Cat Bite - microbiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cat bite" AND "microbiology" AND infection
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a comprehensive breakdown of the microbiology of cat bites:
Cat Bite - Microbiology
Why Cat Bites Are Especially Dangerous
Cat bites carry an infection rate >50% - far higher than dog bites. The reason is mechanical: cat canine teeth are narrow and sharp, functioning like a hypodermic needle. They create a small puncture that seals quickly at the skin surface, trapping bacteria deep in tissue where anaerobic conditions favor rapid proliferation. This also explains why cat bites over joints frequently lead to septic arthritis and osteomyelitis. - Rosen's Emergency Medicine, p. 801
Microorganisms
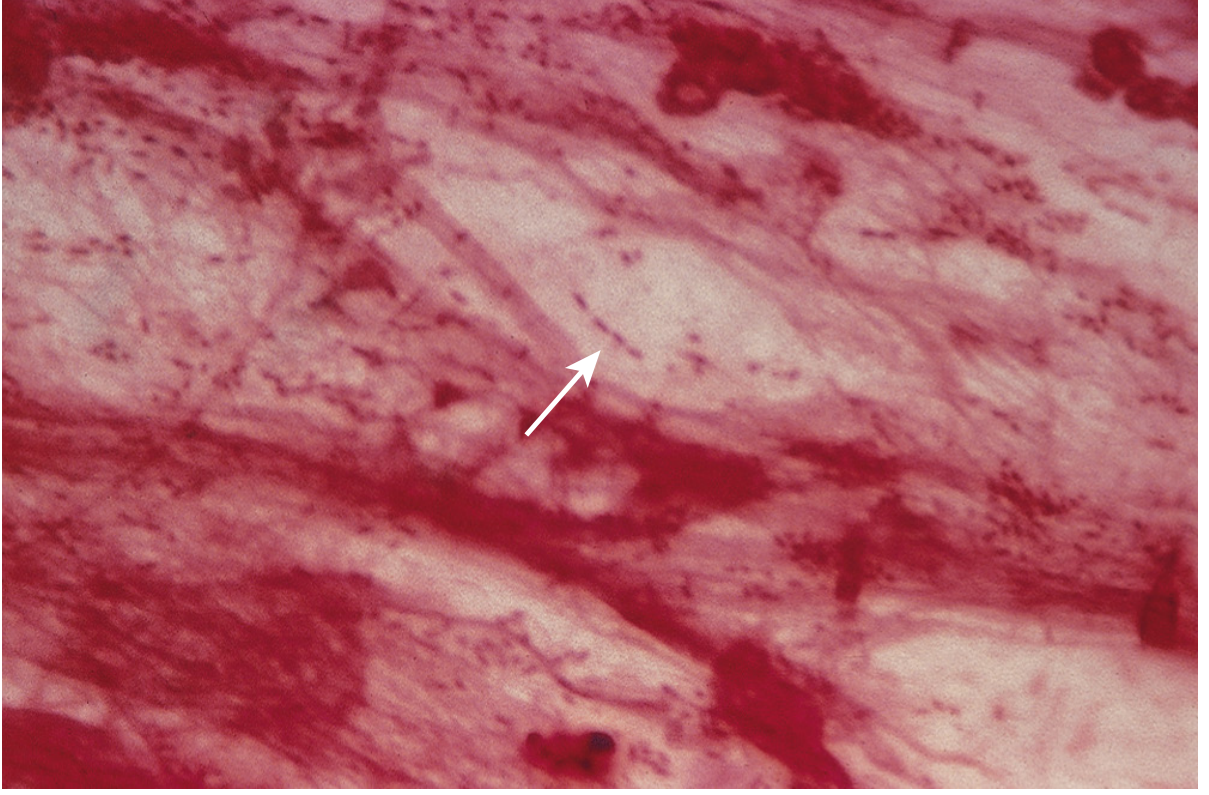
1. Pasteurella multocida - THE Key Pathogen
- Present in 70-75% of infected cat bite wounds - the dominant organism
- A normal commensal in the oropharynx of 70% of all cats
- Morphology: Small, gram-negative coccobacillus (facultatively anaerobic, fermentative)
- Gram stain: Shows bipolar staining ("safety pin" appearance)
- Culture characteristics:
- Grows well on blood agar and chocolate agar
- Grows poorly on MacConkey agar (key distinguishing feature)
- After overnight incubation: large, buttery colonies with a characteristic musty odor (due to indole production)
- Virulence factor: polysaccharide capsule composed of hyaluronic acid
- Clinical behavior: Infections advance rapidly - often within hours - causing severe inflammation, purulent drainage, and lymphadenitis
Medical Microbiology 9e, p. 291
Diseases caused by P. multocida:
| Disease Form | Context |
|---|---|
| Localized cellulitis + lymphadenitis | After animal bite/scratch |
| Osteomyelitis / Septic arthritis | Deep puncture near joints |
| Bacteremia / Septicemia | Immunocompromised hosts (especially liver disease) |
| Pneumonia | Exacerbation of chronic respiratory disease |
| Meningitis | Rare systemic spread |
2. Polymicrobial Flora (Mixed Aerobic + Anaerobic)
Cat bites are polymicrobial in >60% of cases. The full microbiological picture:
Aerobes / Facultative anaerobes:
| Organism | Notes |
|---|---|
| Pasteurella multocida | Most frequent; rapid onset |
| Pasteurella canis | Less common than P. multocida |
| Staphylococcus aureus | Present in many wounds |
| Streptococcus species | Alpha- and beta-hemolytic strains |
Anaerobes (present in ~40% of cat bite infections):
| Organism | Notes |
|---|---|
| Bacteroides species | Most common anaerobe |
| Fusobacterium species | Gram-negative rod |
| Porphyromonas species | Pigmented anaerobe |
| Prevotella species | Common oral anaerobe |
| Propionibacterium species | Gram-positive anaerobe |
Rosen's Emergency Medicine; Tietz Textbook of Laboratory Medicine
3. Special Pathogens - Late/Systemic Consequences
| Organism | Disease | Mechanism |
|---|---|---|
| Bartonella henselae | Cat-scratch disease (CSD) | Inoculation via scratch or bite; causes regional lymphadenopathy; bacillary angiomatosis in immunocompromised |
| Francisella tularensis | Tularemia | Cat bite/scratch transmission; causes ulceroglandular syndrome |
