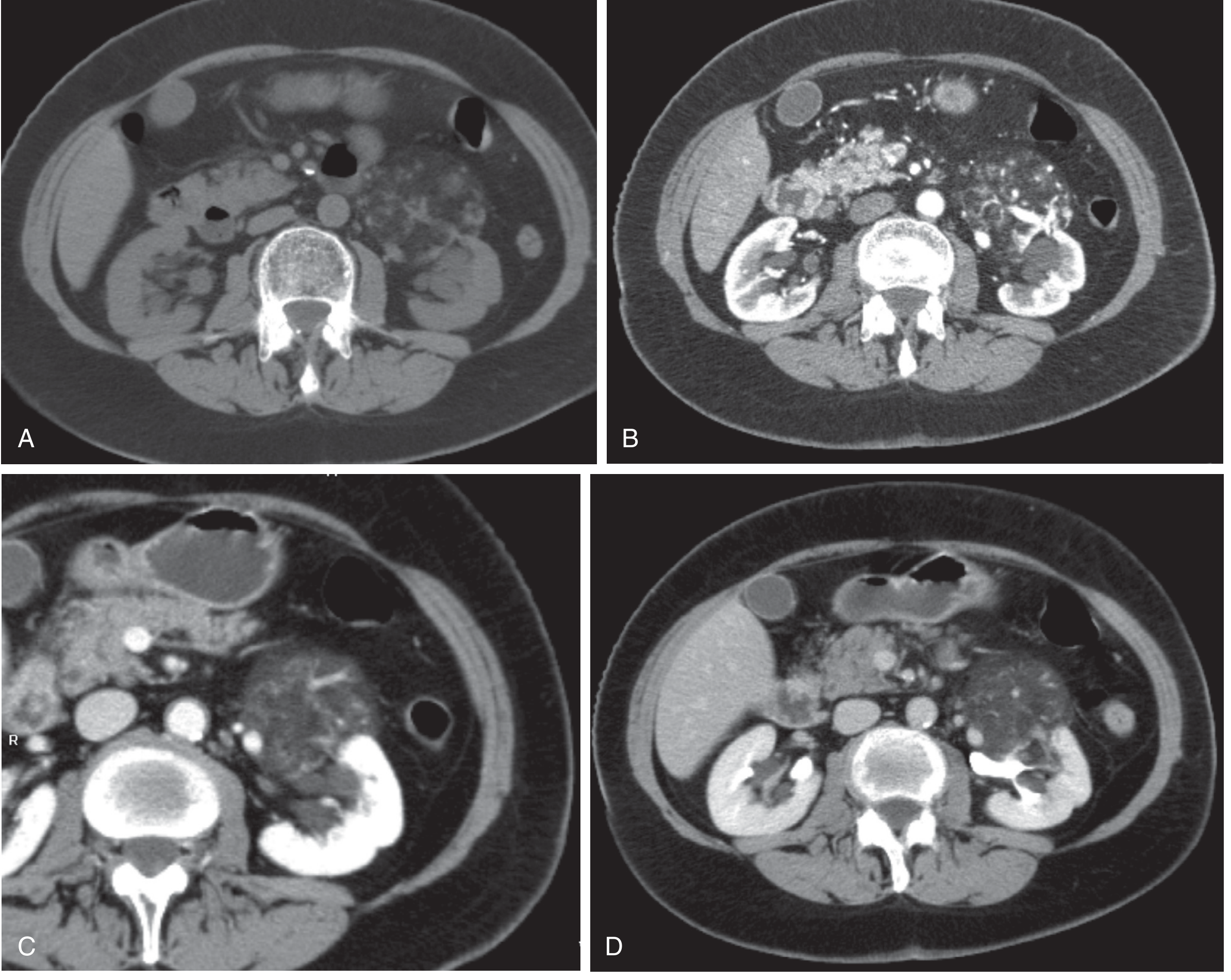
Fig. Angiomyolipoma: CT noncontrast (A), corticomedullary phase (B), nephrographic phase (C), and excretory phase (D). The fat-containing mass projects anteriorly from the left kidney and demonstrates enhancement throughout. - Brenner & Rector's The Kidney
| Feature | Finding |
|---|---|
| US | Solid, hyperechoic (due to fat) |
| CT - unenhanced | Low attenuation < -10 HU (macroscopic fat) - DIAGNOSTIC |
| CT - enhanced | Variable enhancement depending on composition |
| MRI T1 | High signal (fat) |
| MRI T2 | High signal (fat) |
| MRI - fat saturation | Signal drops on fat-suppressed sequences |
| Opposed-phase MRI | "India ink" artifact at tumour-parenchyma interface |
| Minimal-fat AML | Only tiny fat; very difficult - use chemical shift MRI |
Key Points:
- Fat in any renal lesion = AML virtually certain
- Multiple/bilateral AMLs → think Tuberous Sclerosis
- AML ≤4 cm: monitor
- AML >4 cm: increased haemorrhage risk → consider surgery/embolisation
- Wunderlich syndrome = spontaneous retroperitoneal haemorrhage from AML
2. Oncocytoma
Pathology: Benign; arises from proximal collecting tubule epithelium; ~5-7% of renal tumours
| Feature | Finding |
|---|---|
| CT | Solid mass, homogeneous enhancement; central stellate scar (25-30% of cases) |
| MRI | Homogeneous; central scar hypointense on T1, variable T2 |
| Angiography | Classic "spoked-wheel" pattern |
| CEUS | Rim enhancement |
Key Imaging Challenge: Cannot reliably distinguish from RCC on CT. Surgery generally required for diagnosis.
Recent MRI evidence: combined ADC values (diffusion-weighted) + enhancement ratios on multiphasic MRI may differentiate oncocytoma from malignancy, but not yet validated for routine practice.
