Explain about different electrolyte imbalance in body which can be seen in ECG
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Searching Images
hypercalcemia hypocalcemia ECG changes QT interval
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple textbooks and ECG images. Let me compile the complete answer.
Electrolyte Imbalances and ECG Changes
Electrolytes directly govern cardiac action potential generation and conduction. The key electrolytes with visible ECG manifestations are potassium, calcium, and magnesium. Sodium imbalances alone rarely produce distinct ECG changes.
1. Potassium (K⁺)
Hyperkalemia (K⁺ > 5.0 mEq/L)
Hyperkalemia produces the most dramatic and dangerous ECG progression of any electrolyte disturbance. Changes correlate roughly with the serum level but can be unpredictable — progression from mild to life-threatening cardiac effects may occur rapidly.
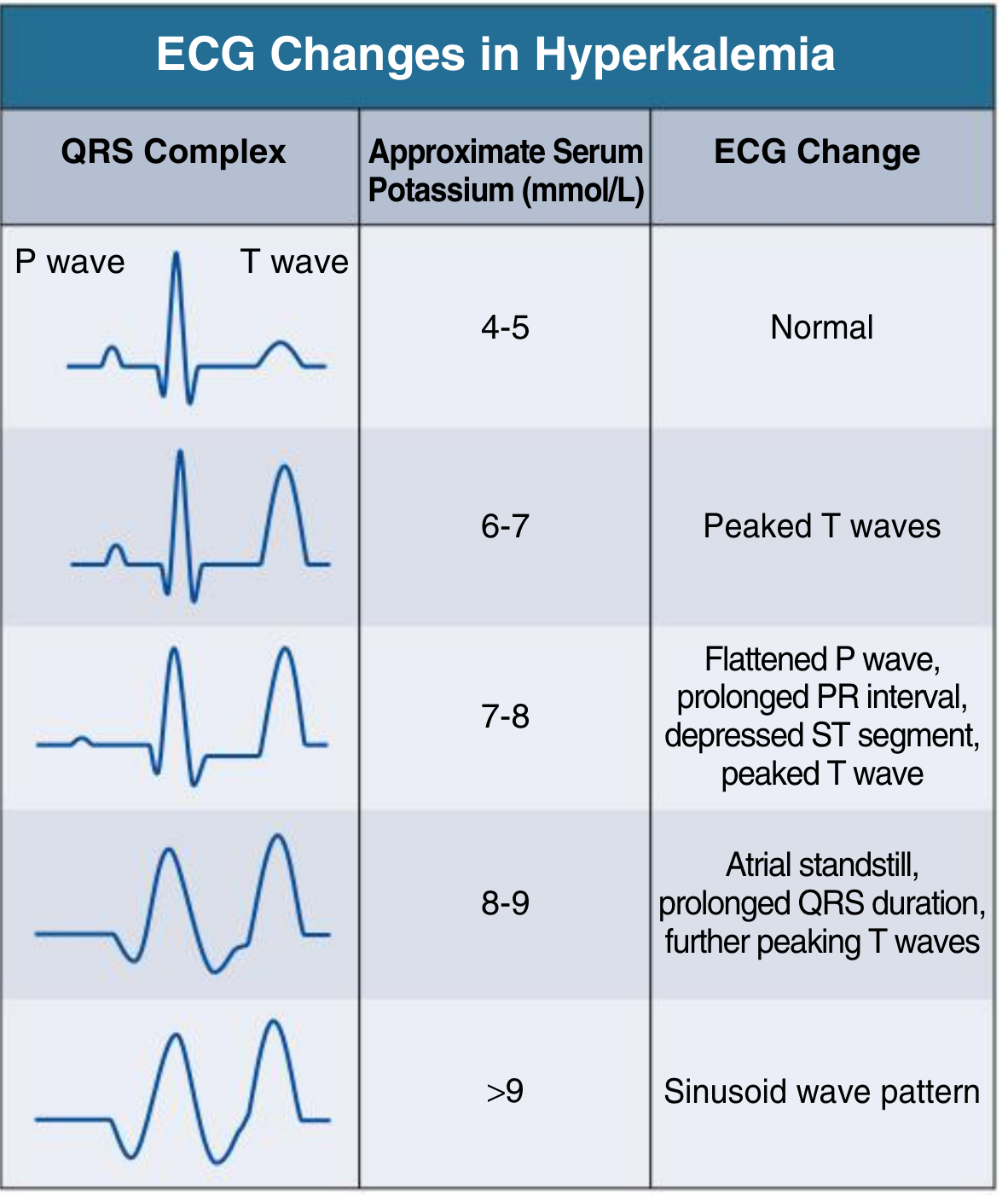
Progressive ECG stages by serum K⁺:
| K⁺ (mmol/L) | ECG Change |
|---|---|
| 4–5 | Normal |
| 6–7 | Peaked ("tented") T waves — tall, narrow, symmetric; most evident in precordial leads |
| 7–8 | Flattened P wave, prolonged PR interval, depressed ST segment |
| 8–9 | Atrial standstill (P waves disappear), prolonged QRS duration |
