Tell me about the anotomy and physiology of heart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Anatomy and Physiology of the Heart
1. Gross Anatomy
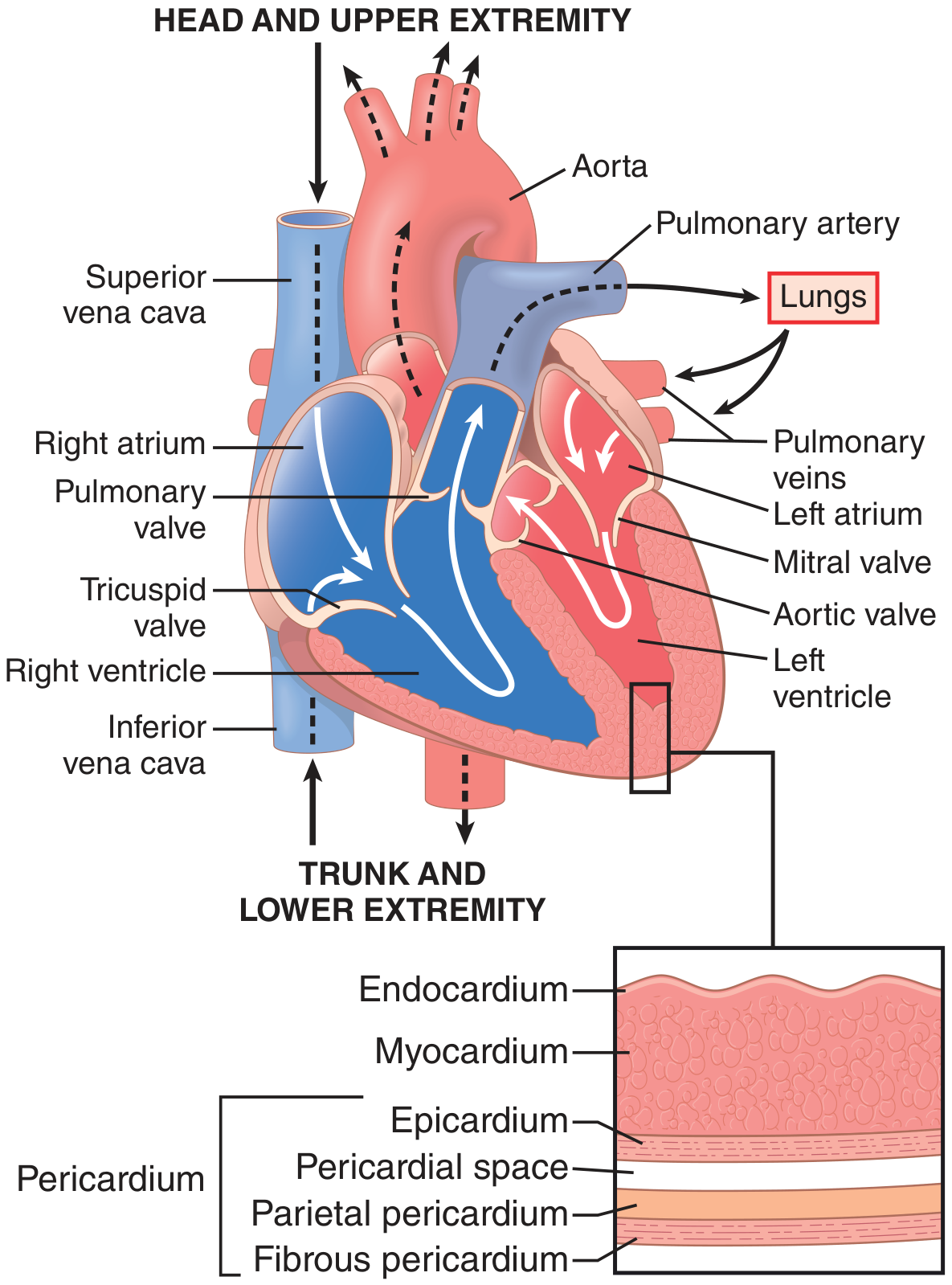
The heart is a phasic, electrically self-actuated, variable-speed hydraulic pump composed of two dual-component elastic muscular chambers (the right and left sides), each with an atrium and a ventricle. It is enclosed within the pericardium, which has three layers:
- Fibrous pericardium - tough outer layer
- Parietal pericardium - inner serous layer
- Pericardial space - contains a thin film of fluid for lubrication
The heart wall itself consists of three layers:
| Layer | Description |
|---|---|
| Endocardium | Smooth inner lining; in contact with blood |
| Myocardium | The thick muscular layer; responsible for contraction |
| Epicardium | Outermost layer of the heart wall (visceral pericardium) |
Chambers
| Chamber | Wall Thickness | Function |
|---|---|---|
| Right atrium | Thin | Receives deoxygenated blood from SVC and IVC |
| Right ventricle | Thin | Pumps to pulmonary circulation |
| Left atrium | Thin | Receives oxygenated blood from pulmonary veins |
| Left ventricle | Thick | Pumps to systemic circulation at high pressure |
The thick-walled left ventricle is the primary pumping chamber, composed of billions of cardiomyocytes connected end to end through gap junctions. The thinner right ventricle is divided from the left by the interventricular septum.