3. Renal Adenoma
- Most common benign renal tumour
- Almost always <2-3 cm
- Location: corticomedullary
- US: solid appearance
- CE-CT: uniform enhancement
- No characteristic features to distinguish from other solid tumours
4. Renal Cysts - Bosniak Classification
BOSNIAK CLASSIFICATION SYSTEM
────────────────────────────────────────────────────────────────────
Category │ Features │ Malignancy │ Management
─────────┼───────────────────────────────────┼────────────┼──────────
I │ Simple cyst; thin wall; water │ ~0% │ No follow-up
│ attenuation; no enhancement │ │
─────────┼───────────────────────────────────┼────────────┼──────────
II │ Few thin septae (<1 mm) │ <5% │ No follow-up
│ Fine calcifications; <3 cm │ │
│ High-density cysts (>70 HU) │ │
│ Nonenhancing │ │
─────────┼───────────────────────────────────┼────────────┼──────────
IIF │ Multiple thin septae │ ~5-10% │ Imaging
│ Slightly thickened walls/septae │ │ follow-up
│ Coarse/nodular calcification │ │
│ Minimal perceived enhancement │ │
─────────┼───────────────────────────────────┼────────────┼──────────
III │ Thick irregular walls or septae │ ~50% │ Surgical
│ Measuring enhancement present │ │ resection
─────────┼───────────────────────────────────┼────────────┼──────────
IV │ Solid enhancing components │ ~90-100% │ Surgical
│ Enhancing nodules in wall │ │ resection
────────────────────────────────────────────────────────────────────
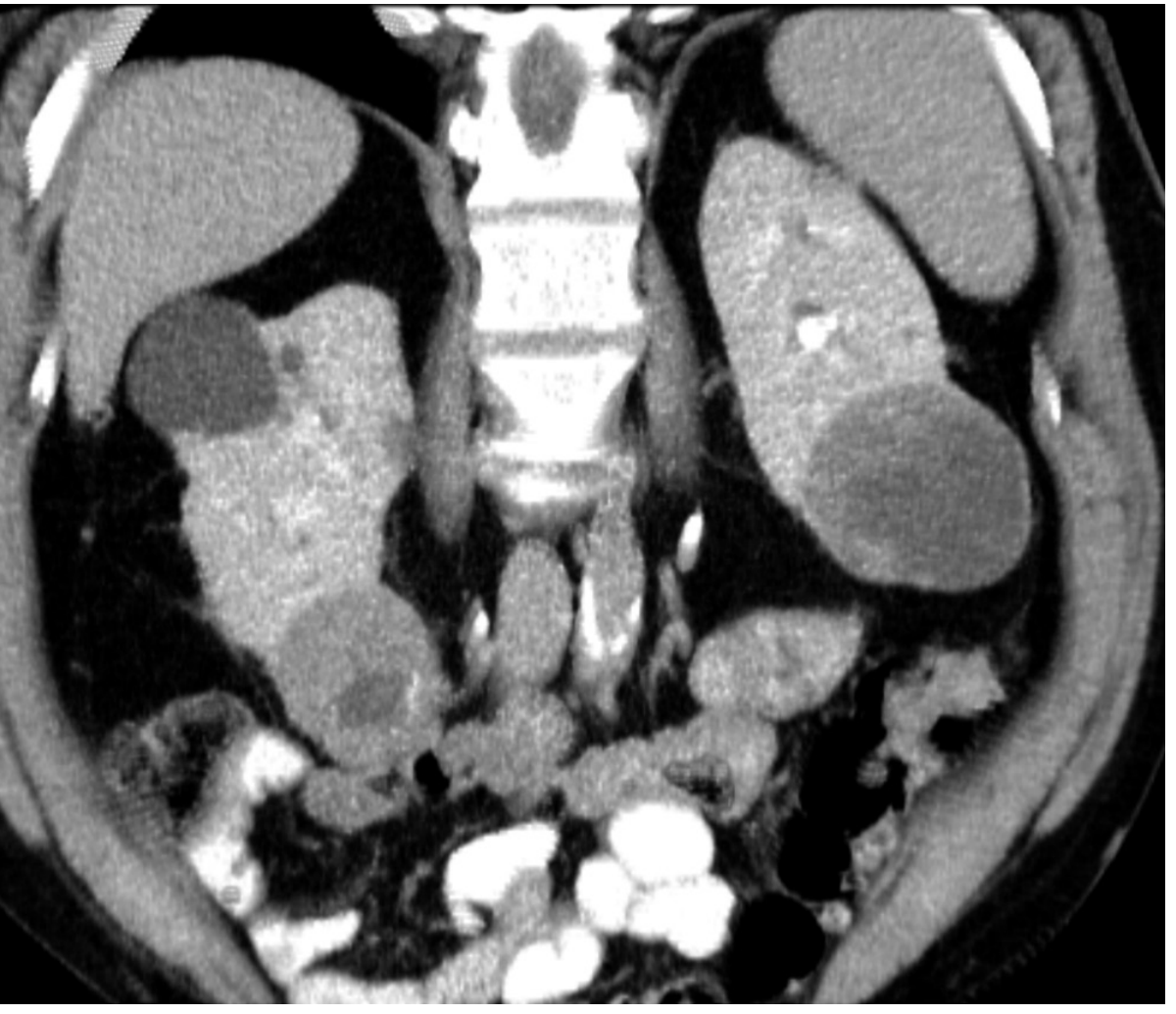
Fig. Bosniak category IV left renal cyst - CT coronal nephrographic phase. Left lower pole cystic mass with internal solid component - proved to be papillary type RCC. Right lower pole solid mass with central necrosis is clear cell RCC. Right upper pole shows Bosniak I cysts. - Brenner & Rector's
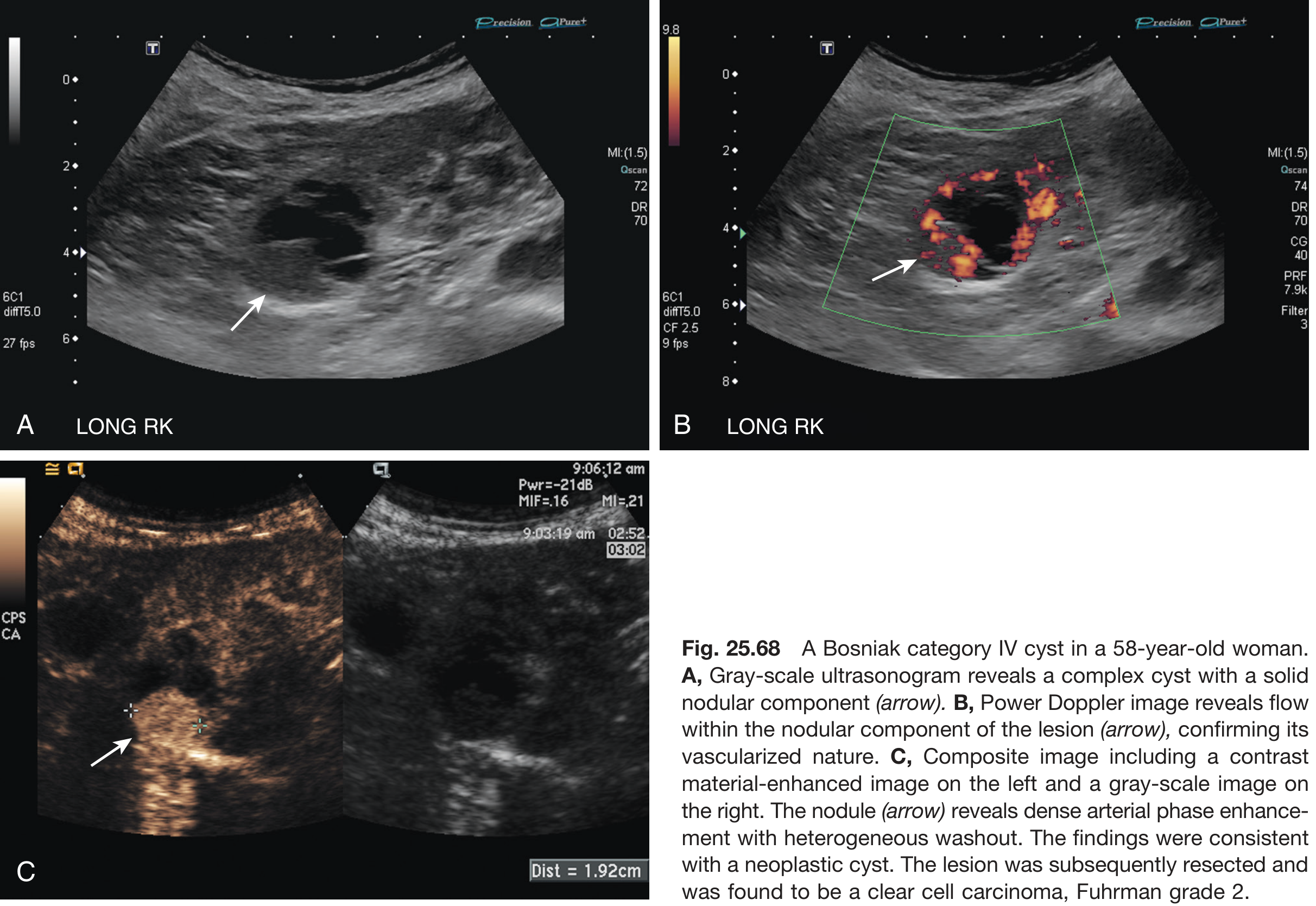
