Hirshsprung disease pediatric
Reading File
Finding Sources
Searching PubMed
Hirschsprung disease children management
Reading File
Reading File
Reading File
Searching Images
Hirschsprung disease barium enema transition zone aganglionic colon
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is a complete, well-structured overview of Hirschsprung disease in pediatrics.
Hirschsprung Disease (Congenital Aganglionic Megacolon)
Epidemiology
- Incidence: 1 in 5,000 live births
- Male:female ratio ≈ 4:1 (though females tend to have more severe/longer-segment disease)
- ~10% of cases are associated with Down syndrome (trisomy 21)
- Siblings of affected children are at increased risk
- Also associated with: MEN 2A/2B, cardiac septal defects, cleft palate, anorectal atresias, other neurocristopathies
Pathogenesis
Hirschsprung disease is a neurocristopathy — it results from failure of neural crest cell migration during embryogenesis (weeks 5–12 of gestation). Neural crest cells normally migrate caudally from the cecum to the rectum to populate the enteric nervous system. When this migration is arrested, the distal bowel is left without:
- Auerbach myenteric plexus
- Meissner submucosal plexus
The resulting aganglionosis causes a loss of coordinated peristalsis and failure of internal anal sphincter relaxation — producing functional obstruction at the aganglionic segment.
Key Genetics
- RET proto-oncogene (chromosome 10q11.2) — loss-of-function mutations account for the majority of familial cases and ~15% of sporadic cases. RET is a receptor tyrosine kinase; its ligands (GDNF, neurturin) are expressed in gut mesenchyme during development
- Other genes involved in neural crest cell development also implicated
- Inheritance is typically non-Mendelian (variable penetrance)
Anatomic Distribution
Aganglionosis always begins at the anorectal line and extends proximally. Segment lengths:
| Segment | Frequency |
