Epidemiology traid
Reading File
Searching the Web
epidemiological triad host agent environment model
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive content from Park's Textbook of Preventive and Social Medicine. Here is the full answer:
The Epidemiological Triad
The epidemiological triad (also called the epidemiological triangle) is the foundational model of disease causation in epidemiology. It was developed as a response to the limitations of the older "germ theory," which proposed a simple one-to-one relationship between a single microbial agent and disease.
The key insight: not everyone exposed to Mycobacterium tuberculosis develops TB, and not everyone exposed to beta-haemolytic streptococci develops rheumatic fever. Other factors - relating to the host and environment - equally determine whether disease occurs. This demanded a broader model synthesising three basic factors.
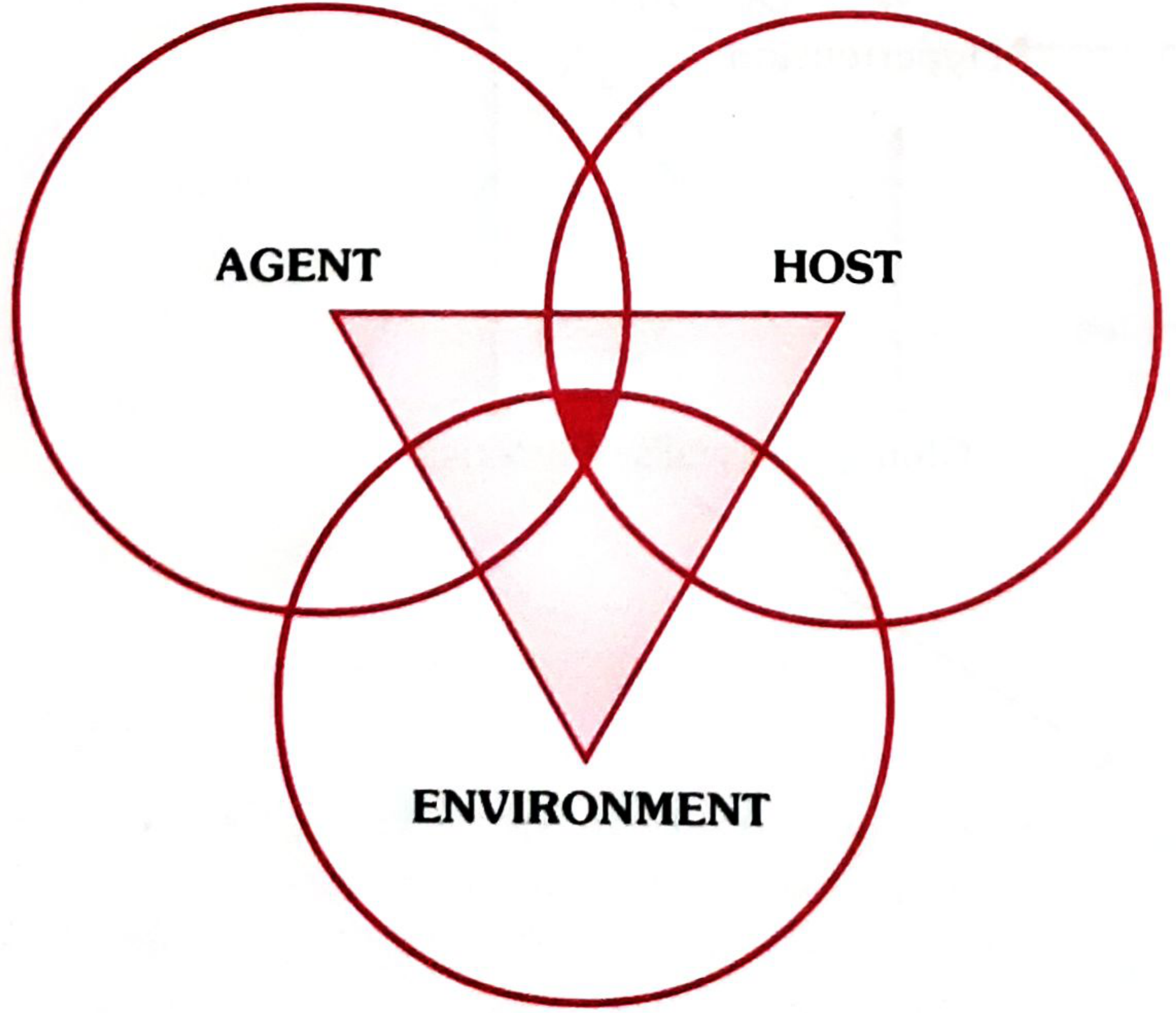
The three components interact as shown in the Venn diagram below. Disease occurs at the point where all three overlap (the dark central zone):
1. AGENT
The disease agent is the factor whose presence or absence (excess or deficiency) is necessary for the disease to occur. Agents are classified into six categories:
| Category | Examples |
|---|---|
| Biological | Viruses, bacteria, rickettsiae, fungi, protozoa, metazoa |
| Nutrient | Proteins, fats, carbohydrates, vitamins, minerals (excess or deficiency) |
| Physical | Excessive heat, cold, radiation, pressure, sound, electricity |
| Chemical | Endogenous (urea, bilirubin, ketones) or exogenous (allergens, metals, fumes, pesticides) |
| Mechanical | Chronic friction, trauma, crushing, sprains |
| Absence/Excess of a factor | Hormones (insulin), chromosomal factors (Down syndrome), immunological factors |
Biological agents have specific host-related properties:
- Infectivity - ability to invade and multiply in a host
- Pathogenicity - ability to produce clinically apparent disease
- Virulence - proportion of clinical cases with severe manifestations (measured by case-fatality rate)
Social agents - poverty, smoking, drug/alcohol abuse, unhealthy lifestyles - are also recognised as agents in the modern concept.