- Goldman-Cecil Medicine, p. 412
2. Valves
The heart has four valves that ensure unidirectional blood flow:
Atrioventricular (AV) Valves - separate atria from ventricles:
- Tricuspid valve (right side, 3 leaflets) - opens on pressure gradient from right atrium to right ventricle
- Mitral valve / Bicuspid valve (left side, 2 leaflets) - separates left atrium from left ventricle
Both AV valves are attached to chordae tendineae anchored to papillary muscles projecting from the ventricular walls. The papillary muscles position the valve leaflets and prevent regurgitation during contraction.
Semilunar Valves - separate ventricles from great vessels:
-
Pulmonary valve - right ventricle to pulmonary artery
-
Aortic valve - left ventricle to aorta
-
Goldman-Cecil Medicine, p. 412
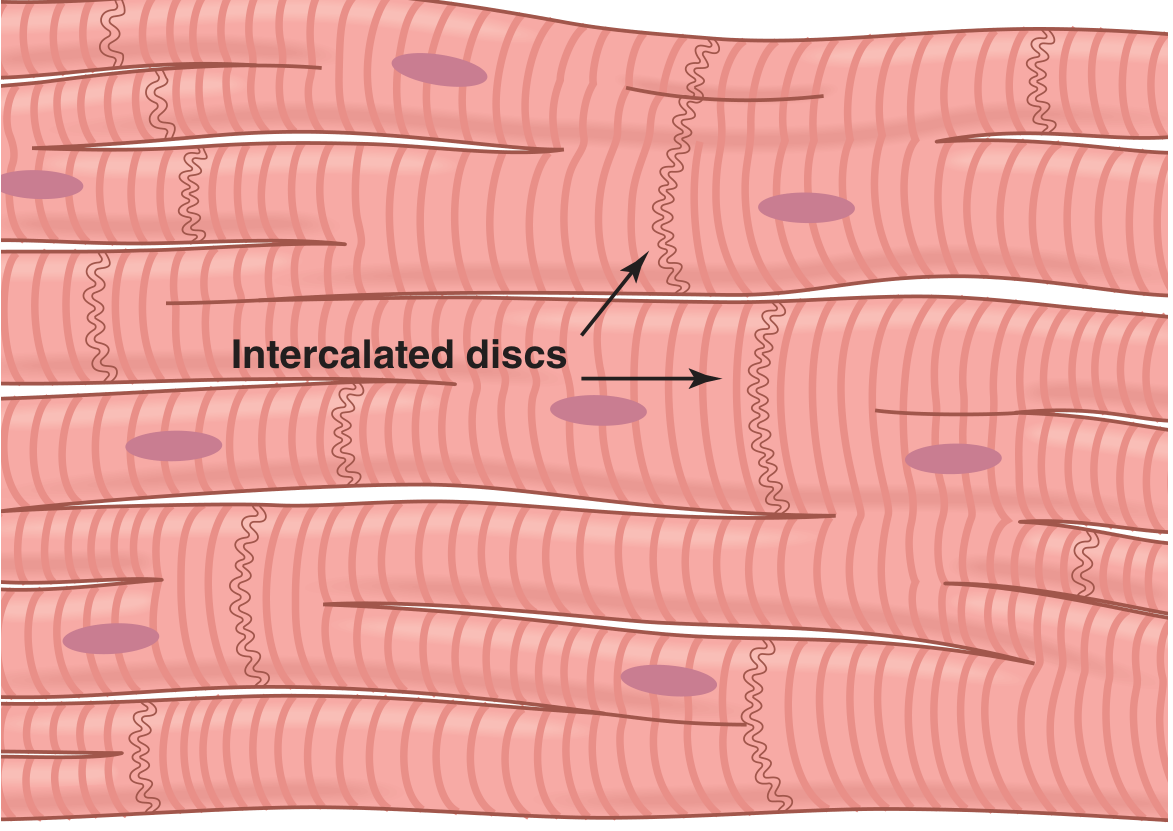
3. Cardiac Muscle Histology (Microanatomy)
The heart is composed of three major types of cardiac muscle:
- Atrial muscle - contracts to prime the ventricles
- Ventricular muscle - generates high-pressure contraction
- Specialized excitatory and conductive fibers - generate and propagate action potentials (few contractile fibrils)
Key histological features:
- Cardiac muscle is striated, like skeletal muscle, with actin and myosin filaments
- Cells are connected by intercalated discs containing gap junctions that allow rapid ionic diffusion
- This makes cardiac muscle a functional syncytium - when one cell is excited, the action potential rapidly spreads to all connected cells
- There are actually two syncytia: the atrial syncytium and the ventricular syncytium, separated by the fibrous AV ring (impulses cross only via the AV node/bundle)
Left Ventricular Fiber Arrangement (Torsion):
The LV has a complex double-helix fiber arrangement. The subepicardial fibers spiral leftward and the subendocardial fibers spiral rightward. During contraction, the apex rotates counterclockwise and the base rotates clockwise (viewed from apex), producing a wringing/twisting motion that optimizes ejection. At end-systole, the ventricle acts like a loaded spring and recoils (untwists) during diastole, aiding rapid filling.