| Sporothrix schenckii | Sporotrichosis | Scratch or bite from cats; subcutaneous mycosis |
| Rabies virus | Rabies | Rare but must be considered; post-exposure prophylaxis if indicated |
| Clostridium tetani | Tetanus | Deep puncture wounds; tetanus prophylaxis needed |
Harrison's Principles of Internal Medicine 22E, p. 1187-1253
Clinical Infection Profile
- 90% of infected cat bites become symptomatic within 48 hours
- Pasteurella infections: onset within hours - a key clinical clue
- Wound breakdown by type:
- Cellulitis: 50%
- Tenosynovitis: 20%
- Osteomyelitis / Septic arthritis: 15%
- Abscess: 10%
Antibiotic Susceptibility of P. multocida
| Antibiotic Class | Activity |
|---|---|
| Penicillin G, Ampicillin | Drug of choice - highly susceptible |
| Amoxicillin-clavulanate | Recommended for cat bites (covers polymicrobial flora too) |
| Expanded-spectrum cephalosporins | Acceptable alternative |
| Macrolides, Tetracyclines, Fluoroquinolones | Acceptable alternatives |
| Semisynthetic penicillins (oxacillin, dicloxacillin) | Poor activity - do NOT use |
| First-generation cephalosporins (cephalexin) | Poor activity - do NOT use |
| Clindamycin | Resistant - do NOT use |
| Aminoglycosides | Poor activity |
Key point: P. multocida is resistant to penicillinase-resistant penicillins and first-generation cephalosporins - drugs that are commonly used for skin infections. This is why amoxicillin-clavulanate is specifically required, not just any beta-lactam. - Goodman & Gilman's Pharmacological Basis of Therapeutics
High-Risk Groups for Systemic Infection
- Age >50
- Diabetes mellitus
- Liver disease / alcoholism
- Immunosuppression (corticosteroids, HIV)
- Chronic renal insufficiency
- Peripheral vascular disease
Rosen's Emergency Medicine, Table 52.2
Sources: Harrison's Principles of Internal Medicine 22E | Medical Microbiology 9e | Rosen's Emergency Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics | Tietz Textbook of Laboratory Medicine 7e
Rate
I'd give the previous response a 8.5/10.
What worked well:
- Parallel tool calls kept it efficient
- Pulled from 5+ authoritative textbooks simultaneously
- Included the actual microscopy image of P. multocida
- Tables made the polymicrobial flora, susceptibility, and clinical data scannable
- Covered the full spectrum - immediate wound flora, late consequences, and systemic risks
- The antibiotic resistance point (first-gen cephalosporins fail) is a high-yield clinical pearl that's easy to miss
What could have been better:
- The Bartonella henselae section could have gone deeper - inoculation papule, incubation period, lymphadenopathy timeline, Warthin-Starry stain, distinction between immunocompetent vs. immunocompromised presentation
- Could have included a summary mnemonic or high-yield exam table at the end
- Tularemia and sporotrichosis were listed but not elaborated - a student might want more on those
- No explicit mention of Capnocytophaga canimorsus (more dog than cat, but relevant in bite wound context)
- The "one-third are aerobic only" stat from Rosen's was buried and deserved highlighting
Want me to expand on any specific organism or clinical aspect?