2. HOST
The host is the human (or animal) that harbours the disease. In epidemiological terminology, the host is referred to as the "soil" and the disease agent as the "seed."
Host factors are classified as:
- Demographic characteristics - age, sex, ethnicity
- Biological characteristics - genetic makeup, blood groups, biochemical levels (cholesterol), immunological status, physiological organ function
- Social and economic characteristics - socioeconomic status, education, occupation, stress, marital status, housing
- Lifestyle factors - personality traits, nutrition, physical exercise, alcohol, drugs, smoking, behavioural patterns
Host factors determine the outcome of exposure. For example, a malnourished or immunocompromised person exposed to TB is far more likely to develop clinical disease than a healthy, well-nourished person exposed to the same bacillus.
3. ENVIRONMENT
The environment is defined as "all that which is external to the individual human host, living and non-living, and with which he is in constant interaction." It is divided into three components:
a. Physical Environment
Non-living factors: air, water, soil, housing, climate, geography, heat, light, noise, radiation. Defective physical environment (e.g., lack of sanitation) remains the main health problem in developing countries.
b. Biological Environment
All living organisms surrounding the host: insects, rodents, animals, plants, and other humans. This includes vectors (mosquitoes, ticks), reservoirs of infection, and food sources.
c. Psychosocial Environment
Social, cultural, economic, and psychological factors: customs, habits, beliefs, attitudes, social norms, and mental/emotional stressors. These influence behaviour and exposure to agents.
The Interaction
The triad functions as a dynamic balance. Disease occurs when this balance is disrupted - when the agent is virulent enough, the host is sufficiently susceptible, and the environment favours their interaction. The core principle is:
"The mere presence of agent, host, and favourable environmental factors in the prepathogenesis period is not sufficient to start the disease in man. What is required is an interaction of these three factors to initiate the disease process." - Park's Textbook
Role of Time
A fourth element, time, is also recognised in the triangle of epidemiology. Time accounts for:
- Incubation periods
- Duration of illness
- Life expectancy of host or pathogen
- Epidemic thresholds
Public Health Application
The primary mission of epidemiology is to break one leg of the triangle - disrupting the connection among environment, host, and agent - to stop an outbreak. Examples:
- Removing the agent - antibiotic treatment, water chlorination
- Protecting the host - vaccination, improving nutrition
- Modifying the environment - vector control, sanitation improvements
Limitations and Evolution
The classical triad applies best to infectious/communicable diseases. For modern non-communicable diseases (coronary artery disease, cancer, mental illness), the model has been expanded into the multifactorial causation model, where "causative factors" replace the single agent concept, and behaviour, lifestyle, and chronic disease mechanisms are incorporated.
Source: Park's Textbook of Preventive and Social Medicine, p. 44-48
Anemia mukth bharath
Searching the Web
Anemia Mukt Bharat programme India 2018 strategy targets beneficiaries
Finding Sources
Finding Sources
Searching the Web
Anemia Mukt Bharat 6x6x6 six interventions six institutional mechanisms details
Reading Web Page
https://www.pib.gov.in/PressReleaseIframePage.aspx?PRID=2122…
Here is a comprehensive overview of the Anemia Mukt Bharat programme:
Anemia Mukt Bharat (AMB)
Meaning: "Anemia-Free India"
Launched: September 2018
Under: Ministry of Health & Family Welfare (MoHFW), National Health Mission (NHM)
Tagline: Test. Treat. Talk.