- Guyton and Hall, Textbook of Medical Physiology, p. 122-126
4. Cardiac Conduction System
The cardiac conduction system initiates and coordinates contraction in a precise unidirectional sequence:
SA Node → Atrial muscle → AV Node → AV Bundle (Bundle of His)
→ Right & Left Bundle Branches → Purkinje Fibers → Ventricular muscle
| Component | Location | Role |
|---|---|---|
| SA Node (pacemaker) | Superior crista terminalis, junction of SVC and right atrium | Generates impulse (~60-100/min); "pacemaker of the heart" |
| AV Node | Near coronary sinus opening, attachment of tricuspid valve septal cusp | Delays impulse >0.1 sec to allow atrial contraction before ventricular filling |
| AV Bundle (Bundle of His) | Along lower border of membranous interventricular septum | Conducts impulse from AV node to bundle branches |
| Right & Left Bundle Branches | Along respective sides of interventricular septum toward apex | Rapidly distribute impulse to ventricular walls |
| Purkinje Fibers | Subendocardial plexus | Final rapid distribution to all ventricular myocardium |
The AV delay (>0.1 second) is physiologically important - it allows the atria to contract first, pumping blood into the ventricles before ventricular contraction begins. Conduction fibers are insulated by connective tissue along their course to prevent inappropriate stimulation, with the greatest number of functional contacts appearing at the subendocardial level.
The wave of excitation and contraction moves from the papillary muscles and apex toward the arterial outflow tracts - this bottom-to-top sequence squeezes blood upward out through the aortic and pulmonary valves.
- Gray's Anatomy for Students, p. 6364-6412
5. Coronary Blood Flow
The coronary arteries arise from the aorta just above the aortic valve and travel through the epicardium. Key points:
-
Diastolic aortic pressure drives most coronary flow (the heart is relaxed and coronary vessels are not compressed)
-
During systole, coronary flow to the endocardium is reduced because intramyocardial pressure compresses vessels; the endocardium is supplied predominantly during diastole
-
The epicardium receives flow during both systole and diastole
-
Metabolic regulators that increase coronary flow (up to 6-fold): nitric oxide, adenosine, bradykinins, prostaglandins, and carbon dioxide
-
The LV extracts oxygen near-maximally at baseline; therefore any increase in demand (exercise, tachycardia, increased afterload) must be met by proportional increases in coronary flow
-
Goldman-Cecil Medicine, p. 412; Barash Clinical Anesthesia, p. 840
6. The Cardiac Cycle
The cardiac cycle is a coordinated, temporally related series of electrical, mechanical, and valvular events from the beginning of one heartbeat to the beginning of the next.
At a heart rate of 72 beats/min, one cardiac cycle lasts ~0.833 seconds.
Phases
Systole (contraction, ~0.3 sec at 72 bpm):
- Isovolumic contraction - all valves closed; ventricular pressure rises rapidly
- Rapid ejection - aortic/pulmonary valves open when ventricular pressure exceeds arterial pressure; blood is ejected
- Reduced ejection - flow slows as pressure gradients equalize
Diastole (relaxation, ~0.5 sec at 72 bpm):
- Isovolumic relaxation - all valves closed; ventricular pressure falls rapidly
- Rapid ventricular filling - mitral/tricuspid valves open; 70-80% of filling occurs passively
- Slow filling (diastasis) - minimal additional filling
- Atrial kick - atrial contraction contributes the remaining ~20-30% of ventricular filling
The atria serve three mechanical roles: conduit (passive flow), reservoir (collecting pulmonary/systemic venous return), and contractile chamber (booster pump).
As heart rate increases, cycle duration shortens - diastole shortens proportionally more than systole. At very high rates (e.g., tachyarrhythmias), diastolic filling time is inadequate, reducing stroke volume and cardiac output.
- Guyton and Hall, Textbook of Medical Physiology, p. 126
7. Excitation-Contraction Coupling
The molecular mechanism linking electrical excitation to mechanical contraction:
- Action potential depolarizes the cell membrane
- L-type Ca²⁺ channels (LTCC) in the T-tubule membrane open → small Ca²⁺ influx
- This triggers ryanodine receptors (RyR2) on the sarcoplasmic reticulum (SR) → massive Ca²⁺ release ("calcium-induced calcium release")
- Ca²⁺ binds troponin C → conformational change in tropomyosin → exposes actin-binding sites
- Myosin heads attach to actin → cross-bridge cycling → contraction (sarcomere shortens)
Relaxation:
- Ca²⁺ is pumped back into the SR by SERCA2 (Ca²⁺-ATPase)
- Ca²⁺ is also extruded from the cell by the sodium-calcium exchanger (NCX)
- Tropomyosin re-covers the actin binding sites → relaxation
Key difference from skeletal muscle: cardiac muscle contraction depends heavily on extracellular Ca²⁺ (via T-tubules), while skeletal muscle relies almost entirely on intracellular SR stores. This is why hypocalcemia can impair cardiac contractility.
