Acid base disorder not able to understand
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have more than enough content from authoritative textbooks to write a thorough, clear explanation. Let me compose the complete answer.
Acid-Base Disorders - A Complete Breakdown
The Big Picture First
The body keeps blood pH tightly between 7.35 - 7.45. Two systems control this:
- Kidneys - regulate bicarbonate (HCO₃⁻) - slower, takes 2-5 days
- Lungs - regulate CO₂ - faster, acts within 12-24 hours
The Henderson-Hasselbalch equation ties it all together:
pH = pK + log ([HCO₃⁻] / [0.03 × PaCO₂])
When one system fails, the other compensates to pull pH back toward normal - but never completely to normal, and never past normal.
The 4 Primary Disorders
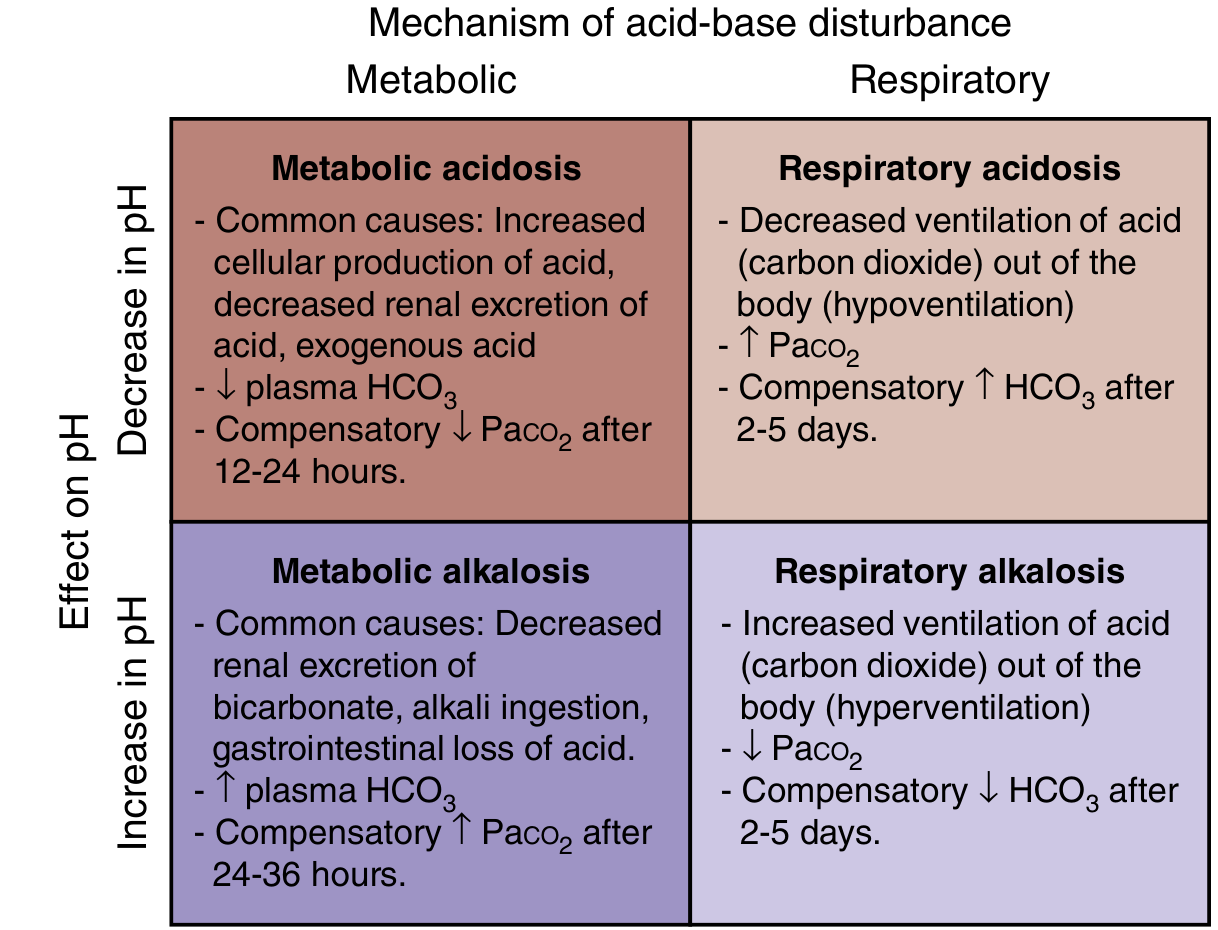
1. Metabolic Acidosis
Definition: Low pH + Low HCO₃⁻ (kidneys losing or not retaining base)
Compensation: Lungs blow off CO₂ (hyperventilation) - kicks in within 12-24 hours
Formula: Expected PaCO₂ = (1.5 × HCO₃⁻) + 8 ± 2 (Winters' formula), or simply: ΔPaCO₂ = ΔHCO₃⁻ × 1.2
Key Step - Calculate the Anion Gap:
AG = Na⁺ - (Cl⁻ + HCO₃⁻) | Normal = ~12 mEq/L
| Type | Anion Gap | Pathology |
|---|---|---|
| High AG (>15) | Elevated | Unmeasured anions accumulate |
| Normal AG (hyperchloremic) | Normal | HCO₃⁻ lost, Cl⁻ rises to compensate |
Causes of High AG Metabolic Acidosis - Mnemonic "MUDPILES":
- M - Methanol
- U - Uremia
- D - DKA (Diabetic ketoacidosis)
- P - Paraldehyde / Paracetamol (acetaminophen)
- I - Iron / Isoniazid
- L - Lactic acidosis
- E - Ethylene glycol
- S - Salicylates
Causes of Normal AG Metabolic Acidosis - Mnemonic "HARDUP":
- H - Hyperalimentation / Hospital saline
- A - Acid infusion / Addison's disease / Acetazolamide
- R - Renal tubular acidosis (RTA)
- D - Diarrhea (loses HCO₃⁻)
- U - Ureterosigmoidostomy
- P - Pancreatic fistula/drainage
2. Metabolic Alkalosis
Definition: High pH + High HCO₃⁻ (acid lost or base gained)