|---|---|
| Rectosigmoid (short-segment) | ~75–80% |
| Proximal to sigmoid (long-segment) | ~17% |
| Total colonic aganglionosis (TCA) ± distal ileum | ~8% |
| Ultrashort segment (internal sphincter only) | Rare |
| Total intestinal Hirschsprung | Very rare |
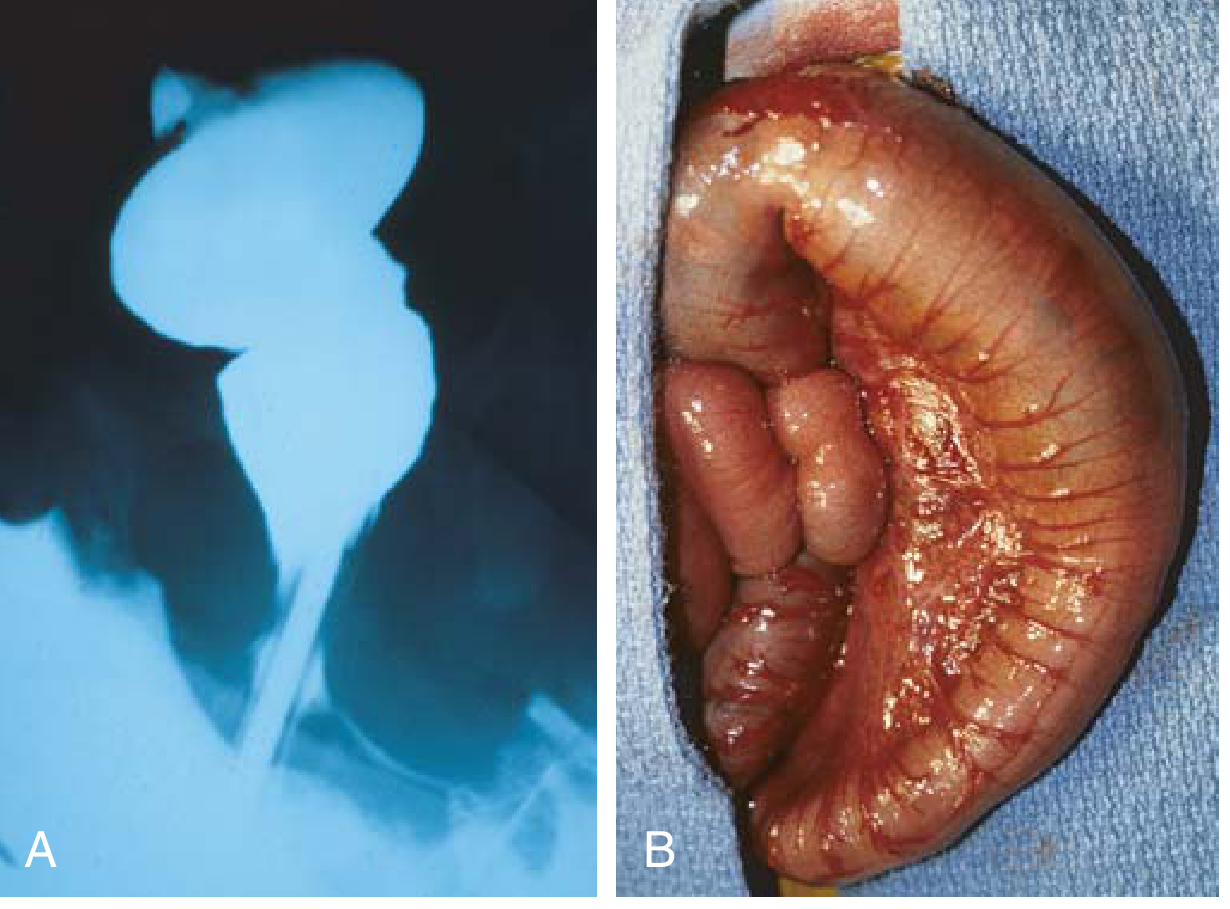
Key anatomic paradox: The aganglionic distal bowel appears narrow/normal caliber externally; the normal proximal bowel becomes progressively dilated (megacolon) due to obstruction.
Clinical Presentation
Neonatal (>90% of cases)
- Failure to pass meconium within the first 24 hours of life (classic hallmark)
- Abdominal distension
- Bilious vomiting
- Symptoms may temporarily resolve after digital rectal exam or rectal thermometer insertion (decompression), but recur without treatment
Older children / missed diagnosis
- Chronic constipation from birth
- Progressive abdominal distension
- Failure to thrive
- Longer-segment disease can paradoxically present later (milder initial symptoms)
Hirschsprung-Associated Enterocolitis (HAEC) — Most feared complication
- Occurs in 18–50% of patients, both pre- and postoperatively
- Leading cause of death in Hirschsprung disease
- Presents with: severe bloody diarrhea, fever, abdominal distension, sepsis, shock, peritonitis
- Higher frequency in: long-segment disease, delayed diagnosis (after 1st week of life)
Diagnosis
Imaging
Contrast enema (first-line in neonates)
- Shows: narrow aganglionic distal rectum → transition zone → dilated proximal colon
- Failure to evacuate contrast after 24 hours is highly suggestive
- Also excludes: meconium plug, small left colon syndrome, intestinal atresia
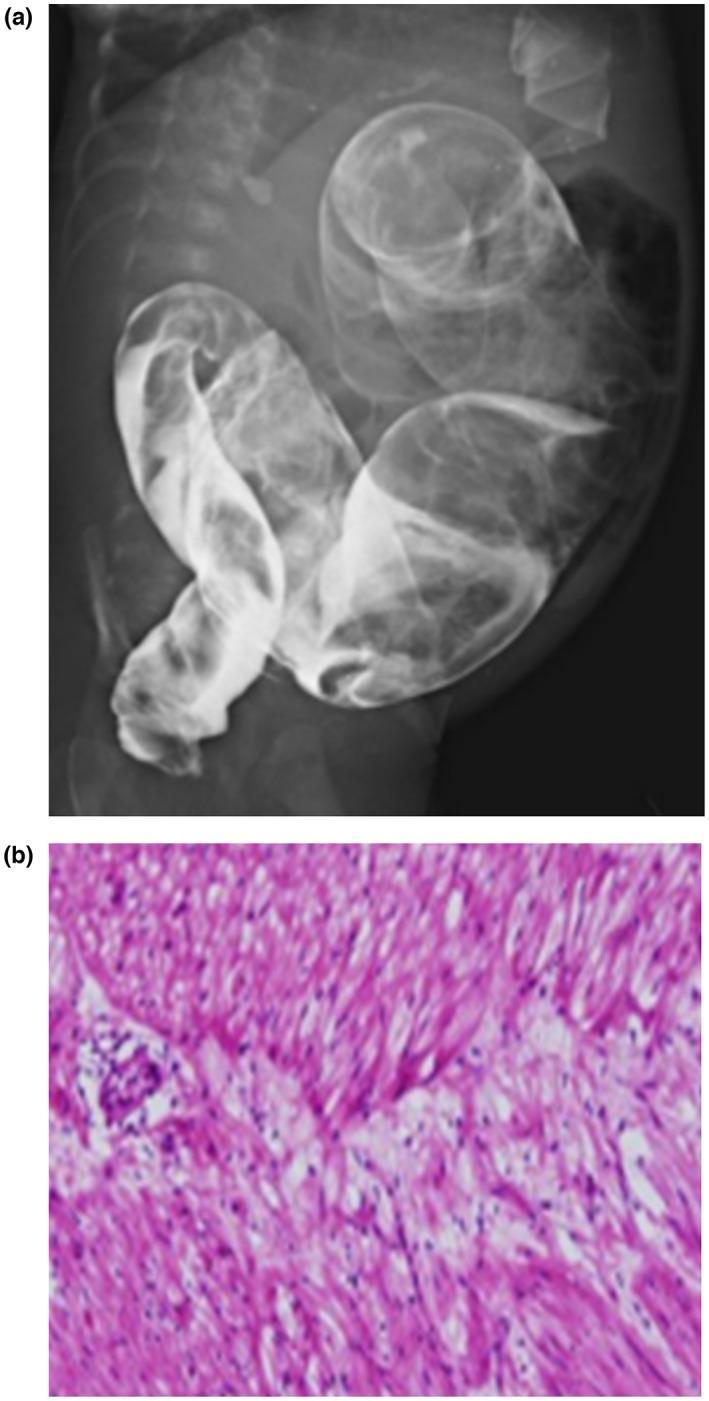
Plain abdominal radiograph
- Low bowel obstruction pattern; may show a paucity of rectal gas
Anorectal manometry (toddlers)
- Failure of internal sphincter relaxation on rectal balloon distension — can be diagnostic