- Goldman-Cecil Medicine, p. 412 (Sarcomere and excitation-contraction coupling figure)
8. Determinants of Cardiac Performance
| Determinant | Definition | Clinical Relevance |
|---|---|---|
| Preload | Volume of blood in the ventricle just before contraction (end-diastolic volume) | Increased by fluid overload; reduced in hypovolemia |
| Afterload | Resistance the ventricle faces during ejection (systemic vascular resistance / aortic pressure) | Increased in hypertension; reduced by vasodilators |
| Contractility (inotropy) | Intrinsic force of contraction, independent of loading | Increased by catecholamines; decreased in heart failure |
| Heart Rate | Beats per minute | Too slow or too fast reduces cardiac output |
Cardiac Output (CO) = Stroke Volume × Heart Rate
Stroke Volume is determined by preload (Frank-Starling mechanism), afterload, and contractility.
Frank-Starling Law: As end-diastolic volume (preload) increases, stretch of myofilaments increases sensitivity of troponin C to Ca²⁺ → greater force of contraction and larger stroke volume.
- Barash Clinical Anesthesia, p. 840-841
Summary
The heart is a dual pump that circulates blood through the pulmonary and systemic circulations. Its anatomy (four chambers, four valves, specialized conduction system, coronary circulation) is precisely engineered to support its function. Cardiac physiology integrates electrical automaticity (SA node), rapid conduction (AV bundle/Purkinje network), excitation-contraction coupling (Ca²⁺-mediated), and the cardiac cycle (systole/diastole) to maintain continuous, effective blood flow. Performance is tuned moment to moment by preload, afterload, contractility, and heart rate.
Sources: Guyton and Hall Textbook of Medical Physiology; Goldman-Cecil Medicine; Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e; Gray's Anatomy for Students
Give the drug classification to remember from kd Tripathi
Reading File
Finding Sources
Finding Sources
KD Tripathi is not in the library. I'll answer comprehensively from my training knowledge of KD Tripathi's book, which I know well. This is one of the most well-known Indian pharmacology textbooks with very specific and memorable drug classifications.
Drug Classifications from KD Tripathi's Essentials of Medical Pharmacology
KD Tripathi is famous for his concise, exam-oriented classifications. Below are the major drug classifications as presented in his textbook, organized system-wise.
AUTONOMIC NERVOUS SYSTEM
Cholinergic Drugs (Parasympathomimetics)
A. Directly Acting:
- Choline esters: Acetylcholine, Methacholine, Carbachol, Bethanechol
- Alkaloids: Muscarine, Pilocarpine, Arecoline
B. Indirectly Acting (Anticholinesterases):
- Reversible: Physostigmine, Neostigmine, Pyridostigmine, Edrophonium, Rivastigmine, Donepezil
- Irreversible (organophosphates): DFP, Echothiophate, Parathion, Malathion, Tabun, Sarin
Anticholinergic Drugs
- Atropine, Hyoscine (Scopolamine), Homatropine, Tropicamide
- Quaternary: Ipratropium, Glycopyrrolate, Propantheline
Adrenergic Drugs
A. Directly Acting:
- α + β: Adrenaline (Epinephrine), Noradrenaline, Dopamine
- Predominantly α: Phenylephrine, Methoxamine, Xylometazoline, Clonidine
- Predominantly β: Isoprenaline, Salbutamol, Terbutaline, Salmeterol, Dobutamine
B. Indirectly Acting: Amphetamine, Tyramine, Hydroxyamphetamine
C. Mixed Acting: Ephedrine, Metaraminol
Adrenergic Antagonists
α-Blockers:
- Non-selective: Phentolamine, Phenoxybenzamine
- Selective α1: Prazosin, Terazosin, Doxazosin, Tamsulosin
β-Blockers:
- Non-selective: Propranolol, Sotalol, Timolol, Nadolol, Carvedilol (α+β)
- Cardioselective (β1): Metoprolol, Atenolol, Bisoprolol, Esmolol, Acebutolol