Fig. Bosniak category IV cyst, 58F. (A) Grey-scale US: complex cyst with solid nodular component. (B) Power Doppler: flow within nodule confirming vascularisation. (C) CEUS: dense arterial-phase enhancement with heterogeneous washout - clear cell carcinoma Fuhrman grade 2. - Brenner & Rector's
MALIGNANT RENAL TUMORS
1. Renal Cell Carcinoma (RCC)
Epidemiology: Most common renal malignancy (85%); peak 60-70 years; M>F
Histological Subtypes and Imaging Features:
| Subtype | Frequency | CT Enhancement | CT Characteristics | MRI |
|---|---|---|---|---|
| Clear Cell (ccRCC) | 70-75% | Avid heterogeneous enhancement | Large; haemorrhage + necrosis common | Heterogeneously hyperintense T2; hypointense T1 |
| Papillary | 10-15% | Mild (25-30 HU only) | Often bilateral/multifocal; calcification | Hypointense T2 (haemosiderin); enhancement poor |
| Chromophobe | 5% | Mild (25-30 HU) | Spoke-wheel pattern; calcification | Hypointense T2 |
| Collecting duct | <1% | Variable | Central; infiltrative | Variable |
CT Enhancement Rule:
- Clear cell: >84 HU corticomedullary phase (avid)
- Papillary/Chromophobe: typically <84 HU (mild)
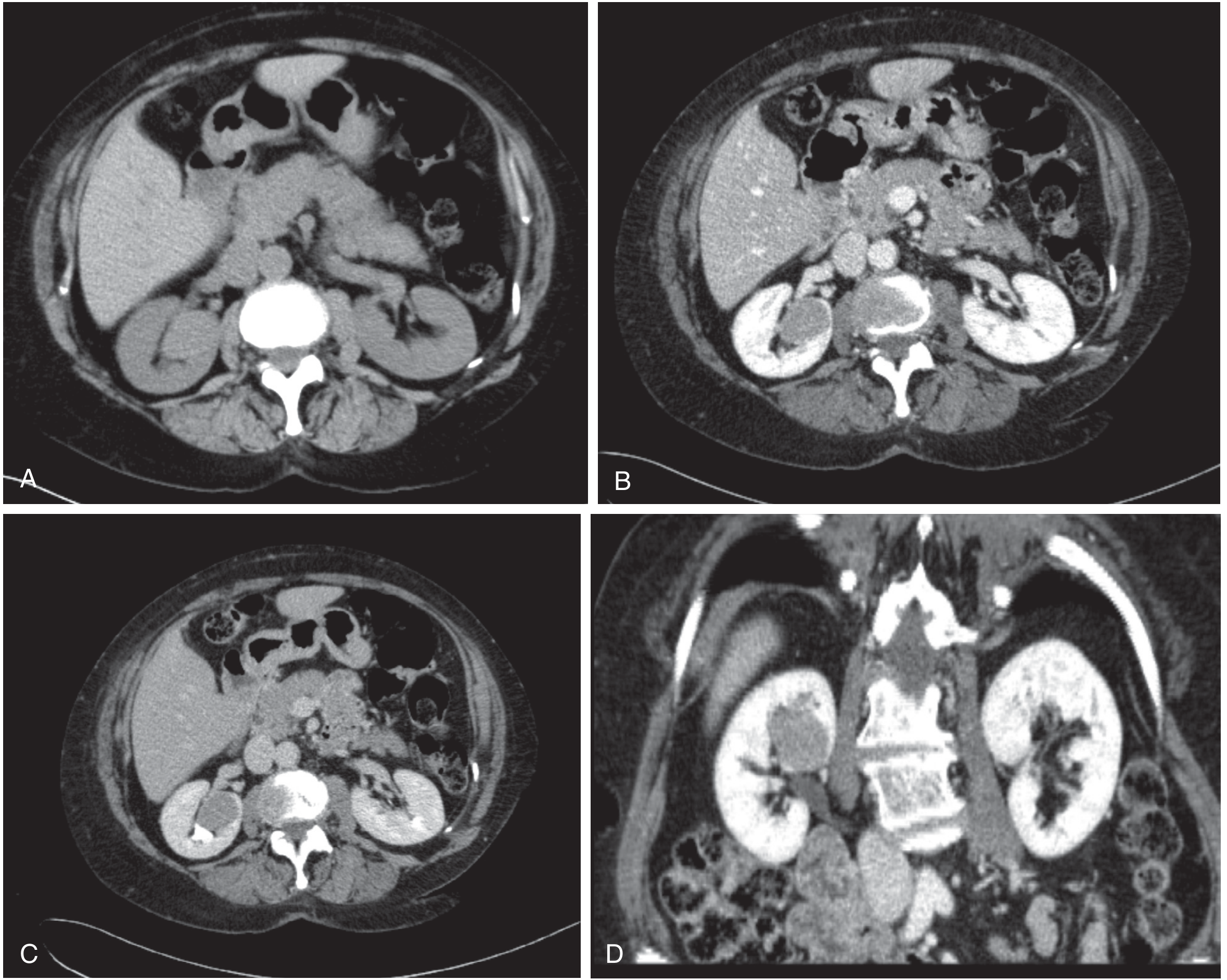
Fig. Renal cell carcinoma CT. (A) Non-contrast: right renal mass slightly hyperdense. (B,C,D) Enhanced: mass enhancement surrounded by normal renal parenchyma - nephrographic and coronal phases demonstrate stage I RCC. - Brenner & Rector's
Robson Staging of RCC:
ROBSON STAGING - RENAL CELL CARCINOMA
══════════════════════════════════════════════════════════
Stage I │ Confined to renal parenchyma by renal capsule
│ CT: mass within kidney; intact pseudocapsule
──────────┼───────────────────────────────────────────────
Stage II │ Extends through capsule into PERINEPHRIC FAT
│ Still within GEROTA'S FASCIA
│ CT: stranding in perinephric fat; Gerota intact
──────────┼───────────────────────────────────────────────
Stage III │ IIIA: Tumour extends into RENAL VEIN or IVC