| >9 | Sine wave pattern → ventricular fibrillation |
The mechanism: elevated K⁺ reduces the resting membrane potential, slowing depolarization and conduction throughout the myocardium. ECG changes should be treated as a medical emergency regardless of symptoms. — Comprehensive Clinical Nephrology, 7e; Schwartz's Principles of Surgery, 11e
Hypokalemia (K⁺ < 3.5 mEq/L)
ECG findings:
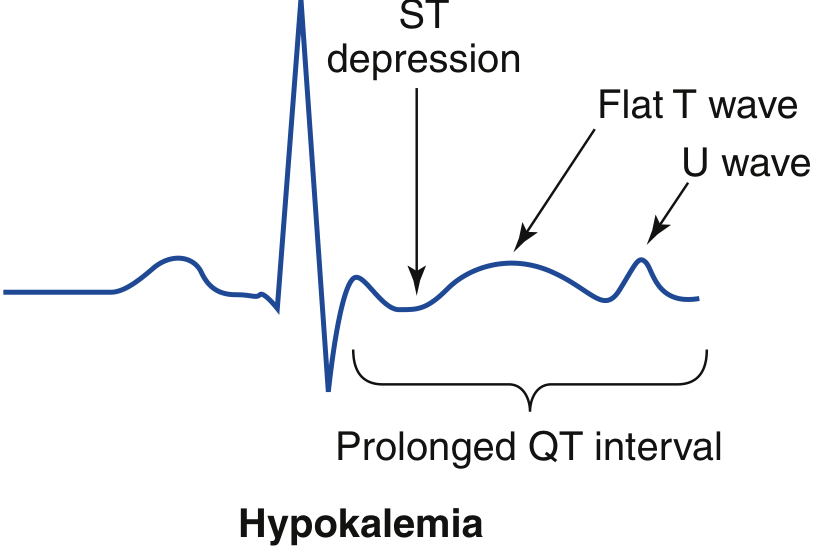
- Flattening or inversion of T waves — hallmark early finding
- Prominent U waves — small positive deflections after the T wave (best seen in V2–V3); pathognomonic for hypokalemia
- ST-segment depression
- Prolonged QU interval (often mistaken for QT prolongation)
- Severe depletion: prolonged PR interval, decreased QRS voltage, widened QRS complex
The practical danger: torsades de pointes can occur, especially if QT (QU) >500 ms. — Washington Manual of Medical Therapeutics; Rosen's Emergency Medicine
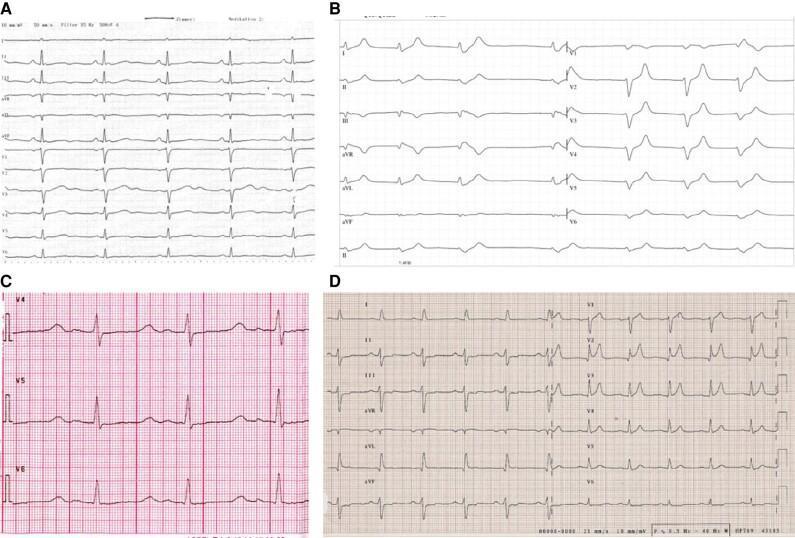
The real 12-lead ECG below (Panel A) shows flattened T waves and prominent U waves in hypokalemia; Panel B shows hyperkalemia with tall peaked T waves:
2. Calcium (Ca²⁺)
Calcium affects phase 2 (plateau) of the action potential — altering the duration of the ST segment and thus the QT interval.