- ISA (Intrinsic Sympathomimetic Activity): Pindolol, Acebutolol, Oxprenolol
CARDIOVASCULAR DRUGS
Antihypertensives
A. Diuretics: Thiazides, Furosemide, Spironolactone
B. Sympatholytics:
- Central: Clonidine, Methyldopa
- Ganglion blockers: Trimethaphan
- Adrenergic neurone blockers: Reserpine, Guanethidine
- α-blockers, β-blockers (as above)
C. Vasodilators:
- Arteriolar: Hydralazine, Minoxidil, Diazoxide
- Arteriolar + venous: Sodium nitroprusside
D. ACE Inhibitors: Captopril, Enalapril, Lisinopril, Ramipril, Perindopril
E. ARBs (AT1 blockers): Losartan, Valsartan, Candesartan, Irbesartan
F. Calcium Channel Blockers:
- Phenylalkylamines: Verapamil
- Benzothiazepines: Diltiazem
- Dihydropyridines: Nifedipine, Amlodipine, Felodipine, Nimodipine
Antianginal Drugs
- Organic Nitrates: GTN (Glyceryl Trinitrate), Isosorbide dinitrate (ISDN), Isosorbide mononitrate (ISMN), Erythrityl tetranitrate
- β-blockers: Propranolol, Metoprolol, Atenolol
- Calcium Channel Blockers: Verapamil, Diltiazem, Nifedipine, Amlodipine
- Potassium Channel Openers: Nicorandil
- Others: Ranolazine, Trimetazidine
Antiarrhythmics (Vaughan-Williams Classification)
| Class | Mechanism | Drugs |
|---|---|---|
| IA | Na⁺ channel block (moderate) + K⁺ block | Quinidine, Procainamide, Disopyramide |
| IB | Na⁺ channel block (weak/fast off) | Lidocaine, Mexiletine, Phenytoin |
| IC | Na⁺ channel block (strong/slow off) | Flecainide, Propafenone |
| II | β-blockade | Propranolol, Metoprolol, Esmolol |
| III | K⁺ channel block (prolong repolarization) | Amiodarone, Sotalol, Ibutilide, Dofetilide |
| IV | Ca²⁺ channel block | Verapamil, Diltiazem |
| Unclassified | Various | Digoxin, Adenosine, Atropine, Magnesium |
Anticoagulants
A. Parenteral:
- Unfractionated heparin
- LMWHs: Enoxaparin, Dalteparin, Tinzaparin
- Factor Xa inhibitors: Fondaparinux
- Direct thrombin inhibitors: Lepirudin, Bivalirudin, Argatroban
B. Oral:
- Vitamin K antagonists: Warfarin, Acenocoumarol
- Direct Xa inhibitors (DOACs): Rivaroxaban, Apixaban, Edoxaban
- Direct thrombin inhibitors: Dabigatran
Fibrinolytics (Thrombolytics)
- 1st gen: Streptokinase, Urokinase
- 2nd gen (fibrin-specific): Alteplase (tPA), Reteplase, Tenecteplase
Antiplatelet Drugs
- COX inhibitors: Aspirin
- ADP (P2Y12) antagonists: Clopidogrel, Prasugrel, Ticagrelor, Ticlopidine
- GPIIb/IIIa inhibitors: Abciximab, Eptifibatide, Tirofiban
- PDE inhibitors: Dipyridamole, Cilostazol
- PAR-1 antagonists: Vorapaxar
Antihyperlipidemics (Hypolipidaemics)
- Statins (HMG-CoA reductase inhibitors): Lovastatin, Simvastatin, Atorvastatin, Rosuvastatin
- Fibrates (PPARα agonists): Gemfibrozil, Fenofibrate, Bezafibrate
- Bile acid sequestrants (resins): Cholestyramine, Colestipol
- Nicotinic acid (Niacin)
- Cholesterol absorption inhibitors: Ezetimibe
- PCSK9 inhibitors: Evolocumab, Alirocumab
CNS DRUGS
General Anaesthetics
A. Inhalational:
- Gases: Nitrous oxide, Cyclopropane
- Volatile liquids: Halothane, Enflurane, Isoflurane, Sevoflurane, Desflurane
B. Intravenous:
- Barbiturates: Thiopentone
- Benzodiazepines: Midazolam, Diazepam
- Opioids: Fentanyl, Morphine
- Others: Propofol, Ketamine, Etomidate
Sedative-Hypnotics
- Benzodiazepines: Diazepam, Alprazolam, Lorazepam, Triazolam, Nitrazepam
- Barbiturates: Phenobarbitone, Pentobarbitone
- Non-BZD-non-barbiturate: Zolpidem, Zaleplon, Eszopiclone, Zopiclone (Z-drugs)
- Others: Chloral hydrate, Buspirone (anxiolytic, not hypnotic)
Antiepileptics
- Older (classical): Phenobarbitone, Phenytoin, Carbamazepine, Valproate, Ethosuximide
- Newer: Lamotrigine, Topiramate, Levetiracetam, Gabapentin, Pregabalin, Oxcarbazepine, Lacosamide, Zonisamide