Compensation: Lungs retain CO₂ (hypoventilation) - takes 24-36 hours
Formula: ΔPaCO₂ = ΔHCO₃⁻ × 0.7 (PaCO₂ rarely rises above 60 mmHg even with very high HCO₃⁻)
Common Causes:
- Vomiting / NG tube suction (loss of HCl)
- Diuretic use (loop/thiazide - lose Cl⁻, K⁺)
- Hyperaldosteronism
- Alkali ingestion (antacid overuse)
- Post-hypercapnic state
Important: Metabolic alkalosis is associated with volume depletion and hypokalemia. GI-based chloride losses respond to IV normal saline. Mineralocorticoid-driven cases do not respond to saline (called "chloride-resistant").
3. Respiratory Acidosis
Definition: Low pH + High PaCO₂ (CO₂ not cleared = hypoventilation)
Compensation: Kidneys retain HCO₃⁻
| Timing | Formula |
|---|---|
| Acute | ΔHCO₃⁻ = ΔPaCO₂ × 0.1 (rises ~1 mEq/L per 10 mmHg CO₂ rise) |
| Chronic | ΔHCO₃⁻ = ΔPaCO₂ × 0.4 (rises ~3.5 mEq/L per 10 mmHg CO₂ rise) |
Common Causes:
- COPD / severe asthma (lung disease)
- Opioid/sedative overdose (reduced respiratory drive)
- Neuromuscular disease (ALS, Guillain-Barre, myasthenia)
- Chest wall deformity (obesity hypoventilation, kyphoscoliosis)
- Central sleep apnea
4. Respiratory Alkalosis
Definition: High pH + Low PaCO₂ (hyperventilation = too much CO₂ blown off)
Compensation: Kidneys excrete HCO₃⁻ (most effective compensator - pH can sometimes return to normal)
| Timing | Formula |
|---|---|
| Acute | ΔHCO₃⁻ = ΔPaCO₂ × 0.2 |
| Chronic | ΔHCO₃⁻ = ΔPaCO₂ × 0.5 |
Common Causes:
- Anxiety / panic attack (most common)
- Pain
- Pregnancy (progesterone stimulates respiration)
- High altitude
- Pulmonary embolism
- Salicylate toxicity (early - directly stimulates respiratory center)
- Sepsis (early)
- Liver failure
Step-by-Step ABG Interpretation (5-Step Approach)
Given: pH, PaCO₂, HCO₃⁻ (from basic metabolic panel + blood gas)
Step 1: Check the pH
- pH < 7.35 → Acidemia
- pH > 7.45 → Alkalemia
- pH 7.35-7.45 → Normal (but a mixed disorder may still exist!)