│ IIIB: Regional retroperitoneal lymph nodes
│ IIIC: Veins AND nodes
──────────┼───────────────────────────────────────────────
Stage IVA │ Outside Gerota's fascia
│ Adjacent organ invasion (not ipsilateral adrenal)
──────────┼───────────────────────────────────────────────
Stage IVB │ DISTANT METASTASES
│ Sites: Lungs > Mediastinum > Liver > Bone
══════════════════════════════════════════════════════════
IVC Thrombus Assessment (Stage IIIA):
- CT: filling defect in renal vein/IVC; enhancing thrombus = tumour thrombus
- MRI: highly accurate for IVC involvement - coronal gadolinium-enhanced T1WI
- Key to surgery: level of IVC thrombus determines approach (infrahepatic vs. suprahepatic)
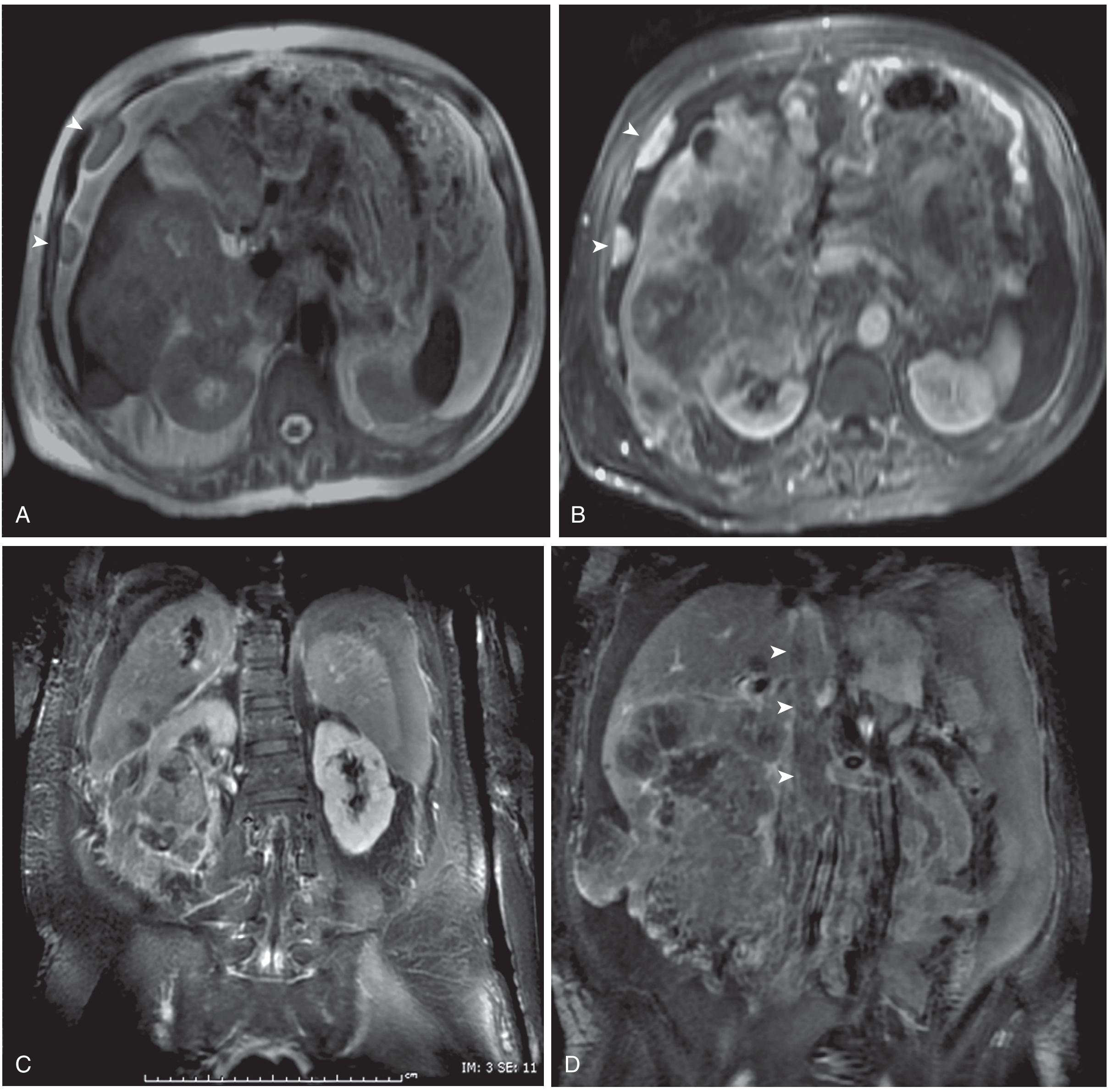
Fig. Metastatic clear cell RCC, stage IV. (A,B) T2-weighted and gadolinium-enhanced T1 axial: large heterogeneous mass, liver invasion and peritoneal metastases. (C,D) Coronal T1+Gad: IVC invasion to level of hepatic veins (arrowheads). - Brenner & Rector's
MRI Features of RCC:
| MRI Sequence | Finding |
|---|---|
| T1WI | Hypointense to isointense (heterogeneous with haemorrhage = hyperintense foci) |
| T2WI | Most commonly heterogeneously hyperintense |
| Pseudocapsule | Hypointense rim on T2 (best for staging; if intact → perinephric fat not invaded) |
| DWI | Restricted diffusion; ADC values aid characterisation |
| Gad-enhanced | Enhances less than normal cortex; clear cell > papillary > chromophobe |
| Opposed-phase | Intraluminal lipid causes signal drop |
2. Transitional Cell Carcinoma (TCC/Urothelial Carcinoma)
Locations: Renal pelvis > ureter > bladder
CT Urography Features:
- Filling defect in renal pelvis or ureter during excretory phase
- Enhancing soft-tissue mass contrasted against low-attenuation urine
- Nephrographic/urothelial phase (60 sec) superior to excretory phase (5 min)
- CTU sensitivity 97%, specificity 93% vs. gold standard retrograde pyelography