Antipsychotics (Neuroleptics)
Typical (1st Generation):
- Phenothiazines: Chlorpromazine, Fluphenazine, Trifluoperazine
- Butyrophenones: Haloperidol, Droperidol
- Thioxanthenes: Flupenthixol
Atypical (2nd Generation):
- Clozapine, Risperidone, Olanzapine, Quetiapine, Aripiprazole, Ziprasidone, Paliperidone
Antidepressants
- TCAs (Tricyclics): Imipramine, Amitriptyline, Clomipramine, Doxepin, Nortriptyline
- SSRIs: Fluoxetine, Paroxetine, Sertraline, Citalopram, Escitalopram, Fluvoxamine
- SNRIs: Venlafaxine, Desvenlafaxine, Duloxetine
- MAOIs: Phenelzine, Tranylcypromine, Moclobemide (reversible RIMA)
- Others: Mirtazapine (NaSSA), Bupropion (NDRI), Trazodone, Agomelatine
Opioid Analgesics
A. Strong (Morphine-like): Morphine, Pethidine (Meperidine), Fentanyl, Oxycodone, Methadone, Heroin
B. Moderate: Codeine, Tramadol, Pentazocine, Buprenorphine
C. Antagonists: Naloxone, Naltrexone
D. Mixed agonist-antagonists: Pentazocine, Buprenorphine, Nalbuphine
AUTACOIDS AND ANTI-INFLAMMATORY DRUGS
NSAIDs (Non-selective COX inhibitors)
- Salicylates: Aspirin
- Propionic acid derivatives: Ibuprofen, Naproxen, Ketoprofen
- Acetic acid derivatives: Indomethacin, Diclofenac, Ketorolac, Sulindac
- Enolic acid derivatives: Piroxicam, Meloxicam
- Fenamates: Mefenamic acid
- Pyrazolone derivatives: Phenylbutazone, Oxyphenbutazone
- Para-aminophenol derivatives: Paracetamol (Acetaminophen) - not a true NSAID
Selective COX-2 Inhibitors (Coxibs)
Celecoxib, Etoricoxib, Parecoxib, Rofecoxib (withdrawn)
Antihistamines
H1 Blockers:
- 1st gen (sedating): Diphenhydramine, Chlorpheniramine, Promethazine, Hydroxyzine
- 2nd gen (non-sedating): Loratadine, Cetirizine, Fexofenadine, Azelastine, Levocetirizine, Desloratadine
H2 Blockers: Cimetidine, Ranitidine, Famotidine, Nizatidine
Corticosteroids
- Short-acting: Hydrocortisone (Cortisol)
- Intermediate-acting: Prednisolone, Methylprednisolone, Triamcinolone
- Long-acting: Dexamethasone, Betamethasone
DMARDs (Disease-Modifying Antirheumatic Drugs)
- Non-biological (conventional): Methotrexate, Hydroxychloroquine, Sulfasalazine, Leflunomide, Gold salts, Penicillamine
- Biological DMARDs:
- Anti-TNF: Infliximab, Etanercept, Adalimumab
- Anti-IL-6: Tocilizumab
- Anti-CD20: Rituximab
- Anti-CD80/86: Abatacept
- Targeted synthetic: Tofacitinib (JAK inhibitor), Baricitinib
ANTIMICROBIAL DRUGS
Antibiotics - Cell Wall Synthesis Inhibitors
Penicillins:
- Natural: Penicillin G, Penicillin V
- Antistaphylococcal (penicillinase-resistant): Cloxacillin, Methicillin, Nafcillin
- Aminopenicillins (broad-spectrum): Ampicillin, Amoxicillin
- Antipseudomonal: Piperacillin, Ticarcillin
- β-lactamase inhibitor combinations: Amoxicillin-Clavulanate, Piperacillin-Tazobactam
Cephalosporins:
- 1st gen: Cephalexin, Cefazolin, Cephradine
- 2nd gen: Cefuroxime, Cefaclor, Cefoxitin
- 3rd gen: Ceftriaxone, Cefotaxime, Ceftazidime
- 4th gen: Cefepime
- 5th gen: Ceftaroline (anti-MRSA)
Carbapenems: Imipenem-Cilastatin, Meropenem, Doripenem, Ertapenem
Monobactams: Aztreonam
Glycopeptides: Vancomycin, Teicoplanin
Antibiotics - Protein Synthesis Inhibitors
| Site | Drugs |
|---|---|
| 30S ribosome | Aminoglycosides (Gentamicin, Amikacin, Tobramycin, Streptomycin), Tetracyclines, Tigecycline |
| 50S ribosome | Macrolides (Erythromycin, Azithromycin, Clarithromycin), Chloramphenicol, Clindamycin, Linezolid, Streptogramins |
Antibiotics - DNA/RNA Synthesis Inhibitors
- Fluoroquinolones: Ciprofloxacin, Ofloxacin, Levofloxacin, Moxifloxacin, Gemifloxacin
- Metronidazole, Tinidazole (anaerobes, protozoa)
- Rifampicin (RNA polymerase inhibitor)
Sulfonamides & Co-trimoxazole