Background & Rationale
India carries a massive burden of anemia. As per NFHS-5 data:
- 67.1% of children under 5 are anemic
- 59.1% of adolescent girls are anemic
- 3 in 4 Indian women have low dietary iron intake
- Iron Deficiency Anemia (IDA) causes 1.18% of GDP loss and is the 3rd leading cause of DALYs in women aged 15-44 years
AMB was built on lessons from earlier programmes (timeline below) and designed to cover 450 million beneficiaries - nearly 50% of India's population.
Historical Timeline
| Year | Programme |
|---|---|
| 1970 | National Nutritional Anemia Prophylaxis Programme (NNAPP) |
| 1991 | National Nutritional Anemia Control Programme |
| 2007 | 12 by 12 Initiative |
| 2013 | National Iron Plus Initiative (NIPI) |
| 2018 | Anemia Mukt Bharat (AMB) |
Objective
Reduce the prevalence of anemia by 3 percentage points per year among children, adolescents, and women of reproductive age (15-49 years) between 2018-2022.
Specific target: Reduce anemia in pregnant women from 50% (2016) to 32% by 2022.
India is also committed to the WHO World Health Assembly target of 50% reduction of anemia in women of reproductive age by 2025.
The 6×6×6 Strategy (Core Framework)
The entire programme is structured around 3 sets of 6:
6 TARGET BENEFICIARIES (Life-Cycle Approach)
| # | Beneficiary Group |
|---|---|
| 1 | Children 6-59 months |
| 2 | Children 5-9 years |
| 3 | Adolescent girls AND boys (10-19 years) |
| 4 | Women of Reproductive Age - WRA (15-49 years) |
| 5 | Pregnant women |
| 6 | Lactating mothers (0-6 months postpartum) |
6 INTERVENTIONS
| # | Intervention | Details |
|---|---|---|
| 1 | Prophylactic IFA Supplementation | Color-coded, age-specific (see table below) |
| 2 | Deworming (Biannual) | Albendazole 400 mg; via National Deworming Day (NDD) |
| 3 | Intensified year-round BCC | Behaviour Change Communication / SBCC campaigns |
| 4 | Digital testing of anemia | Point-of-care hemoglobin testing using digital hemoglobinometers |
| 5 | IFA fortification of foods | Mandatory in government-funded health programmes (midday meal, ICDS, etc.) |
| 6 | Addressing non-nutritional causes | Malaria (NVBDCP), hemoglobinopathies (thalassemia, sickle cell), fluorosis (NPPCF) |
IFA Supplementation Schedule (Color-coded)
| Beneficiary | Formulation | Frequency |
|---|---|---|
| Children 6-59 months | IFA syrup | Biweekly (twice a week) |
| Children 5-9 years | Pink tablet (small) | Weekly |
| Adolescents 10-19 years | Blue tablet | Weekly |
| Non-pregnant WRA (20-49 yrs) | Red tablet | Weekly |
| Pre-conception / 1st trimester | Folic acid tablet | Daily |
| Pregnant women (from 2nd trimester) + 6 months postpartum | IFA tablet | Daily |
6 INSTITUTIONAL MECHANISMS
| # | Mechanism |
|---|---|
| 1 | Intra-Ministerial Coordination - AMB Steering Committee; bi-annual meetings with MoHFW, MoWCD, MoRD, Ministry of Tribal Welfare, etc. |
| 2 | National AMB Unit (AMBU) - Supports and monitors state-level implementation |
| 3 | National Centre of Excellence & Advanced Research on Anemia Control (NCEAR-A) |
| 4 | Strengthened supply chain & logistics - Reliable IFA procurement and distribution to district/block level |
| 5 | Convergence with other ministries - POSHAN Abhiyaan, School Health Programme, ICDS, NDD |
| 6 | AMB Dashboard & Digital Portal - Real-time tracking of anemia screening, IFA stock, and distribution data |
Key Features
- Life-cycle approach - addresses all vulnerable groups from infancy to reproductive age
- Test-Treat-Talk framework at the facility and community level
- Digital hemoglobinometers at sub-centres and health facilities for point-of-care testing
- Implemented across all villages, blocks, and districts of all States/UTs
- Integrated with POSHAN Abhiyaan (national nutrition mission) and School Health Programme
Recent Progress (2024-25)
As per PIB, April 2025:
- 15.4 crore children/adolescents received IFA supplements in Q2 FY 2024-25
- Digital tools now track real-time anemia screening and supply chain data nationwide
Public Health Significance
- IDA in South Asia accounts for close to $4.2 billion in economic losses annually (Bangladesh, India, Pakistan combined)
- Anemia causes decreased work output, cognitive losses, increased maternal and infant mortality
- AMB addresses both nutritional (iron/folate deficiency) and non-nutritional (malaria, hemoglobinopathies, fluorosis) causes - making it a holistic national strategy
Recent update of it
Searching the Web
Anemia Mukt Bharat 2025 recent updates new guidelines progress
Searching the Web
Anemia Mukt Bharat NFHS-5 results 2024 2025 achievements challenges
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12838808
Reading Web Page
https://www.pib.gov.in/PressReleaseIframePage.aspx?PRID=2122…
Here are the most recent updates on Anemia Mukt Bharat:
Anemia Mukt Bharat - Recent Updates (2024-2025)
1. Current Anemia Burden (NFHS-5 Data - Latest National Picture)
Despite years of intervention, anemia remains a major public health challenge in India:
| Group | Prevalence |
|---|---|
| Children under 5 | 67.1% |
| Adolescent girls | 59.1% |
| Pregnant women | 52.2% |
| Women of Reproductive Age | 3 in 4 have low dietary iron intake |
The NFHS-5 (2019-21) showed that anemia actually increased in several groups compared to NFHS-4, highlighting the gap between programme coverage and actual impact - prompting a reassessment of strategies.