Rat Bite infection
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
All the information needed is in hand. Here is the full breakdown:
Rat Bite - Microbiology
Overview
Rat bites are low-risk for local wound infection (rodent saliva carries sparse flora), but carry a unique systemic risk - Rat Bite Fever (RBF), a bacteremic febrile illness that is distinct from ordinary wound infections. The local bite site often heals completely before systemic disease manifests - a classic and clinically important feature.
The Two Causative Organisms of Rat Bite Fever
| Feature | Streptobacillus moniliformis | Spirillum minus |
|---|---|---|
| Disease name | Streptobacillary RBF / Haverhill fever | Spirillary RBF / Sodoku |
| Geography | Worldwide; predominant in Americas & Europe | Almost exclusively East Asia (Japan = "sodoku") |
| Reservoir | Nasopharynx of rats; also cats, dogs, other predators | Rat blood and tissues |
| Gram stain morphology | Gram-negative pleomorphic rod | Gram-negative spirochete (spiral, 2-5 coils) |
| Incubation period | 3-10 days (short) | 1-4 weeks (long) |
| Bite site at presentation | Usually healed - no local signs | Usually tender, indurated, ulcerated or eschar |
| Arthritis | Prominent - migratory polyarthritis (60%) | Rare (~20%) |
| Rash distribution | Palms, soles, around joints - peripherally prominent | Abdomen-prominent, resembles typhoid rose spots |
| Lymphadenopathy | Minimal | Prominent regional lymphadenopathy + lymphangitis |
| False-positive VDRL | ~1/3 of cases | Present |
| Culture | Possible (fastidious) | Cannot be cultured in vitro |
| Diagnosis | Blood culture + joint fluid culture | Darkfield microscopy of blood; animal inoculation |
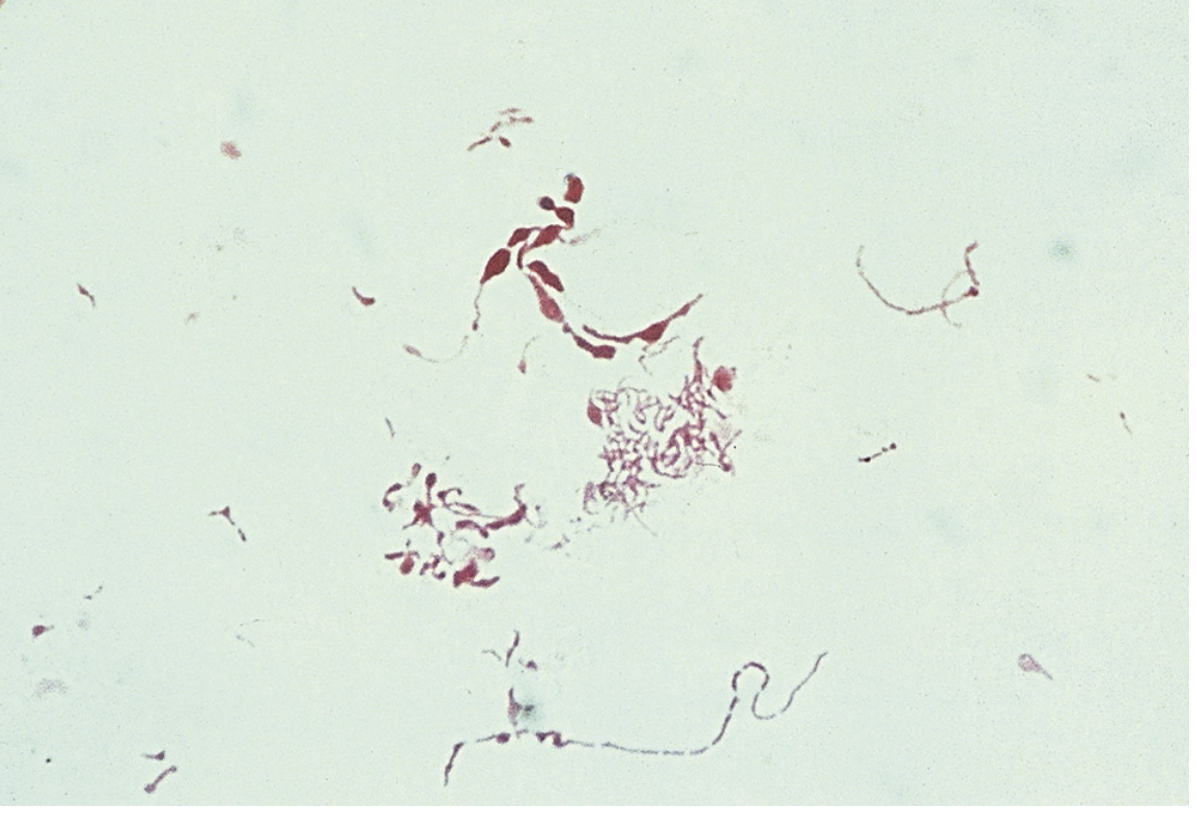
Streptobacillus moniliformis - Detailed Microbiology
Morphology (Gram stain):
- Long, thin gram-negative rod (0.1-0.5 × 1-5 μm)
- Stains poorly and is highly pleomorphic
- Characteristic bulbous swellings ("string of beads" appearance - hence moniliformis = necklace-shaped)
- Extremely long filaments (up to 150 μm) with fusiform swellings and large round bodies in older cultures
- Name origin: Latin monile = necklace
Culture characteristics (critical for lab):
- Fastidious - requires enriched media
- Media must be supplemented with: 15% blood, 20% horse/calf serum, or 5% ascitic fluid
- IMPORTANT: Growth is inhibited by sodium polyanethol sulfonate (SPS) - the anticoagulant present in most commercial blood culture bottles. Lab must be informed to use SPS-free bottles
- Broth growth: characteristic "puffball" colonies (or "bread crumb" clumps)
- Agar colonies: small, round; cell-wall-defective L-form variants grow as "fried egg" colonies (heaped center with spreading edges)
- Slow growth: minimum 3 days to isolate
- Identification: biochemically relatively inert; most reliable method is 16S rRNA gene sequencing
- Microaerophilic
Medical Microbiology 9e, p. 346; Harrison's 22E
Spirillum minus - Detailed Microbiology