- Sulfamethoxazole + Trimethoprim (Co-trimoxazole/Cotrimoxazole)
Antitubercular Drugs
First-line (RIPE):
- R - Rifampicin
- I - Isoniazid (INH)
- P - Pyrazinamide
- E - Ethambutol
- (S - Streptomycin)
Second-line: Kanamycin, Amikacin, Ethionamide, Cycloserine, PAS, Capreomycin
Newer: Bedaquiline, Linezolid, Delamanid
Antifungals
- Polyenes: Amphotericin B, Nystatin
- Azoles: Fluconazole, Itraconazole, Voriconazole, Posaconazole, Ketoconazole
- Echinocandins: Caspofungin, Micafungin, Anidulafungin
- Others: Flucytosine (5-FC), Griseofulvin, Terbinafine
Antivirals
Anti-Herpes: Acyclovir, Valacyclovir, Famciclovir, Ganciclovir, Valganciclovir
Anti-Influenza: Oseltamivir, Zanamivir, Baloxavir
Anti-HIV (ARTs):
- NRTIs: Zidovudine, Lamivudine, Tenofovir, Emtricitabine, Abacavir
- NNRTIs: Nevirapine, Efavirenz, Rilpivirine, Etravirine
- Protease inhibitors: Ritonavir, Lopinavir, Atazanavir, Darunavir
- Integrase inhibitors: Raltegravir, Elvitegravir, Dolutegravir, Bictegravir
- Fusion inhibitor: Enfuvirtide
- CCR5 antagonist: Maraviroc
Antimalarials
- Tissue schizonticides (causal prophylaxis/radical cure): Primaquine
- Blood schizonticides:
- Chloroquine-sensitive: Chloroquine, Quinine
- Artemisinin-based: Artesunate, Artemether, Arteether
- Others: Mefloquine, Halofantrine
- Both tissue + blood: Proguanil, Pyrimethamine
- Fixed dose combinations: Artemether+Lumefantrine (Coartem), AS+SP, AS+AQ
Antiprotozoals
- Amoebiasis: Metronidazole (tissue), Diloxanide furoate (luminal)
- Leishmaniasis: Sodium stibogluconate, Amphotericin B, Miltefosine
- Giardiasis: Metronidazole, Tinidazole
- Trypanosomiasis: Pentamidine, Melarsoprol, Suramin
ENDOCRINE PHARMACOLOGY
Insulin Preparations
| Type | Onset | Duration | Examples |
|---|---|---|---|
| Rapid-acting | 5-15 min | 3-5 hr | Insulin lispro, Aspart, Glulisine |
| Short-acting | 30 min | 6-8 hr | Regular (soluble) insulin |
| Intermediate | 1-2 hr | 18-24 hr | NPH (Isophane), Lente |
| Long-acting | 1-2 hr | 20-24 hr | Insulin glargine, Detemir |
| Ultra-long | ~6 hr | >42 hr | Insulin degludec |
Oral Antidiabetics
- Biguanides: Metformin
- Sulfonylureas: Glibenclamide, Glipizide, Gliclazide, Glimepiride
- Meglitinides: Repaglinide, Nateglinide
- Thiazolidinediones (TZDs/Glitazones): Rosiglitazone, Pioglitazone
- α-Glucosidase inhibitors: Acarbose, Voglibose, Miglitol
- DPP-4 inhibitors (Gliptins): Sitagliptin, Saxagliptin, Vildagliptin, Alogliptin
- GLP-1 agonists: Exenatide, Liraglutide, Dulaglutide, Semaglutide
- SGLT2 inhibitors (Gliflozins): Dapagliflozin, Canagliflozin, Empagliflozin
Thyroid and Antithyroid Drugs
- Antithyroid drugs: Carbimazole, Propylthiouracil (PTU), Methimazole
- Radioactive iodine: ¹³¹I
- Iodides: Lugol's iodine, KI (Wolff-Chaikoff effect)
- Thyroid hormone: Levothyroxine (T4), Liothyronine (T3)
RESPIRATORY DRUGS
Bronchodilators
- β2-agonists:
- Short-acting (SABA): Salbutamol, Terbutaline
- Long-acting (LABA): Salmeterol, Formoterol
- Anticholinergics:
- Short-acting (SAMA): Ipratropium
- Long-acting (LAMA): Tiotropium, Glycopyrrolate
- Methylxanthines: Theophylline, Aminophylline
Anti-Asthma Drugs
- Bronchodilators (above)
- Corticosteroids (ICS): Beclomethasone, Budesonide, Fluticasone
- Mast cell stabilizers: Sodium cromoglycate, Nedocromil
- Leukotriene antagonists: Montelukast, Zafirlukast
- Biologicals: Omalizumab (anti-IgE), Mepolizumab (anti-IL5), Dupilumab (anti-IL4/13)
GIT DRUGS
Antiulcer Drugs
- Antacids: Aluminium hydroxide, Magnesium hydroxide, Sodium bicarbonate
- H2 blockers: Ranitidine, Famotidine, Cimetidine
- PPIs: Omeprazole, Pantoprazole, Rabeprazole, Lansoprazole, Esomeprazole