Histopathology — Gold Standard
Rectal biopsy is the definitive diagnosis:
- Newborns: suction rectal biopsy at bedside (2+ specimens, ≥5–10 mm above dentate line, 1 cm apart)
- Older children: full-thickness biopsy under general anesthesia (thicker mucosa not amenable to suction technique)
Histologic criteria:
- Absent ganglion cells in submucosal/myenteric plexuses
- Hypertrophied nerve trunks
- Robust acetylcholinesterase immunostaining (increased AChE-positive fibers)
- Calretinin immunostaining — now a standard adjunct (absent staining in aganglionic segment)
Management
Preoperative / Bridging
- Daily rectal irrigations with warm normal saline via soft red rubber catheter (1–2×/day, until clear effluent returns) — decompresses the bowel
- Leveling colostomy with intraoperative biopsies — used when irrigations are not feasible (comorbidities, family limitations, long-segment disease), to identify the level of normally ganglionated bowel
Definitive Surgery — Pull-Through Procedures
All procedures share the same principle: resection of the aganglionic segment with pull-through of normally innervated bowel to the anal margin. Three classic techniques:
| Procedure | Approach | Key Feature |
|---|---|---|
| Swenson (1949) | Abdominal/perineal, full-thickness rectal dissection | Original technique; low anastomosis 5 mm above dentate line |
| Soave | Endorectal pull-through, preserves muscular cuff | Strips mucosa, pulls ganglionic bowel through retained rectal muscle |
| Duhamel | Retrorectal pull-through | Side-to-side anastomosis of ganglionic bowel behind the aganglionic rectum |
Minimally invasive options: Laparoscopic and single-incision laparoscopic pull-through are now standard at many centers. Robotic surgery is also emerging (PMID 41028657).
Recent meta-analyses (2025) compare Soave vs. Swenson procedures in terms of complications, continence, and enterocolitis recurrence (PMID 41454984).