2. New Digital Tool - T4 App (2025)
A major 2025 innovation presented at the South Asia Nutrition Conference, Kathmandu (December 2025) is the T4 Mobile Application - an expansion of the original "Test, Treat, Talk" framework to Test, Treat, Talk & Track:
- Real-time beneficiary tracking - individual hemoglobin records linked to digital hemoglobinometers
- Supply chain management - tracks IFA stock levels at block/district level in real time
- Community IEC dissemination - pushes health communication to frontline workers (ASHAs, ANMs)
- Referral tracking - ensures severe anemia cases are followed up
- Program transparency - dashboard data for program managers at state and national level
Piloted by the Institute of Economic Growth (IEG), New Delhi under the Technical Support Unit of AMB.
3. AMB Index & State Rankings (Published December 2025)
A landmark paper published in Global Health: Science and Practice (Dec 2025) introduced the Anemia Mukt Bharat Index - a composite scoring tool to rank states and UTs by IFA supplementation coverage (2018-19 to 2022-23):
Key findings:
- IFA coverage has grown for all recipient groups between 2017-18 and 2019-20 following AMB implementation
- Coverage more than doubled between 2020-21 and 2022-23, crossing 50% for the first time nationally
- States/UTs now use AMB scorecards as the primary reference for anemia data in Parliament, state trainings, and programme reviews
- Gaps identified: Multi-departmental convergence groups (ICDS, schools) showed lower coverage than health-department-only groups
- No significant gender difference in IFA coverage between school-age boys and girls
- Most coverage variance is state-specific (not gender-based)
- Recommendation: Include HMIS data for WRA (Women of Reproductive Age - the 6th beneficiary group) which is currently underrepresented in the index
4. IFA Coverage Progress (FY 2024-25)
As per PIB, April 2025:
- 15.4 crore (154 million) children and adolescents received IFA supplements in Q2 FY 2024-25 alone
- Programme now operational across all villages, blocks, and districts of all States/UTs
- HMIS updated from April 2023 onward with new indicators for better tracking
5. Integration with Other Schemes (Updated)
AMB is now tightly integrated with:
| Scheme | Integration |
|---|---|
| POSHAN Abhiyaan 2.0 | Shared beneficiaries, monitoring dashboards |
| School Health Programme | Weekly IFA delivery via school teachers |
| National Deworming Day (NDD) | Biannual albendazole + coordinated IFA |
| NVBDCP | Addresses malaria-related anemia in endemic zones |
| Pradhan Mantri Poshan Shakti Nirman (PM POSHAN) | IFA-fortified food in midday meals |
6. Identified Bottlenecks (2025 Research - Jharkhand)
A qualitative study (Cureus, August 2025) on rural Jharkhand identified key implementation gaps:
- Inadequate training of frontline workers (ASHAs, AWWs)
- Irregular IFA supply at block/district pharmacy level
- Poor community awareness and side-effect concerns (nausea, black stools) leading to non-compliance
- Cultural food taboos limiting dietary improvement
- Delayed cord clamping still not universally practised
- Limited infrastructure for digital hemoglobin testing in remote areas
7. Way Forward
- Expansion of the AMB Index to facility-level data (currently state/district level only)
- Strengthen supply chain for last-mile IFA delivery
- Focus on high-burden states (UP, Bihar, Jharkhand, MP, Rajasthan) where anemia prevalence remains highest
- Scaling the T4 digital platform nationally after pilot success
- Continued commitment to the WHO 2025 target: 50% reduction in anemia in women of reproductive age
Bottom line: While AMB has significantly expanded IFA coverage since 2018, the NFHS-5 paradox (rising coverage but still-high prevalence) shows that supplementation alone is insufficient - improved supply chains, compliance, dietary change, and tackling non-nutritional causes (malaria, hemoglobinopathies) remain the biggest challenges going forward.
