Here are the complete, unified notes on Junctional Rhythm - everything in one place:
JUNCTIONAL RHYTHM - Complete Notes
SECTION 1: PHYSIOLOGY - Normal Cardiac Conduction
The Pacemaker Hierarchy
The heart has a layered system of backup pacemakers, each firing slower as you go further from the SA node:
| Pacemaker Site | Intrinsic Rate | Notes |
|---|
| SA node | 60-100 bpm | Dominant pacemaker; suppresses all below |
| Atrial tissue | 50-60 bpm | Rarely takes over |
| AV node / His bundle (AV Junction) | 40-60 bpm | Source of junctional rhythm |
| Bundle branches / Purkinje | 20-40 bpm | Source of ventricular/idioventricular rhythm |
| Ventricular myocardium | 20-30 bpm | Last resort, unreliable |
How the SA Node Suppresses the AV Junction - Overdrive Suppression
The SA node fires at 70-80 bpm. Every time it fires, the impulse reaches the AV junction, resets its membrane potential, and restarts the junction's spontaneous depolarization clock before it ever completes. The junction never gets a chance to fire on its own. This is called overdrive suppression - the faster pacemaker continuously suppresses slower ones by keeping them perpetually reset.
SA node fires at 75 bpm (every 800 ms)
AV junction would fire at 50 bpm (every 1200 ms)
SA impulse arrives at 800 ms → resets junction
Junction never reaches 1200 ms threshold
→ Junction is suppressed
Why the AV Node Has a Narrow QRS When It Fires
When the AV junction fires, its impulse travels downward through the normal His-Purkinje system - the same pathway used in normal sinus rhythm. The ventricles are activated rapidly and synchronously. Therefore the QRS is narrow (< 0.12 s). This distinguishes junctional from ventricular rhythms (which produce a wide QRS because they bypass the His-Purkinje system).
The AV Node Pacemaker Cells - Cellular Mechanism
Pacemaker cells in the AV junction undergo phase 4 spontaneous diastolic depolarization - the membrane potential gradually drifts from -60 mV toward threshold (-40 mV). This is driven by:
- If (funny) current - slow inward Na+ through HCN channels (hyperpolarization-activated cyclic nucleotide-gated channels)
- Progressive Na+ entry makes the membrane progressively less negative
- At threshold (-40 mV): L-type calcium channels open → action potential fires
Factors that steepen phase 4 slope (increase automaticity):
- Catecholamines, sympathetic activation
- Digoxin toxicity, ischemia
Factors that flatten phase 4 slope (decrease automaticity):
- Beta-blockers, vagal tone
- Calcium channel blockers
Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 645; Tintinalli's Emergency Medicine, p. 147
SECTION 2: DEFINITION
A junctional rhythm is any cardiac rhythm that arises from the AV node or Bundle of His (collectively called the AV junction) rather than the SA node.
Two fundamental mechanisms generate junctional rhythms:
| Mechanism | Explanation | Clinical Correlate |
|---|
| Passive escape | SA node slows below AV junction rate → junction "escapes" suppression | Junctional escape rhythm (protective) |
| Enhanced automaticity | AV junction fires faster than normal, exceeding SA node | Accelerated junctional rhythm / Junctional tachycardia (pathological) |
SECTION 3: ETIOLOGY AND CAUSES
Group A - SA Node Depression / Failure (leads to passive escape)
- Sick sinus syndrome (drug-induced or intrinsic)
- High vagal tone - athletes, sleep, carotid sinus hypersensitivity, vasovagal
- Inferior MI - RCA occlusion ischemia of SA node (60% RCA-supplied) and AV node
- Sinus bradycardia, sinus arrest, sinoatrial exit block
- 2nd or 3rd degree AV block - impulse blocked before reaching junction
Group B - Medications (Common)
- Digoxin - most classic cause of all types of junctional rhythm
- Beta-blockers - propranolol, metoprolol, atenolol
- Calcium channel blockers - verapamil, diltiazem
- Amiodarone, adenosine
- Inhalation anesthetics (depress SA node > AV node)
- Anticholinesterase agents
Group C - Enhanced Automaticity (leads to accelerated/tachycardic junctional)
- Digoxin toxicity - lowers resting membrane potential of junctional cells
- Inferior MI / AV nodal ischemia
- Post-cardiac surgery (VSD repair, AV canal, Fontan)
- Catecholamine excess, sympathomimetics, isoproterenol infusion
- Acute rheumatic fever
- Myocarditis
Group D - Metabolic
- Hypokalemia - most important electrolyte trigger
- Hyperkalemia (severe)
- Hypoxia, acidosis
- Hypothyroidism (slows SA node)
Group E - Physiologic / Benign
- Young healthy adults, athletes during sleep
- Isorhythmic AV dissociation (incidental, no treatment)
Tintinalli's Emergency Medicine;
StatPearls NBK507715;
Braunwald's Heart Disease
SECTION 4: THE CORE ECG PRINCIPLE - Understanding P Waves in Junctional Rhythm
This one principle explains ALL ECG findings in junctional rhythm:
When the AV junction fires, it sends impulses in TWO directions simultaneously: DOWN into the ventricles (anterograde) and UP into the atria (retrograde).
Why QRS is Narrow
Downward conduction uses the normal fast His-Purkinje system → synchronized ventricular depolarization → narrow QRS
Why P Waves Are Inverted (Retrograde)
In normal sinus rhythm, the SA node fires at the top of the right atrium. Depolarization spreads top-to-bottom across the atria. Lead II (pointing downward/leftward) sees the wave coming toward it → upright P wave.