Postoperative Complications
- Anastomotic leak, fistula, abscess, stenosis
- Persistent/recurrent Hirschsprung-associated enterocolitis
- Constipation or soiling (bowel function may take years to normalize)
- Up to 10% of patients may eventually require a permanent colostomy
- Total intestinal Hirschsprung disease — notoriously difficult; requires parenteral nutrition support
Differential Diagnosis of Delayed Meconium Passage
| Condition |
|---|
| Ileal atresia |
| Meconium ileus (cystic fibrosis) |
| Functional immaturity of the colon |
| Colon atresia |
| Anorectal malformations |
| Hirschsprung disease |
| Megacystis-microcolon-intestinal hypoperistalsis syndrome |
| Extrinsic compression by mass (mesenteric/duplication cyst) |
| Paralytic ileus (sepsis, drugs, metabolic) |
Summary Table
| Feature | Detail |
|---|---|
| Incidence | 1 in 5,000 births |
| M:F ratio | 4:1 |
| Genetics | RET proto-oncogene (chr. 10q11.2); non-Mendelian |
| Association | Down syndrome (10%), MEN 2A/2B |
| Pathology | Absent Auerbach + Meissner plexuses; distal → proximal |
| Most common segment | Rectosigmoid (75–80%) |
| Classic presentation | Failure to pass meconium in first 24 h |
| Deadliest complication | Hirschsprung enterocolitis |
| Imaging | Contrast enema — transition zone |
| Gold standard diagnosis | Rectal biopsy (suction or full-thickness) |
| Histology markers | Absent ganglion cells; ↑ AChE; absent calretinin |
| Treatment | Pull-through surgery (Swenson/Soave/Duhamel) |
Sources: Sabiston Textbook of Surgery; Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology; Yamada's Textbook of Gastroenterology
Recent evidence: Current surgical literature (2025) favors minimally invasive pull-through with equivalent or superior outcomes to open surgery [PMID 41023221, 41454984, 41028657].
Ribbon like stool seen in
Finding Sources
Finding Sources
Reading File
Finding Sources
Here is a concise, exam-ready answer:
Ribbon-Like (Pencil-Thin) Stool — Causes
Ribbon-like (narrow, flat, or pencil-thin) stools indicate luminal narrowing somewhere in the distal colon, rectum, or anal canal. The key causes:
Primary / Classic Cause
1. Carcinoma of the Left Colon / Rectum (most important)
- The annular (apple-core/napkin ring) carcinoma of the sigmoid colon or rectum narrows the lumen circumferentially
- Ribbon-like stool is a classic symptom of left-sided colorectal carcinoma — one of the earliest alarming symptoms
- Accompanied by: change in bowel habits, rectal bleeding, tenesmus, weight loss
Other Important Causes
2. Anal Stenosis
- A fibrous ring at the anal verge causes constipation and gives stool a ribbon-like appearance
- Responds well to dilation or surgical disruption
- — Sleisenger & Fordtran's GI and Liver Disease
3. Anal Canal Spasm / Levator Spasm (Proctalgia fugax)
- Functional narrowing of the anal outlet
4. Stricture of the Rectum / Anal Canal
- Post-inflammatory (Crohn's disease, radiation proctitis, lymphogranuloma venereum)
- Post-surgical anastomotic stricture
5. External Compression of the Rectum
- Pelvic masses (ovarian cyst, fibroid, presacral tumor)
- Pelvic floor dysfunction
6. Spinal Cord / Neurological Causes
- Ribbon-like stools are listed among symptoms prompting urological/neurological evaluation (alongside urinary/fecal incontinence and lower extremity neurological signs) — suggests dysfunctional defecation from spinal dysraphism or tethered cord syndrome
- — Campbell-Walsh-Wein Urology
Summary Table
| Cause | Mechanism | Key Clue |
|---|---|---|
| Left-sided colorectal carcinoma | Annular luminal obstruction | ± rectal bleeding, weight loss, age >50 |
| Anal stenosis | Fibrous ring at anal verge | Congenital or acquired (post-op, IBD) |
| Rectal/anal stricture | Post-inflammatory or post-radiation | History of Crohn's, radiation, STI |
| External pelvic compression | Extrinsic narrowing | Pelvic mass on imaging |
| Spinal cord lesion | Neurogenic dysmotility | Lower limb neuro symptoms, sacral anomaly |
Exam pearl: In most clinical/exam contexts, ribbon-like or pencil-thin stool = carcinoma of the left/sigmoid colon or rectum until proven otherwise. It should be investigated urgently with colonoscopy.
This is a shared conversation. Sign in to Orris to start your own chat.