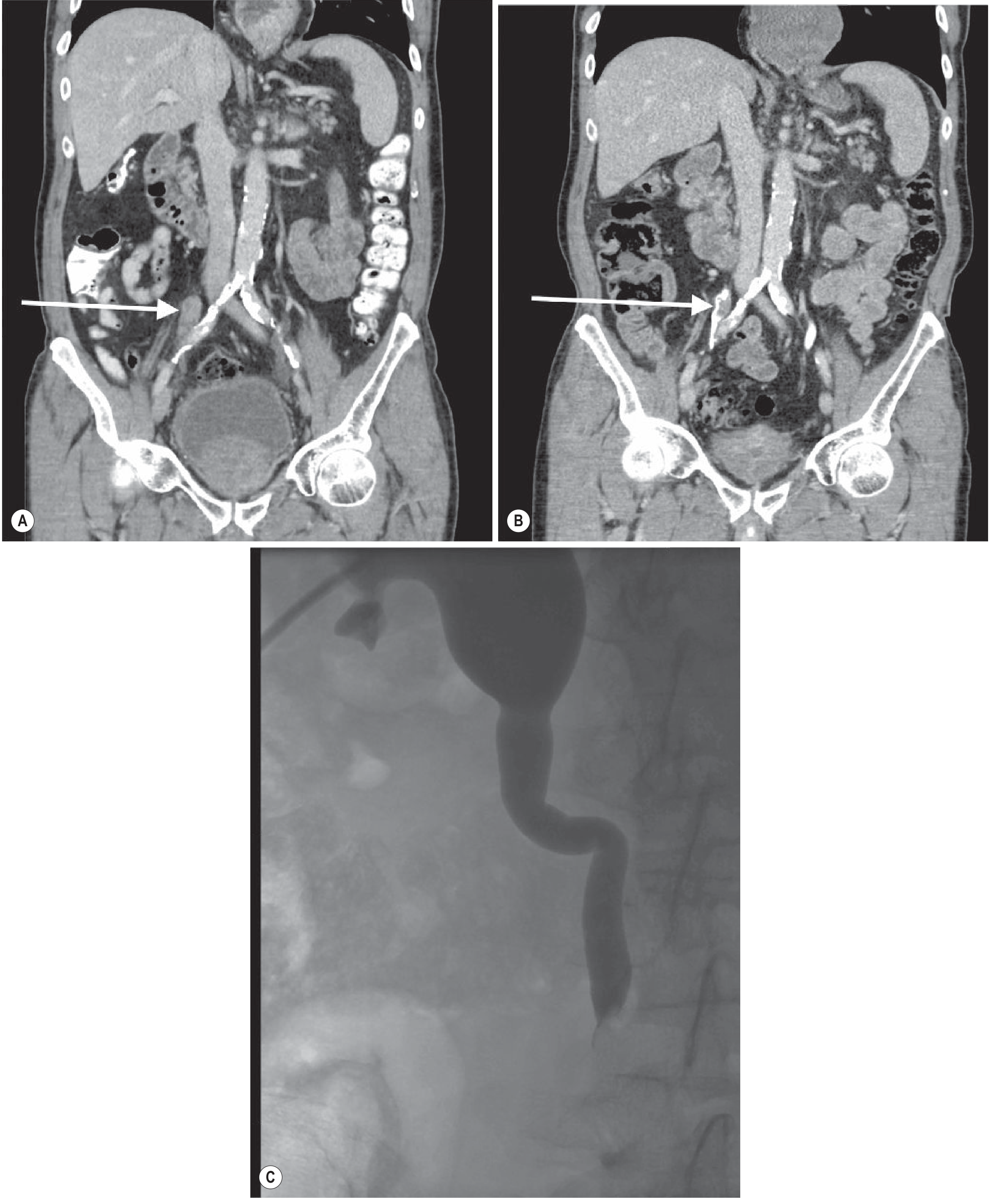
Fig. TCC of ureter. (A,B) Enhancing mass in distal right ureter on CTU (arrows). (C) Antegrade pyelography: abrupt filling defect in ureter due to mass. - Grainger & Allison's
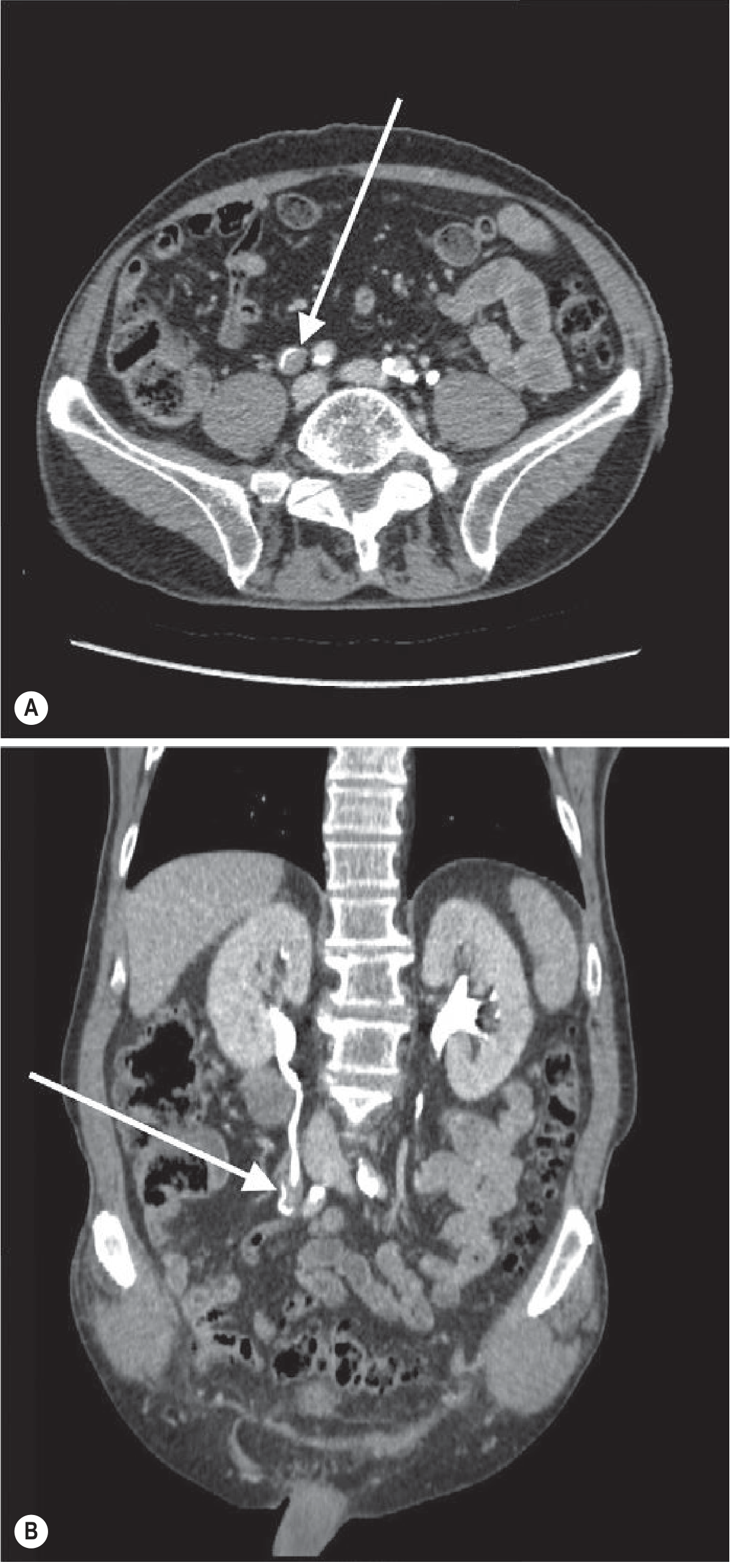
Fig. TCC of ureter - filling defect in right ureter on delayed-phase CT urogram (arrows A,B). - Grainger & Allison's
3. Wilms' Tumour (Nephroblastoma)
- Most common renal tumour in children (peak 3-4 years)
- CT: large heterogeneous mass; enhances heterogeneously; claw of renal tissue
- US: mixed echogenicity; may contain haemorrhage/necrosis
- IVC thrombus in ~10%
- Bilateral in 5-10%
4. Renal Lymphoma
- Usually secondary (haematogenous spread)
- CT patterns: multiple bilateral masses > solitary mass > perinephric soft tissue > diffuse infiltration
- Homogeneous; minimal enhancement; "wrap around" renal vessels
5. Renal Metastases
- Common primaries: lung, breast, colon, melanoma
- Usually bilateral; small; minimal enhancement
- CT: multiple hypoenhancing nodules
FLOWCHART: Approach to an Incidental Renal Mass
INCIDENTAL RENAL MASS DISCOVERED ON IMAGING
│
▼
Is it a CYST?
(round; smooth; water attenuation ~0 HU; no enhancement)
/ \
YES NO (solid or complex)
│ │
▼ ▼
Bosniak Classification Does it contain FAT?
(See table above) (<-10 HU on unenhanced CT)
/ \
YES NO
│ │
▼ ▼
ANGIOMYOLIPOMA Measure enhancement:
Unenhanced → Nephrographic
│
┌──────────────────────────────────┐
│ >20 HU = DEFINITE ENHANCEMENT │
│ 10-20 HU = EQUIVOCAL │
│ <10 HU = NO ENHANCEMENT │
└──────────────────────────────────┘
│ │ │
▼ ▼ ▼
NEOPLASM MRI / Biopsy Simple cyst
(RCC most likely) to clarify No follow-up
│
▼
STAGING CT (chest/abdomen/pelvis)
± MRI for IVC thrombus assessment
│
┌───────────┴────────────────┐
▼ ▼
Small (<3 cm) Large / Complex
Partial nephrectomy Radical nephrectomy