Hypercalcemia (total Ca²⁺ > 10.5 mg/dL)
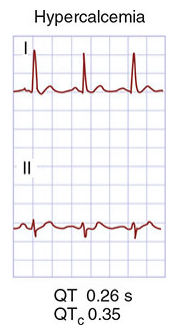
ECG findings:
- Shortened QT interval — the hallmark (due to shortened ST segment/phase 2)
- Prolonged PR and QRS intervals
- T-wave flattening and widening
- Increased QRS voltage
- Atrioventricular block → can progress to complete heart block and cardiac arrest
- Worsening of digitalis toxicity
Schwartz's Principles of Surgery, 11e; Harrison's Principles of Internal Medicine, 22e
Hypocalcemia (total Ca²⁺ < 8.5 mg/dL)
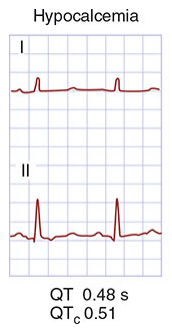
ECG findings:
- Prolonged QT interval — due to prolonged ST segment (phase 2 lengthened); T-wave morphology is relatively preserved
- T-wave inversion
- Heart block
- Ventricular fibrillation (in severe cases)
The QT prolongation in hypocalcemia is specifically from ST-segment lengthening, not T-wave widening — this distinguishes it from drug-induced QT prolongation. — Schwartz's Principles of Surgery, 11e; Harrison's Principles, 22e
3. Magnesium (Mg²⁺)
Magnesium acts as a cofactor for Na⁺/K⁺-ATPase and stabilizes cardiac cell membranes. Importantly, hypomagnesemia often coexists with and perpetuates hypokalemia and hypocalcemia.
Hypermagnesemia (Mg²⁺ > 2.5 mEq/L)
ECG findings (similar to hyperkalemia):
- Increased PR interval
- Widened QRS complex
- Elevated T waves
- Can lead to heart block, hypotension, and cardiac arrest
Usually seen in severe renal insufficiency or excess magnesium administration (e.g., eclampsia therapy). — Schwartz's Principles of Surgery, 11e
Hypomagnesemia (Mg²⁺ < 1.5 mEq/L)
ECG findings:
- Prolonged QT and PR intervals
- Widened QRS complex
- ST-segment depression
- Flattening or inversion of P waves and T waves
- Torsades de pointes — the classically associated arrhythmia; may respond only to magnesium repletion
Hypomagnesemia is especially important in the ICU and in patients on diuretics, alcoholics, and those with malabsorption. Persistent hypokalemia that does not correct with potassium replacement should prompt measurement of serum magnesium. — Washington Manual of Medical Therapeutics; Schwartz's Principles of Surgery, 11e
Summary Table
| Electrolyte | Disturbance | Key ECG Findings | Dangerous Arrhythmia |
|---|---|---|---|
| K⁺ | Hyperkalemia | Peaked T → flat P → wide QRS → sine wave | VF |
| K⁺ | Hypokalemia | Flat T, prominent U wave, ST depression, prolonged QU | Torsades de pointes |
| Ca²⁺ | Hypercalcemia | Shortened QT (short ST segment) | AV block → VF |
| Ca²⁺ | Hypocalcemia | Prolonged QT (long ST segment) | VF |
| Mg²⁺ | Hypermagnesemia | Prolonged PR, wide QRS, elevated T | Heart block |
| Mg²⁺ | Hypomagnesemia | Prolonged QT/PR, wide QRS, ST depression | Torsades de pointes |
Mnemonic for QT interval:
"Hypocalcemia and hypomagnesemia LONG it; hypercalcemia SHORT it"
⚠️ Clinical pearl: Hypomagnesemia should always be corrected alongside hypokalemia — magnesium depletion causes ongoing renal potassium wasting that makes hypokalemia refractory to replacement alone.
This is a shared conversation. Sign in to Orris to start your own chat.