Apical impulse and apex beat difference
Reading File
Searching the Web
apical impulse vs apex beat difference cardiology examination
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Now I have enough high-quality textbook and web data to give a thorough answer.
Apical Impulse vs. Apex Beat
These two terms are frequently used interchangeably in clinical practice, but they are not identical - and understanding the distinction matters, particularly in abnormal cardiac states.
Definitions
| Term | Definition |
|---|---|
| Apex Beat | The lowermost and outermost visible/palpable pulsation on the chest wall, corresponding to the anatomical tip (apex) of the heart. It is the point farthest from the sternum and farthest down. |
| Apical Impulse | The cardiac pulsation felt (or seen) at the region of the cardiac apex, caused by left ventricular systolic contraction against the chest wall. It reflects the character, contour, and timing of LV contraction - not just the location. |
The Key Difference
The apex beat is a positional/anatomical landmark - it tells you where the heart's tip is. The apical impulse is a functional descriptor - it tells you how the left ventricle is contracting and transmitting force to the chest wall.
Fuster & Hurst's The Heart (15th ed.) explicitly recommends using the term "apical impulse" rather than "point of maximal impulse (PMI)" because:
"Patients with significantly enlarged right ventricles might have parasternal lifts that are more prominent than the left ventricular apical impulse."
In other words, the point of maximal impulse (the most forceful pulsation) may NOT always be the apex beat when the RV is massively enlarged - the parasternal region may be more prominent.
Normal State
In a healthy individual:
- The apex beat = apical impulse = PMI - all three coincide at the 5th intercostal space, midclavicular line
- Occupies an area ≤3 cm in diameter
- Brief, early systolic outward movement
When They Diverge (Pathological States)
| Condition | Apex Beat | Apical Impulse Character |
|---|---|---|
| LV dilatation (e.g., MR, DCM) | Displaced laterally and inferiorly | Diffuse, sustained, hyperdynamic |
| LV hypertrophy (pressure overload - AS, HTN) | Normal position | Sustained, forceful ("heaving"), not displaced |
| RV enlargement | Apex shifted laterally (passively pushed) | LV apical impulse may be weak; parasternal lift dominates |
| Massive pleural effusion | Pushed contralaterally | May be absent or faint |
| Massive pulmonary collapse | Pulled ipsilaterally | May be absent |
| Pericardial effusion | Apex may be impalpable | Apical impulse absent |
| Mitral stenosis | Normal or minimal displacement | "Tapping" apical impulse (palpable S1 due to loud, snapping MV closure) |
- Fuster and Hurst's The Heart, 15th Edition, pp. 81-82
- Harrison's Principles of Internal Medicine 22E, Cardiovascular Examination chapter
- S Das: A Manual on Clinical Surgery, 13th Edition, p. 408
Practical Note: "Tapping" Apex Beat in Mitral Stenosis
In mitral stenosis, the apex beat has a characteristic "tapping" quality - caused by a palpable loud S1 (snapping mitral valve closure). The position may be normal, but the impulse character is clearly abnormal. This is a classic example where the apex beat location and the apical impulse character give different information.
Summary
- Apex beat = anatomical position of the cardiac apex on the chest wall (lowermost, outermost cardiac pulsation)
- Apical impulse = the quality, character, size, and timing of the LV systolic contraction felt at the apex
- In most people, both refer to the same physical point
- The distinction matters most when the RV is enlarged (the PMI may shift to the parasternal area, while the true apex beat is the LV tip) or when the character of the impulse is more diagnostically important than its location (e.g., sustained vs. tapping vs. hyperdynamic)
What is parasternal heave
Finding Sources
Searching the Web
parasternal heave clinical examination causes right ventricle
Reading File
Reading File
Loading Image
Here is a complete breakdown of the parasternal heave:
Parasternal Heave (Parasternal Lift / Thrust)
Definition
A parasternal heave is a visible and/or palpable forward (anterior) lifting movement of the lower left parasternal area during systole. It is caused by a hypertrophied or enlarged right ventricle pushing against the chest wall, since the RV is the most anteriorly placed cardiac chamber, directly behind the sternum.
Anatomy - Why the RV Causes This
The right ventricle lies directly beneath the lower sternum and left parasternal region. When the RV enlarges (due to pressure or volume overload), its systolic contraction generates enough force to visibly and palpably lift the chest wall in this region.