or ablation (±IVC thrombectomy)
PART 2: IMAGING OF RENAL INFECTIONS AND COMPLICATIONS
Overview: Renal Infection Spectrum
RENAL INFECTION SPECTRUM (Ascending >> Haematogenous)
──────────────────────────────────────────────────────────────────
UNCOMPLICATED COMPLICATED SEVERE/SPECIAL
───────────────── ─────────────────── ────────────────
Acute pyelonephritis Renal abscess Emphysematous
(imaging rarely Perinephric abscess pyelonephritis
needed) Pyonephrosis Xanthogranulomatous
Papillary necrosis pyelonephritis
Renal tuberculosis
Fungal infection
──────────────────────────────────────────────────────────────────
When to Image in Renal Infection
IMAGING INDICATIONS IN PYELONEPHRITIS
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
✘ NOT responding to antibiotics within 72 hours
✘ Unclear diagnosis
✘ Coexisting stone disease + possible obstruction
✘ Diabetes mellitus with poor response
✘ Immunocompromised patient
✘ Suspicion of abscess or complicated infection
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
MODALITY OF CHOICE: CT (nephrographic phase)
1. Acute Pyelonephritis (APN)
Imaging Findings:
| Modality | Findings |
|---|---|
| US (often normal) | Loss of corticomedullary differentiation; focal/diffuse swelling; decreased echogenicity; Power Doppler: focal hypoperfusion |
| CE-CT (best test) | Wedge-shaped areas of decreased density (renal pyramid → cortex); streaky/striated nephrogram; focal or global swelling; perinephric fat stranding; Gerota's fascia thickening |
| MRI | Wedge-shaped T2 hyperintense zones; reduced enhancement; restricted diffusion on DWI |
| Scintigraphy (DMSA) | Photopenic defects in cortex (most sensitive for parenchymal involvement especially in children) |
CT key: Sharp demarcation between diseased tissue and normally enhancing adjacent parenchyma during nephrographic phase. Streaky/striated nephrogram = pathognomonic.
