
d77a4da5-328f-4034-af01-2315a3a37572.jpeg
Give me answer to this and explain in appropriate way
analyse_media
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a complete, structured answer to all three questions.
Clinical Case: 40-year-old Female with Dyspepsia, Epigastric Pain, and Tarry Stools
Q1. Diagnosis
Chronic Peptic Ulcer Disease (most likely Duodenal Ulcer)
Clinical reasoning:
- Pain occurring 2-3 hours after meals and worse at night is the hallmark of duodenal ulcer (pain occurs when stomach empties and acid is unbuffered, relieved by food/antacids)
- Dyspepsia and epigastric pain fit PUD perfectly
- Tarry stools (melena) indicate upper GI bleeding - a classic complication of peptic ulcers
- A 40-year-old female is in the typical age group for PUD
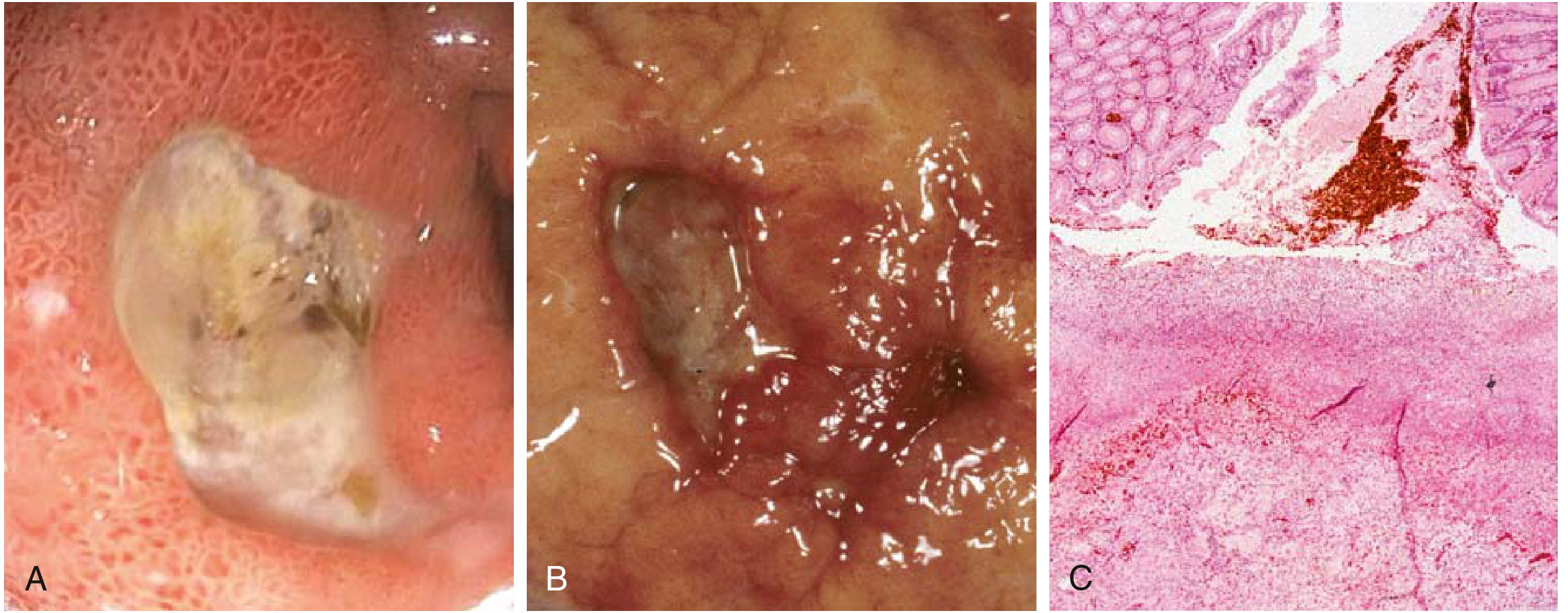
Q2. Microscopic Features Seen in the Image
The histological slide shows the 4-layer zonal architecture of a chronic peptic ulcer base (from surface/lumen down to deeper tissue):
| Zone | What You See |
|---|---|
| Zone 1 - Superficial Necrosis | Thin layer of eosinophilic amorphous debris + fibrinous exudate at the luminal surface |
| Zone 2 - Active Inflammation | Dense band of neutrophils (PMNs) indicating active tissue destruction |
| Zone 3 - Granulation Tissue | Proliferating capillaries (neovascularization), fibroblasts, and chronic inflammatory cells (lymphocytes, plasma cells, macrophages) |
| Zone 4 - Fibrosis/Cicatrization | Deep dense collagenous scar replacing the normal muscularis - the hallmark of chronicity |
Additional microscopic features:
- Complete breach of the mucosal epithelium extending through the muscularis mucosae
- Destruction of normal glandular architecture in the ulcer bed
- Endarteritis obliterans (thickened vessel walls) may be seen in deeper tissue
- Marginal regenerative epithelial changes at ulcer edges (hyperchromatic nuclei, mucin depletion - should not be confused with dysplasia)
As Robbins & Kumar describe: "The classic peptic ulcer is a round to oval, sharply punched-out defect. The ulcer base is smooth and clean as a result of peptic digestion of exudate and on histologic examination is composed of highly vascular granulation tissue." - Robbins & Kumar Basic Pathology, p. 556
Q3. Complications of Peptic Ulcer Disease
The four major complications are:
1. Hemorrhage (most common)
- Erosion into a submucosal blood vessel leads to bleeding
- Presents as melena (tarry stools) as seen in this patient - from upper GI bleeding
- Massive hemorrhage if a large vessel (e.g., gastroduodenal artery) is eroded
2. Perforation
- Ulcer erodes completely through the bowel wall
- Releases gastric contents into the peritoneal cavity
- Causes acute peritonitis - sudden severe diffuse abdominal pain ("board-like rigidity")
- X-ray shows free air under the diaphragm
3. Pyloric Obstruction / Gastric Outlet Obstruction
- Repeated ulceration and scarring of the pylorus/duodenum causes fibrosis and narrowing
- Presents with projectile vomiting of undigested food, succussion splash, weight loss
4. Penetration
- Ulcer erodes into an adjacent organ (pancreas, liver, biliary tract)
- Posterior duodenal ulcer penetrating the pancreas causes back pain and raised serum amylase/lipase
5. Malignant Transformation
- Gastric ulcers (NOT duodenal) carry a small risk of transformation into gastric adenocarcinoma
- Duodenal ulcers almost never become malignant
Key Teaching Points:
- This patient's melena = hemorrhage complication already present
- H. pylori infection and NSAID use are the two biggest causes of PUD
- Treatment: H. pylori eradication (triple therapy) + proton pump inhibitors (PPIs)
- Robbins notes: "Pain tends to occur 1 to 3 hours after meals during the day, is worse at night, and is relieved by alkali or food" - matching this patient exactly
This is a shared conversation. Sign in to Orris to start your own chat.