How to Elicit It (Examination Technique)
Three methods are described in Fuster & Hurst's The Heart (15th ed.):
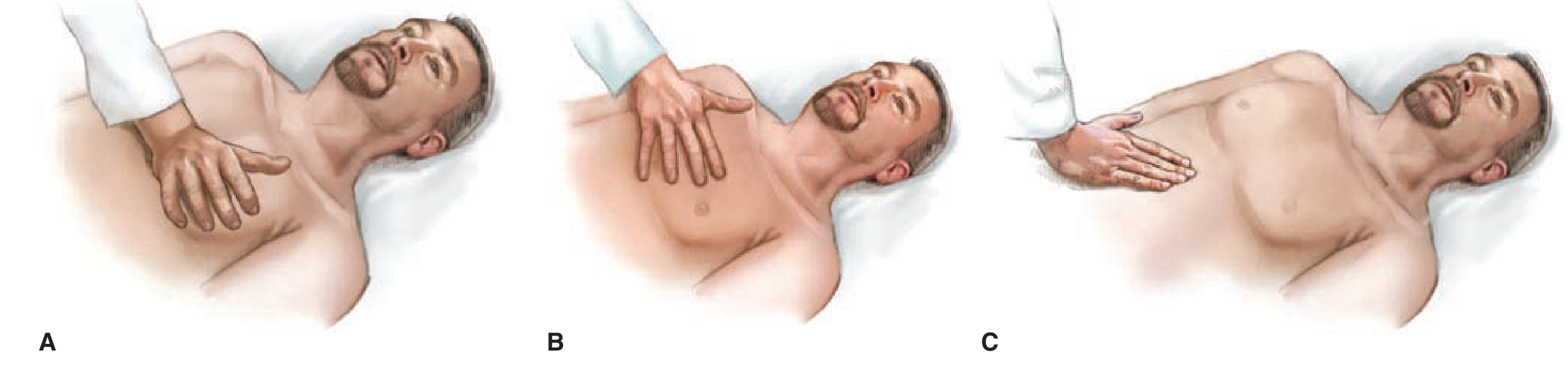
- (A) Thenar/hypothenar method: Place the heel/ulnar border of the right hand flat on the left lower sternal border with fingers angled toward the left shoulder. A heave lifts the heel of the hand with each systole.
- (B) Finger method: Place the index, middle, and ring fingers over the 3rd, 4th, and 5th intercostal spaces at the left parasternal line.
- (C) Subxiphoid method: Place the right hand under the xiphoid process, pointing upward - particularly useful in patients with COPD/emphysema where the hyperinflated lungs push the heart inferiorly.
Patient position: Supine, at 30-45 degrees. Examine during quiet respiration.
Grading
| Grade | Description |
|---|---|
| Grade 1 | Visible impulse but not palpable |
| Grade 2 | Visible and palpable, but can be obliterated with pressure |
| Grade 3 | Visible, palpable, and cannot be obliterated with pressure |
Causes
RV Pressure Overload (RV Hypertrophy - Sustained heave)
- Pulmonary hypertension (primary or secondary) - most common
- Pulmonary stenosis
- Cor pulmonale (COPD, pulmonary fibrosis, recurrent PE)
- Eisenmenger syndrome
RV Volume Overload (RV Dilatation - heave may be less sustained)
- Atrial septal defect (ASD) - classic cause
- Tricuspid regurgitation
- Pulmonary regurgitation
- Total anomalous pulmonary venous connection (TAPVC)
Left Atrial Enlargement
- Mitral stenosis - the massively enlarged LA can push the RV (and entire heart) anteriorly, producing a parasternal heave even without primary RV disease. This is a left atrial heave, transmitted via the RV.
Associated Clinical Signs
When a parasternal heave is present, look for these accompanying signs to identify the cause:
| Sign | Suggests |
|---|---|
| Loud/palpable P2 | Pulmonary hypertension |
| Fixed split S2 | ASD |
| Opening snap + mid-diastolic murmur | Mitral stenosis |
| Pansystolic murmur at LLSB increasing with inspiration | Tricuspid regurgitation |
| Raised JVP + peripheral edema | Right heart failure |
| Ejection systolic murmur at LUSB | Pulmonary stenosis |
Important Caveat
A parasternal lift can also be present in thin patients or those with pectus excavatum (funnel chest) even with a normal-sized RV, because the chest wall is closer to the heart. Always interpret in clinical context. - Fuster and Hurst's The Heart, 15th Edition, p. 81-82
Quick Summary
A parasternal heave = RV enlargement until proven otherwise. Palpate with the heel of the hand at the left sternal border. Grade it, characterize it (sustained = pressure overload; non-sustained = volume overload), and seek the underlying cause through associated clinical and investigative findings.
A short video demonstration is available here:
This is a shared conversation. Sign in to Orris to start your own chat.