2. Renal Abscess
FORMATION PATHWAY:
Pyelonephritis → Microabscesses → Coalescence → MACROABSCESS
│
Rim of granulation tissue
│
Rupture through renal capsule
│
PERINEPHRIC ABSCESS
| Feature | Renal Abscess | Perinephric Abscess |
|---|---|---|
| US | Thick-walled hypoechoic/complex fluid; internal echoes/debris | Fluid collection surrounding kidney |
| CT | Rounded low-density mass; thick irregular rim enhancement; gas bubbles if gas-forming organism | Soft-tissue density collection in perinephric space; Gerota's fascia thickening; loculations |
| MRI | T2 hyperintense; T1 hypointense; DWI restricted | Similar pattern, extends beyond capsule |
| Treatment | Antibiotics ± CT-guided drainage | CT-guided drainage usually required |
3. Pyonephrosis
Definition: Infected hydronephrosis - pus in an obstructed collecting system
| Feature | Finding |
|---|---|
| US | Dilated collecting system with echogenic debris/layering; "dirty shadowing"; mobile debris |
| CT | Dilated pelvicalyceal system; high-attenuation debris; wall thickening; perinephric stranding |
| Gas | If gas-forming organism: echogenic foci with dirty shadowing (US); air in collecting system (CT) |
| Urgency | Medical emergency - needs urgent nephrostomy/drainage |
4. Emphysematous Pyelonephritis (EPN)
Definition: Necrotising infection with gas in renal parenchyma; 90% in diabetics; high mortality without treatment
| Class | CT Findings | Mortality | Treatment |
|---|---|---|---|
| Class I | Gas in collecting system only | Low | Antibiotics + drainage |
| Class II | Gas in renal parenchyma; no extension | Moderate | Antibiotics + drainage ± percutaneous |
| Class III A | Extension to perinephric space | High | Percutaneous drainage |
| Class III B | Extension to pararenal space | High | Percutaneous drainage |
| Class IV | Bilateral EPN or solitary kidney | Very high (>50%) | Emergency nephrectomy |
CT = gold standard: mottled gas densities within renal parenchyma/collecting system; "bubbly" or "streaky" pattern
5. Xanthogranulomatous Pyelonephritis (XGP)
Definition: Chronic destructive infection; often secondary to staghorn calculus + obstruction; lipid-laden macrophages
XGP IMAGING CHARACTERISTICS
────────────────────────────────────────────────────────────────
• Enlarged, non-functioning kidney (90% unilateral)
• Central staghorn calculus (75% of cases)
• Focal (segmental) or diffuse replacement of parenchyma
• Multiple lipid-containing rounded low-density areas
(xanthoma cells = fat density on CT!)
• Extension into perinephric fat and adjacent organs
• "Bear paw" sign: central high-density stone surrounded by
multiple low-density masses (xanthoma nodules)
────────────────────────────────────────────────────────────────
| Modality | Findings |
|---|---|
| Plain film / KUB | Staghorn calculus; enlarged renal shadow |
| US | Enlarged kidney; central echogenic calculus; hypoechoic masses; posterior shadowing |
| CT | BEST modality: central calculus; multiple water-density (−10 to +15 HU) rounded masses replacing parenchyma; extension into retroperitoneum |
| IVP | Non-functioning kidney ("silent kidney") |
Differential: Must distinguish from renal TB and renal cell carcinoma.
6. Papillary Necrosis
Causes (Mnemonic: POSTCARDS)
- Pyelonephritis
- Obstruction
- Sickle cell disease
- Tuberculosis
- Cirrhosis/analgesics
- Analgesic nephropathy
- Renal vein thrombosis
- Diabetes mellitus
- Sjogren's/shock
| Modality | Findings |
|---|---|
| IVP / CT urography | Filling defect in calyx (necrotic papilla); "moth-eaten" calyx; "ring sign" (necrotic papilla surrounded by contrast); "lobster claw" or "ball on tee" deformity |
| US | Hypoechoic triangular area in medulla; papilla may be echogenic |
| CT | Hyperdense necrotic papilla (before sloughing); defect after sloughing; calyceal clubbing |
PART 3: GENITOURINARY TUBERCULOSIS (GU TB)
Epidemiology
- 1.1-1.5% of all TB cases; 5-6% of extrapulmonary TB
- Hematogenous seeding during primary pulmonary infection → renal cortex
- High O₂ tension of cortex = favourable for M. tuberculosis
- Men infected twice as often as women
- Mean latent period from pulmonary TB to GU disease: 22 years (range 1-46 yrs)
- Reactivation usually unilateral (bilateral in 25%)
Organ Involvement in GU TB:
| Organ | Frequency |
|---|---|
| Kidneys | 60-100% |
| Ureters | 19-41% |
| Bladder | 15-20% |
| Prostate/Epididymis | 20-50% of men |
Pathological Progression of Renal TB:
RENAL TB PATHOLOGICAL SEQUENCE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Hematogenous seeding → Cortical granulomas (latent)
│
▼
Caseating granulomas in cortex → CALYCEAL EROSIONS
(earliest imaging finding!)