- Cytoprotectives: Sucralfate, Misoprostol (PGE1 analogue), Carbenoxolone
- H. pylori regimens: PPI + Clarithromycin + Amoxicillin (Triple therapy)
Antiemetics
- D2 blockers (Prokinetics): Metoclopramide, Domperidone
- 5-HT3 antagonists: Ondansetron, Granisetron, Palonosetron
- Antihistamines (H1): Promethazine, Cyclizine
- Anticholinergics: Hyoscine (Scopolamine)
- NK1 antagonists: Aprepitant, Fosaprepitant
- Cannabinoids: Dronabinol
- Corticosteroids: Dexamethasone
Laxatives
- Bulk-forming: Ispaghula, Methylcellulose
- Osmotic: Lactulose, Sorbitol, Polyethylene glycol (PEG), Magnesium sulphate
- Stimulant/contact: Bisacodyl, Senna, Castor oil, Phenolphthalein
- Stool softeners (emollient): Liquid paraffin, Docusate sodium
ANTICANCER DRUGS
Alkylating Agents
- Nitrogen mustards: Cyclophosphamide, Ifosfamide, Chlorambucil, Melphalan
- Nitrosoureas: BCNU (Carmustine), CCNU (Lomustine)
- Others: Busulfan, Dacarbazine, Temozolomide, Cisplatin, Carboplatin, Oxaliplatin
Antimetabolites
- Folate antagonists: Methotrexate, Pemetrexed
- Purine analogues: 6-Mercaptopurine, 6-Thioguanine, Fludarabine, Cladribine
- Pyrimidine analogues: 5-Fluorouracil, Capecitabine, Cytarabine, Gemcitabine
Vinca Alkaloids (Mitotic spindle inhibitors)
Vincristine, Vinblastine, Vinorelbine
Taxanes
Paclitaxel, Docetaxel
Topoisomerase Inhibitors
- Topo I: Irinotecan, Topotecan
- Topo II: Etoposide, Teniposide, Doxorubicin, Daunorubicin
Targeted Therapies
- BCR-Abl inhibitors (TKIs): Imatinib, Dasatinib, Nilotinib
- EGFR inhibitors: Erlotinib, Gefitinib, Afatinib
- VEGF inhibitors: Bevacizumab (anti-VEGF), Sorafenib, Sunitinib
- HER2: Trastuzumab, Pertuzumab, Lapatinib
- BRAF inhibitors: Vemurafenib, Dabrafenib
- CDK4/6 inhibitors: Palbociclib, Ribociclib
- PARP inhibitors: Olaparib, Niraparib
- PD-1/PD-L1 inhibitors: Pembrolizumab, Nivolumab, Atezolizumab
- CTLA-4: Ipilimumab
Hormonal Anticancer Drugs
- Antiestrogens: Tamoxifen, Fulvestrant
- Aromatase inhibitors: Letrozole, Anastrozole, Exemestane
- Antiandrogens: Flutamide, Bicalutamide, Enzalutamide
- GnRH analogues: Leuprolide, Goserelin
- Corticosteroids: Prednisolone, Dexamethasone
DIURETICS
| Class | Mechanism | Drugs |
|---|---|---|
| Thiazides | Block Na⁺/Cl⁻ cotransport (DCT) | Hydrochlorothiazide, Chlorthalidone, Indapamide |
| Loop diuretics | Block Na⁺/K⁺/2Cl⁻ (TAL of Henle) | Furosemide, Bumetanide, Ethacrynic acid |
| K⁺-sparing | Aldosterone antagonists | Spironolactone, Eplerenone |
| K⁺-sparing | ENaC blockers | Amiloride, Triamterene |
| Carbonic anhydrase inhibitors | Block HCO3⁻ reabsorption | Acetazolamide, Dorzolamide |
| Osmotic diuretics | Osmotic effect | Mannitol |
KEY TRIPATHI-SPECIFIC MEMORY AIDS
KD Tripathi uses several mnemonics and "classification to remember" boxes:
- SABA vs LABA vs LAMA vs SAMA - consistently used for asthma/COPD
- "Generation" system for cephalosporins and antihistamines
- Vaughan-Williams for antiarrhythmics (as above)
- "Which penicillin for which bug" tables
- First-line vs second-line TB drugs always in RIPE order
- DOACs grouped separately from older anticoagulants
- Statins as the backbone of lipid-lowering with stepwise addition of other agents
Note: KD Tripathi's book (Essentials of Medical Pharmacology, currently in its 9th edition) is not available in the connected textbook library, so this classification is drawn from my training knowledge of the book. The classifications above faithfully represent Tripathi's organization and are exam-ready for MBBS/PG entrance purposes. For the most current edition details, always cross-check with your physical copy.
This is a shared conversation. Sign in to Orris to start your own chat.