- Gram-negative spirochete with 2-5 tight coils
- Cannot be cultured in vitro - key distinguishing feature
- Diagnosis by: darkfield microscopy of blood/exudate, or animal inoculation (mice/guinea pigs)
- Serology: false-positive VDRL (syphilis test) common
Clinical Disease - Streptobacillary RBF
Pathophysiology: Rat bite → bacteria enter bloodstream → bacteremia → systemic seeding
Classic triad:
- Irregular fever (relapsing pattern), chills, headache, myalgia
- Migratory polyarthralgia / polyarthritis - large joints, asymmetric, resembles rheumatoid arthritis but rarely suppurative; can involve liver, kidneys, meninges, heart valves
- Maculopapular or petechial rash - palms, soles, acral - appears 2-3 days after fever onset
Important clinical points:
- Bite site heals before systemic illness - patients may not recall the bite
- Rash can show desquamation of palms and soles ~1 week after resolution (mimics Kawasaki disease)
- Hemorrhagic acral vesicles can resemble leukocytoclastic vasculitis or gonococcemia
- Untreated mortality: ~10%
Haverhill Fever = same organism (S. moniliformis) acquired by ingestion of rat-contaminated food/water (not bite) - classically milk. Presents with pharyngitis + vomiting in addition to usual RBF features.
Other Pathogens Transmissible via Rat Bite
| Pathogen | Disease |
|---|---|
| Leptospira species | Leptospirosis (via urine-contaminated water/soil) |
| Francisella tularensis | Tularemia |
| Yersinia pestis | Plague (typically via flea vector, not direct bite) |
| Sporothrix schenckii | Sporotrichosis |
| Murine typhus (Rickettsia typhi) | Via rat flea |
| Hantavirus | Via inhalation of excreta, rarely direct contact |
Rosen's Emergency Medicine; Park's Preventive and Social Medicine
Differential Diagnosis of RBF
- Rocky Mountain Spotted Fever
- Lyme disease
- Meningococcemia / Disseminated gonococcemia
- Secondary syphilis
- Leptospirosis
- Acute rheumatoid arthritis / Acute rheumatic fever
- Endocarditis
- Viral exanthems (Coxsackievirus)
- Ehrlichiosis/Rickettsioses
- Pasteurella multocida infection
Treatment
| Situation | Drug of Choice | Alternative |
|---|---|---|
| Empirical (bite, pre-ID) | Amoxicillin-clavulanate | Doxycycline |
| S. moniliformis confirmed | Penicillin G (IV) or amoxicillin (oral) | Tetracycline |
| Penicillin allergy | Doxycycline | Streptomycin |
| Note | Penicillin NOT active against L-form (cell wall-defective) variants |
- Tetanus immunization status must be checked
- Always cleanse wound promptly and thoroughly
- Rat bites: low risk for classic wound infection; main concern is systemic RBF
Fitzpatrick's Dermatology; Medical Microbiology 9e; Harrison's Principles of Internal Medicine 22E
Sources: Harrison's Principles of Internal Medicine 22E | Medical Microbiology 9e | Fitzpatrick's Dermatology | Dermatology 2-Volume Set 5e | Rosen's Emergency Medicine | Jawetz Melnick & Adelberg's Medical Microbiology 28E
This is a shared conversation. Sign in to Orris to start your own chat.