Copd
Reading File
Finding Sources
Searching PubMed
"chronic obstructive pulmonary disease"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"COPD"[MeSH Terms] AND "exacerbation" AND "treatment"
Here is a thorough overview of COPD drawn from multiple authoritative medical textbooks:
Chronic Obstructive Pulmonary Disease (COPD)
Definition
COPD is a progressive, largely irreversible obstructive lung disease characterized by persistent airflow limitation caused by an abnormal inflammatory response of the lung to noxious particles or gases - most commonly cigarette smoke. It encompasses two main phenotypes that frequently coexist:
- Emphysema - destruction of alveolar walls and elastic support
- Chronic Bronchitis - persistent productive cough for at least 3 months per year in 2 consecutive years
COPD is the 3rd most common cause of death in the United States, accounting for over $40 billion per year in direct and indirect healthcare costs. (Katzung's Basic and Clinical Pharmacology)
Etiology & Risk Factors
| Factor | Details |
|---|---|
| Cigarette smoking | Major risk factor (responsible for ~85-90% of cases) |
| Air pollutants | Industrial dust, indoor biomass smoke |
| Alpha-1 antitrypsin (α1-AT) deficiency | Genetic risk for panacinar emphysema |
| Recurrent infections | Particularly Haemophilus influenzae |
| Occupational exposures | Dust, chemicals, fumes |
Importantly, even smokers with normal spirometry may show progressive CT changes in bronchial wall thickness and lung tissue loss.
Pathophysiology
Emphysema
- Enlargement of air spaces distal to terminal bronchioles from destruction of alveolar elastic support
- Proteases (mainly from neutrophils) destroy elastin - in normal lungs, α1-antitrypsin inhibits these proteases
- Two subtypes:
- Centriacinar (centrilobular) - most common; smoking-related; upper lobe predominance
- Panacinar - associated with α1-antitrypsin deficiency; lower lobe predominance
- Results in: increased lung compliance, static and dynamic lung hyperinflation, increased chest volume ("barrel chest"), dyspnea
- Blood gases: relatively preserved oxygenation at rest ("pink puffer")
Chronic Bronchitis
- Mucus hypersecretion in proximal airways due to surface epithelial mucous metaplasia and submucosal gland expansion
- Combined with ciliary dysfunction - impaired mucociliary clearance
- Small airway mucus occlusion correlates with severity of airflow obstruction
- Histology: enlarged mucus-secreting glands, goblet cell metaplasia, inflammation, bronchiolar wall fibrosis
- Blood gases: hypoxemia and hypercapnia ("blue bloater")
- MUC5AC concentration increased 10-fold and MUC5B 3-fold in severe COPD
Airflow Limitation & Exercise Intolerance
The key drivers of dyspnea in COPD are:
- Decreased ventilatory capacity - increased airway resistance + reduced lung elastic recoil
- Increased ventilatory requirement - V/Q mismatch
- Dynamic hyperinflation - during exercise, end-expiratory lung volume (EELV) rises, inspiratory reserve volume (IRV) falls, causing "neuromechanical uncoupling" and severe dyspnea
- Cor pulmonale (right-sided heart failure) in advanced disease from chronic hypoxic pulmonary vasoconstriction
(Fishman's Pulmonary Diseases and Disorders)
Diagnosis
Spirometry (gold standard)
- FEV1/FVC < 0.70 (post-bronchodilator) - confirms airflow obstruction
- FEV1 is reduced; FVC is normal or near-normal
- Obstruction is not fully reversible (unlike asthma)
GOLD Severity Classification (based on FEV1 % predicted)
| GOLD Grade | FEV1 % predicted |
|---|---|
| 1 - Mild | ≥ 80% |
| 2 - Moderate | 50-79% |
| 3 - Severe | 30-49% |
| 4 - Very Severe | < 30% |
Clinical Features
- Dyspnea (progressive, especially on exertion)
- Chronic cough with sputum production
- Wheezing and chest tightness
- Barrel chest (increased AP diameter due to hyperinflation)
- Decreased breath sounds, prolonged expiratory phase
- Cyanosis in advanced chronic bronchitis
ABG Findings (classic case - (Costanzo Physiology))
- PaO2 ↓ (e.g., 60 mmHg)
- PaCO2 may be ↓ (if hyperventilating) or ↑ (in severe disease)
- Elevated A-a gradient due to V/Q mismatch
Treatment
Stable COPD (Katzung's Basic and Clinical Pharmacology)
Step-by-step approach:
| Symptom level | First-line treatment |
|---|---|
| Acute relief | Inhaled SABA (albuterol) or SAMA (ipratropium) or combination |
| Persistent exertional dyspnea | LABA and/or LAMA (long-acting anticholinergic) |
| Severe obstruction or frequent exacerbations | Add ICS (inhaled corticosteroid) |
| Persistent exacerbations despite triple therapy | Roflumilast (PDE4 inhibitor) |
Key points:
- LAMA (e.g., tiotropium) is often preferred over LABA as first-line for stable COPD
- ICS use is cautious in COPD - less effective than in asthma, and associated with increased risk of bacterial pneumonia
- ICS recommended when: severe airflow obstruction, prior exacerbations, blood eosinophils are high (biomarker-guided)
- Theophylline: no longer routinely recommended (failed to show benefit in large RCT)
- Roflumilast (selective PDE4 inhibitor): approved for COPD, improves FEV1 and reduces exacerbation frequency
Non-pharmacologic:
- Smoking cessation (most important intervention to slow decline)
- Pulmonary rehabilitation
- Long-term oxygen therapy (LTOT) when PaO2 ≤ 55 mmHg or SpO2 ≤ 88%
- Influenza and pneumococcal vaccination
Acute Exacerbations of COPD (AECOPD)
Defined as acute worsening of respiratory symptoms beyond normal day-to-day variation. Major drivers of COPD morbidity and mortality.