Step 2: Identify the primary disorder
| pH | Primary Change | Disorder |
|---|---|---|
| Low pH | Low HCO₃⁻ | Metabolic acidosis |
| Low pH | High PaCO₂ | Respiratory acidosis |
| High pH | High HCO₃⁻ | Metabolic alkalosis |
| High pH | Low PaCO₂ | Respiratory alkalosis |
Step 3: Check for appropriate compensation
Use the formulas above. If compensation is MORE or LESS than expected, a second primary disorder is present (mixed disorder).
Step 4: Calculate Anion Gap (if metabolic acidosis)
AG = Na⁺ - (Cl⁻ + HCO₃⁻). Normal = ~12.
Step 5: If high AG - calculate the Delta-Delta (Delta Gap)
Used to detect a hidden concurrent metabolic alkalosis or normal-AG acidosis:
Delta Gap = (Measured AG - 12) - (24 - Measured HCO₃⁻)
- Delta gap > +6 → Concurrent metabolic alkalosis hiding behind the AG acidosis
- Delta gap < -6 → Concurrent normal-AG acidosis also present
Compensation Formulas - Quick Reference Table
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO₂ = ΔHCO₃⁻ × 1.2 |
| Metabolic alkalosis | PaCO₂ = ΔHCO₃⁻ × 0.7 (max ~60 mmHg) |
| Acute resp. acidosis | HCO₃⁻ = ΔPaCO₂ × 0.1 |
| Chronic resp. acidosis | HCO₃⁻ = ΔPaCO₂ × 0.4 |
| Acute resp. alkalosis | HCO₃⁻ = ΔPaCO₂ × 0.2 |
| Chronic resp. alkalosis | HCO₃⁻ = ΔPaCO₂ × 0.5 |
Worked Example
ABG: pH = 7.28, PaCO₂ = 20, HCO₃⁻ = 9, Na = 140, Cl = 105
Step 1: pH 7.28 → Acidemia
Step 2: Low HCO₃⁻ → Primary metabolic acidosis
Step 3: Expected PaCO₂ = 1.5 × 9 + 8 = 21.5 ± 2. Measured = 20 ✓ Appropriate compensation (simple metabolic acidosis)
Step 4: AG = 140 - (105 + 9) = 26 → High AG metabolic acidosis
Step 5: Delta gap = (26 - 12) - (24 - 9) = 14 - 15 = -1 → No additional hidden disorder. Pure high-AG metabolic acidosis.
Think: MUDPILES. Lactic acidosis? DKA? Renal failure?
Simple Memory Framework
| disorder | pH | Primary change | Compensation |
|---|---|---|---|
| Metabolic acidosis | ↓ | ↓ HCO₃⁻ | ↓ PaCO₂ (hyperventilate) |
| Metabolic alkalosis | ↑ | ↑ HCO₃⁻ | ↑ PaCO₂ (hypoventilate) |
| Respiratory acidosis | ↓ | ↑ PaCO₂ | ↑ HCO₃⁻ (kidneys retain) |
| Respiratory alkalosis | ↑ | ↓ PaCO₂ | ↓ HCO₃⁻ (kidneys excrete) |
Key rule: In compensation, PaCO₂ and HCO₃⁻ always move in the same direction. If they move in opposite directions, you are looking at a mixed disorder - guaranteed.
Sources: Rosen's Emergency Medicine (9th ed.), Henry's Clinical Diagnosis and Management by Laboratory Methods, Barash Clinical Anesthesia (9th ed.), Comprehensive Clinical Nephrology (7th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.