│
▼
PAPILLARY NECROSIS → cavitation of papillae
│
▼
CALYCEAL CLUBBING + DILATION
│
▼
HYDRONEPHROSIS (ureteric strictures)
│
▼
RENAL PARENCHYMAL CAVITATION
│
▼
DYSTROPHIC CALCIFICATION (granuloma → caseous necrosis → calcium)
│
▼
AUTONEPHRECTOMY ("putty kidney" / "chalk kidney")
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Imaging Findings in GU TB (by Organ):
Kidney:
| Stage/Feature | IVP | CT | US |
|---|---|---|---|
| Early: Calyceal erosions | Smudged, irregular calyces | Calyceal irregularity | Non-specific |
| Papillary necrosis | "Moth-eaten" appearance | Low-density papillary defects | Hypoechoic papillae |
| Cavitation | Cavities communicating with calyx | Parenchymal cavities with thick walls | Complex masses |
| Hydronephrosis | Dilated pelvicalyceal system | Dilated collecting system + strictures | Dilated PCS |
| Calcification | Stippled/dystrophic calcium | Cortical/curvilinear/putty calcification | Echogenic foci + shadowing |
| Autonephrectomy | Non-functioning kidney | Shrunken, calcified, non-enhancing kidney | Small hyperechoic kidney |
Ureter:
| Feature | Imaging Appearance |
|---|---|
| Ureteric strictures | Multiple; irregular; "pipe-stem ureter" |
| Beading | Alternating strictures + dilatations |
| "Golf-hole" ureter | Short, straight, wide ureteric orifice on cystoscopy |
| Location | Often distal ureter first; may progress proximally |
| CT | Thickened ureteric wall; irregular lumen; peritubular stranding |
Bladder:
| Feature | Imaging |
|---|---|
| Cystitis/thickening | Wall thickening (US, CT) |
| "Thimble bladder" | Severely contracted, fibrotic bladder on CT/IVP |
| Calcifications | Bladder wall calcification on CT |
| Capacity | Markedly reduced volume |
Male Genital TB:
| Organ | Finding |
|---|---|
| Epididymis | Enlarged, heterogeneous; calcifications; "beaded" on US |
| Prostate | Nodular/granulomatous; elevated PSA - mimics PCa |
| Vas deferens | Thickened, "beaded" appearance on US |
| Testis | Non-tender mass; complex epididymo-orchitis |
CT vs. IVP in GU TB:
| Feature | IVP | CT |
|---|---|---|
| Currently preferred? | No (historical standard) | YES (now preferred) |
| Detects calcification | Moderate | Excellent |
| Shows cavitation | Poor | Excellent |
| Ureteric detail | Good (with retrograde) | Good |
| Extraurinary spread | No | Excellent (lymph nodes, adrenal) |
| Non-functioning kidney | Silent/white out | Can assess residual parenchyma |
| Follow-up during Rx | IVP every 6 months for ureteric strictures | CT when indicated |
GU TB Key Imaging Signs:
GU TB IMAGING SIGNS SUMMARY
─────────────────────────────────────────────────────
KIDNEY
• "Moth-eaten" calyces = papillary necrosis (earliest)
• "Phantom calyx" = amputation of infundibulum
• "Putty kidney" = totally calcified autonephrectomy
• "Lobar nephronia" = focal parenchymal destruction
URETER
• "Pipe-stem" ureter = rigid, strictured ureter
• "Saw-tooth" ureter = multiple strictures
• "Golf-hole" ureteric orifice = cystoscopy finding
BLADDER
• "Thimble bladder" = contracted fibrotic bladder
EPIDIDYMIS
• "Beaded epididymis" = multiple granulomas
─────────────────────────────────────────────────────
Diagnostic Algorithm for Suspected GU TB:
SUSPECTED GU TB
(sterile pyuria + haematuria + relevant history)
│
▼
3x early morning urine for AFB culture
(positive in 75-90% of active cases)
│
▼
CT ABDOMEN/PELVIS
(preferred over IVP)
│
┌─────┴───────────────────────────┐
▼ ▼
CHARACTERISTIC FINDINGS NON-DIAGNOSTIC
(calyceal erosion, calcification, │
strictures, cavitation) ▼
│ TISSUE BIOPSY ±
▼ PCR of urine
CONFIRM with culture/PCR
│
▼
TREATMENT:
4-drug regimen (HRZE × 2 months)
→ 2-drug (HR × 4 months)
│
▼
FOLLOW-UP IVP every 6 months
(detect new ureteric strictures!)
│
▼
Ureteric obstruction developing?
│
YES ┤
▼
Balloon dilation / stent / reimplantation
(corticosteroids do NOT prevent)
Complications of GU TB and Their Management:
| Complication | Imaging | Management |
|---|---|---|
| Ureteric stricture | CT/IVP: obstruction + hydroureter | Balloon dilation; ureteral stent; reimplantation |
| Hydronephrosis | US/CT: dilated PCS | Nephrostomy if infected; drainage |
| Autonephrectomy | CT: shrunken calcified kidney | Nephrectomy (pain, hypertension, drug resistance) |
| Thimble bladder | CT: tiny contracted bladder | Bladder augmentation surgery |
| Fistula | CT/fistulograms | Surgical repair |
| Renal failure | CT small kidneys bilaterally | Dialysis/transplant |
Fungal Urinary Tract Infection (Special Mention)
- Usually Candida species (C. albicans >50%)
- Risk: ICU, immunocompromised, indwelling catheters, broad-spectrum antibiotics
- Imaging:
- US/CT: filling defects in collecting system = fungus balls (echogenic masses without shadowing)
- Bladder: focal wall thickening
- Can cause hydronephrosis if fungus ball obstructs UPJ or ureter
Summary Comparison Table: Complicated Renal Infections
| Condition | Key CT Finding | Key Risk Factor | Treatment |
|---|---|---|---|
| Acute APN | Wedge-shaped nephrogram defect | UTI | Antibiotics |
| Renal abscess | Thick rim-enhancing fluid collection | DM; IV drug use | Antibiotics ± drainage |
| Perinephric abscess | Perinephric fluid + gas | Ruptured renal abscess | CT-guided drainage |
| Pyonephrosis | Dilated PCS + debris + gas | Obstruction + UTI | Emergency nephrostomy |
| Emphysematous PN | Gas in renal parenchyma | Diabetes (90%) | Drainage ± nephrectomy |
| XGP | Staghorn calculus + fat-density masses | Staghorn stone | Nephrectomy |
| Papillary necrosis | "Moth-eaten" calyces; "ring sign" | DM, analgesics, sickle cell | Treat underlying cause |
| Renal TB | Calyceal erosion → calcification | Prior pulmonary TB | HRZE × 2 mo + HR × 4 mo |
| Fungal infection | Fungus ball in collecting system | Immunosuppression | Antifungals ± drainage |
Quick Reference: Imaging Modality of Choice
| Clinical Scenario | First Choice | Second Choice |
|---|---|---|
| Incidental renal mass | CT (multiphase) | MRI |
| Fat-containing renal mass | CT unenhanced | MRI chemical shift |
| Complex cyst characterisation | CT (Bosniak) | MRI |
| TCC / urothelial tumour | CT Urography | Retrograde pyelography |
| RCC staging / IVC thrombus | CT + MRI | CT alone |
| Uncomplicated pyelonephritis | None needed | US (if obstruction suspected) |
| Complicated pyelonephritis | CE-CT (nephrographic phase) | US |
| Emphysematous pyelonephritis | CT | CT (no alternative) |
| XGP | CT | US + plain film |
| GU Tuberculosis | CT | IVP (follow-up for strictures) |
| Renal calculi acute | Unenhanced CT (low-dose) | US + KUB |
| Pregnancy + suspected stone | MRI urography | US |
| Renal failure - size/obstruction | US | Unenhanced CT |
Key Textbook References:
- Grainger & Allison's Diagnostic Radiology (Chapter 26 - Uroradiology), pp. 719-734
- Brenner & Rector's The Kidney (Chapter 25 - Renal Imaging), pp. 1107-1120; Chapter 36 - Renal Infection, pp. 1644-1650
- Campbell Walsh Wein Urology (Chapter 32 - Genitourinary Tuberculosis)
This is a shared conversation. Sign in to Orris to start your own chat.