Common triggers:
- Viral respiratory infections (most common)
- Bacterial infections (H. influenzae, S. pneumoniae, M. catarrhalis)
- Air pollution
Management:
| Intervention | Details |
|---|---|
| Short-acting bronchodilators | SABA + SAMA (first-line) |
| Systemic corticosteroids | Oral prednisone (5-day course; reduces duration and severity) |
| Antibiotics | β-lactams, doxycycline, or azithromycin (covering H. influenzae) |
| Controlled oxygen | Target SpO2 88-92% (avoid hyperoxia) |
| NIV (BiPAP) | For hypercapnic respiratory failure (pH < 7.35, PaCO2 > 45) |
COPD vs. Asthma - Key Differences
| Feature | COPD | Asthma |
|---|---|---|
| Age at onset | Older (usually >40) | Any age |
| Smoking history | Almost always present | Not required |
| Airflow obstruction | Fixed / irreversible | Reversible |
| Predominant inflammation | Neutrophilic | Eosinophilic |
| Response to ICS | Poor | Excellent |
| Course | Progressive decline | Episodic |
Complications
- Cor pulmonale - right heart failure from pulmonary hypertension
- Polycythemia - from chronic hypoxemia
- Respiratory failure - hypercapnic type II
- Spontaneous pneumothorax - from bullae rupture
- Lung cancer - markedly elevated risk in smokers with COPD
Sources: Robbins & Kumar Basic Pathology | Fishman's Pulmonary Diseases and Disorders | Katzung's Basic and Clinical Pharmacology, 16th Ed. | Costanzo Physiology, 7th Ed.
What are biomarker-guided ICS treatment strategies in COPD?
Finding Sources
Searching PubMed
"COPD" AND "eosinophil" AND "inhaled corticosteroid"
Finding Sources
Reading Article
PMID: 38919905
Reading Article
PMID: 39103901
Finding Sources
Reading Article
PMID: 40651490
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Excellent sources retrieved. Here is the full answer:
Biomarker-Guided ICS Treatment Strategies in COPD
The Core Concept: Why Biomarkers?
ICS therapy in COPD is not universally beneficial - unlike in asthma, COPD inflammation is predominantly neutrophilic, not eosinophilic, and ICS offers limited benefit while carrying real risks (especially bacterial pneumonia). Biomarker-guided use allows clinicians to identify the subset of COPD patients with type 2 (eosinophilic) inflammation who are likely to benefit.
The mechanism of ICS benefit in COPD involves changes in inflammatory gene transcription and modulation of β2-adrenergic receptor function, but these effects are amplified in eosinophil-driven disease.