Anemia mukth barath abhiyan
"Anemia Mukt Bharat Abhiyan" and "Anemia Mukt Bharat" refer to the same programme - the national campaign launched in 2018 under NHM. The word "Abhiyan" simply means "campaign/mission" in Hindi, emphasizing its nature as an active national drive.
I've already covered this in detail in our previous two responses. Here's a focused summary:
Anemia Mukt Bharat Abhiyan - Complete Summary
What is it?
A national campaign (abhiyan) by the Government of India under the Ministry of Health & Family Welfare, launched in September 2018, to eliminate anemia across the life cycle. It operates as part of the Intensified National Iron Plus Initiative (I-NIPI) under NHM.
Full name in Hindi: अनीमिया मुक्त भारत अभियान
Meaning: "Campaign for an Anemia-Free India"
The Core: 6×6×6 Strategy
6 Beneficiaries
- Children 6-59 months
- Children 5-9 years
- Adolescents 10-19 years (boys + girls)
- Women of Reproductive Age (15-49 yrs)
- Pregnant women
- Lactating mothers
6 Interventions
- Prophylactic IFA supplementation (color-coded by age group)
- Biannual deworming (National Deworming Day - albendazole)
- Intensified BCC/SBCC - year-round behavior change communication
- Digital hemoglobin testing - point-of-care screening
- IFA-fortified foods in government programmes (midday meals, ICDS)
- Non-nutritional causes - malaria, hemoglobinopathies (thalassemia, sickle cell), fluorosis
6 Institutional Mechanisms
- Intra-ministerial coordination (MoHFW, MoWCD, MoRD, MoTW)
- National AMB Unit (AMBU)
- National Centre of Excellence & Advanced Research on Anemia Control (NCEAR-A)
- Strengthened supply chain & logistics
- Convergence with POSHAN Abhiyaan, School Health Programme
- AMB Dashboard & Digital Portal (real-time data)
IFA Color-Coding (Key Exam Point)
| Beneficiary | Type | Frequency | Color |
|---|---|---|---|
| 6-59 months | Syrup | Twice a week | - |
| 5-9 years | Small tablet | Weekly | Pink |
| 10-19 years (adolescents) | Tablet | Weekly | Blue |
| WRA 15-49 yrs (non-pregnant) | Tablet | Weekly | Red |
| Pre-conception / 1st trimester | Folic acid | Daily | - |
| Pregnant (2nd trimester onwards) + 6 months postpartum | IFA tablet | Daily | - |
Key Targets & Numbers
| Parameter | Value |
|---|---|
| Target anemia reduction | 3% per year |
| Period | 2018-2022 |
| Total beneficiaries targeted | ~450 million (≈50% of India's population) |
| Pregnant women target | Reduce from 50% → 32% by 2022 |
| WHO commitment | 50% reduction in anemia in WRA by 2025 |
| IFA given in Q2 FY 2024-25 | 15.4 crore children/adolescents |
Motto / Framework
TEST. TREAT. TALK. (+ TRACK in 2025 upgrade)
- TEST - Digital hemoglobinometer-based screening
- TREAT - IFA supplementation + referral for severe cases
- TALK - Counseling on iron-rich diet, vitamin C, compliance
- TRACK - Real-time monitoring via AMB dashboard (new T4 app, 2025)
Why It Matters (Burden of Disease)
- 67.1% children under 5 are anemic (NFHS-5)
- 59.1% adolescent girls are anemic
- 52.2% pregnant women are anemic
- IDA causes 1.18% GDP loss and is 3rd leading cause of DALYs in women aged 15-44
- Economic loss in South Asia: $4.2 billion/year
Recent Update (2025)
- New T4 Mobile App launched for real-time beneficiary tracking
- AMB Index published ranking all states/UTs by IFA coverage
- IFA coverage crossed 50% nationally for the first time (2022-23)
- Integrated with POSHAN Abhiyaan 2.0 and PM POSHAN (midday meal scheme)
This programme is a standard exam topic in Community Medicine / PSM for MBBS, MD, and nursing competitive exams in India.
This is a shared conversation. Sign in to Orris to start your own chat.