"The blood eosinophil count is a potentially useful prognostic and theragnostic biomarker in COPD. Thresholds, rather than specific target blood eosinophil counts, are associated with beneficial effect." (Fishman's Pulmonary Diseases and Disorders)
Primary Biomarker: Blood Eosinophil Count (BEC)
The blood eosinophil count (cells/µL) is the most validated and clinically used biomarker. The GOLD 2024/2025 guidelines define three actionable thresholds:
| BEC Threshold | ICS Recommendation |
|---|---|
| < 100 cells/µL | ICS unlikely to benefit; do NOT add ICS |
| 100-299 cells/µL | ICS may be considered IF ≥2 moderate exacerbations or ≥1 severe hospitalization per year |
| ≥ 300 cells/µL | ICS likely to benefit; add ICS even with fewer exacerbations |
(GOLD 2025 Guidelines, as cited in Harrison's Principles of Internal Medicine 22E)
GOLD 2025 Follow-Up Treatment Algorithm (Eosinophil-Guided)
The official GOLD follow-up algorithm integrates BEC into step-up/step-down decisions:
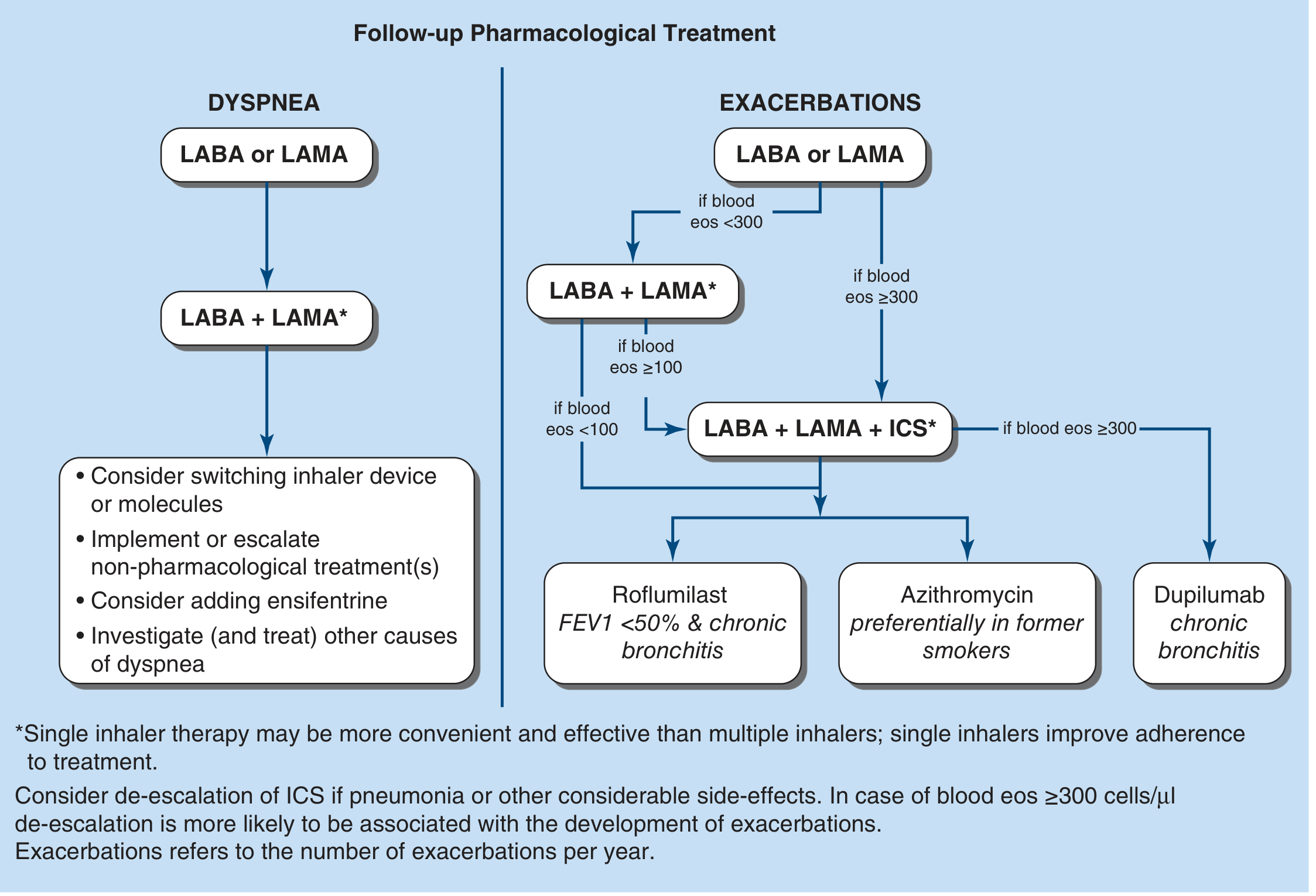
Key decision points:
- For dyspnea-dominant disease: Eosinophils do not guide ICS use - step up from LABA/LAMA regardless
- For exacerbation-dominant disease:
- BEC < 100: Step up to LABA + LAMA only (ICS not recommended)
- BEC 100-299: Step up to LABA + LAMA + ICS if ≥2 exacerbations or hospitalization
- BEC ≥ 300: Step up directly to triple therapy (LABA + LAMA + ICS)
- If still on LABA + LAMA + ICS and exacerbating:
- Add Roflumilast if FEV1 <50% + chronic bronchitis
- Add Azithromycin (preferentially in former smokers)
- Add Dupilumab if BEC ≥300 with chronic bronchitis
(Harrison's Principles of Internal Medicine 22E, GOLD 2025)
ICS Initiation - Key Rules
Initial Treatment (GOLD Groups A/B/E)
- Group A (low symptoms, low exacerbation risk): Start with a bronchodilator; ICS not indicated
- Group B (high symptoms, low exacerbation risk): Start with LABA or LAMA; ICS not routinely indicated
- Group E (high exacerbation risk): LABA + LAMA first-line; add ICS only if BEC ≥300 cells/µL
ICS De-escalation (Withdrawal)
A 2024 systematic review and meta-analysis (PMID 38919905) found:
- ICS withdrawal is safe and feasible when long-acting bronchodilators are maintained
- No consistent difference in exacerbation frequency or FEV1 decline between withdrawal and continuation arms
- Caveat: ICS withdrawal in patients with BEC ≥300 cells/µL is associated with a higher risk of exacerbations - de-escalation should be done cautiously in this group
When to consider ICS withdrawal/de-escalation:
- Development of pneumonia
- Other significant ICS side effects (osteoporosis, hyperglycemia, adrenal suppression)
- BEC persistently < 100 cells/µL (suggests minimal T2 inflammation)
- Widespread ICS prescribing outside guidelines (most common reason)
Triple Therapy and the 100-299 "Gray Zone"
A post-hoc analysis of the KRONOS trial (PMID 39103901) found that even in the intermediate BEC range (100-299 cells/µL):
- Triple therapy (budesonide/glycopyrronium/formoterol - BGF) reduced moderate/severe exacerbation rates by 47-56% vs. dual LABA+LAMA
- FEV1 improvement of 62-73 mL favoring BGF
- Benefit seen even without prior exacerbation history and in moderate COPD
This suggests clinicians may want to consider triple therapy step-up for patients with BEC >100 cells/µL and persistent/worsening symptoms - challenging the strict ≥300 threshold.
Emerging Biomarkers: Beyond Eosinophils
A 2025 phase 3 trial analysis (BOREAS; PMID 40651490) examined biomarkers predicting response to dupilumab (anti-IL-4/IL-13) in COPD:
| Biomarker | Role |
|---|---|
| Blood eosinophils ≥300 cells/µL | Primary selection criterion; higher BEC = greater exacerbation reduction |
| FeNO (fractional exhaled NO) | Higher baseline FeNO predicts greater dupilumab benefit (p=0.043); dupilumab reduced FeNO by ~29% |
| Total IgE | Reduced ~23% with dupilumab vs. placebo |
| Eotaxin-3 | Type 2 chemokine; reduced with dupilumab |
| PARC (CCL18) | Reflects T2 airway inflammation; reduced ~14% with dupilumab |
These findings support a broader type 2 inflammation panel (BEC + FeNO + IgE + eotaxin-3) for identifying who benefits from biologics targeting the IL-4/IL-13 axis.
ICS Risks That Make Biomarker Guidance Essential
| Risk | Details |
|---|---|
| Pneumonia | Consistent signal across ICS trials in COPD; risk highest with fluticasone propionate |
| Osteoporosis | Long-term systemic ICS effect |
| Hyperglycemia | Particularly in diabetics |
| Oral candidiasis/dysphonia | Local effect; mitigated by spacer + mouth rinsing |
| Adrenal suppression | With high-dose or prolonged use |
The pneumonia risk is the main reason why the GOLD guidelines moved away from routine ICS use and toward BEC-guided prescribing.
Summary: The Eosinophil Decision Framework
BEC < 100 cells/µL → No ICS (risk > benefit)
BEC 100-299 cells/µL → ICS if ≥2 exacerbations OR hospitalization
(consider step-up in gray zone per KRONOS data)
BEC ≥ 300 cells/µL → Add ICS; triple therapy preferred
ICS withdrawal risky - monitor closely
BEC ≥ 300 + ongoing exacerbations on triple therapy → Consider dupilumab
Sources: Fishman's Pulmonary Diseases and Disorders | Harrison's Principles of Internal Medicine 22E (2025) | Katzung's Basic and Clinical Pharmacology 16th Ed. | GOLD 2025 Report | PMID 38919905 | PMID 39103901 | PMID 40651490
This is a shared conversation. Sign in to Orris to start your own chat.