In junctional rhythm, the AV junction fires from below. Depolarization spreads bottom-to-top through the atria (retrograde). Lead II sees the wave moving away from it → inverted P wave.
Normal: SA node (top) → atria depolarize top-to-bottom
Lead II "sees" wave coming → UPRIGHT P ↑
Junctional: AV junction (bottom) → atria depolarize bottom-to-top
Lead II "sees" wave going away → INVERTED P ↓
Lead aVR "sees" wave coming → UPRIGHT P ↑ (in aVR)
Why P Waves Appear in Different Positions Relative to QRS
Depends on which direction (up or down) is faster:
Retrograde faster than anterograde:
→ Atria fire BEFORE ventricles
→ P wave BEFORE QRS (inverted, PR < 0.12 s)
Retrograde = anterograde speed:
→ Atria and ventricles fire SIMULTANEOUSLY
→ P wave INSIDE/BURIED within QRS (invisible)
Anterograde faster than retrograde:
→ Ventricles fire BEFORE atria
→ P wave AFTER QRS (inverted notch in ST segment, RP < 0.20 s)
Three ECG variants of junctional P wave position. Top: P hidden inside QRS (simultaneous activation). Middle: Inverted P before QRS (PR < 0.12 s - retrograde faster). Bottom: Inverted P after QRS (appears as notch in ST segment - anterograde faster). Source: UNM
SECTION 5: TYPES, MECHANISMS, AND ECG CORRELATION
TYPE 1: Junctional Escape Rhythm
Rate: 40-60 bpm
Mechanism - "The Safety Net" (Passive)
The SA node's overdrive suppression on the AV junction fails. The junction is simply released from suppression and fires at its own intrinsic rate. This is not pathological firing - it is a protective mechanism. Without it, the patient would have asystole.
SA node slows/fails (< 40-60 bpm)
↓
AV junction no longer receives SA impulses before it reaches threshold
↓
AV junction fires at own rate (40-60 bpm)
↓
Anterograde: Normal His-Purkinje → NARROW QRS
Retrograde: Bottom-to-top atria → INVERTED P (or hidden if simultaneous)
↓
Result: Regular, slow, narrow complex rhythm — NO normal sinus P waves
Key rule: NEVER terminate a junctional escape rhythm if it is the patient's only rhythm. Doing so causes asystole.
ECG Features
| Feature | Finding |
|---|
| Rate | 40-60 bpm |
| Rhythm | Regular |
| P wave | Absent, OR inverted in II/III/aVF (before, within, or after QRS) |
| PR interval | < 0.12 s if P precedes QRS; unmeasurable if P absent or after QRS |
| QRS | Narrow (< 0.12 s) |
ECG Example 1 - Junctional Escape with Annotated Inverted P Wave
Junctional escape rhythm: Regular narrow complexes at 40-60 bpm. One beat shows a clearly labeled inverted retrograde P wave (highlighted in red) just before the QRS. PR interval is very short (< 0.12 s). This is the junction activating the atria from below.
ECG Example 2 - Sinus Pause Triggering Junctional Escape
Classic junctional escape beat triggered by sinus pause: Normal sinus beats followed by a long pause (SA node fails to fire). The AV junction escapes, producing a narrow QRS. The retrograde P wave appears AFTER the QRS (green annotation) - anterograde conduction was faster than retrograde. This is the junction rescuing the patient from a prolonged pause.
ECG Example 3 - Severe Junctional Bradycardia (Rate 25 bpm)
Severe junctional bradycardia (HR = 25 bpm, RR intervals 2000-2640 ms): This is the extreme slow end of junctional escape, bordering on junctional bradycardia (< 40 bpm). Narrow QRS complexes in V5 mod and Lead II mod, no normal sinus P waves. This patient requires urgent pacing.
TYPE 2: Accelerated Junctional Rhythm (AJR)
Rate: 60-100 bpm
Mechanism - "Enhanced Automaticity Overtakes the SA Node" (Active)
This is not a passive escape. The AV junction develops enhanced automaticity - the slope of phase 4 spontaneous diastolic depolarization steepens, causing the junction to reach threshold faster. It fires at 60-100 bpm, exceeding the SA node rate. The AV junction actively takes over the pacemaker role.
Normal state: SA node 75 bpm > AV junction 50 bpm → SA controls
AJR state: SA node 75 bpm < AV junction 80 bpm ← enhanced automaticity
↓
AV junction captures heart rate (overtakes SA node)
→ Narrow QRS at 60-100 bpm
→ SA P waves may be dissociated (AV dissociation)
→ Retrograde P waves inverted in II, III, aVF
→ Rate looks "normal" on the strip but P waves are wrong
Important: AJR rate "looks normal" - this makes it easy to miss. The absence of normal upright sinus P waves before each QRS is the giveaway.
Triggers: Digoxin toxicity, inferior MI, catecholamines, post-cardiac surgery, rheumatic fever, inhalation anesthetics (suppress SA node more than AV node).
ECG Features
| Feature | Finding |
|---|
| Rate | 60-100 bpm |
| Rhythm | Regular |
| P wave | Absent, inverted, or AV dissociation (independent slow sinus P waves between QRS) |
| PR interval | < 0.12 s or unmeasurable |
| QRS | Narrow |
| Digoxin clue | ST depression, scooped ST segment ("Salvador Dali's moustache"), prolonged PR before AJR begins |
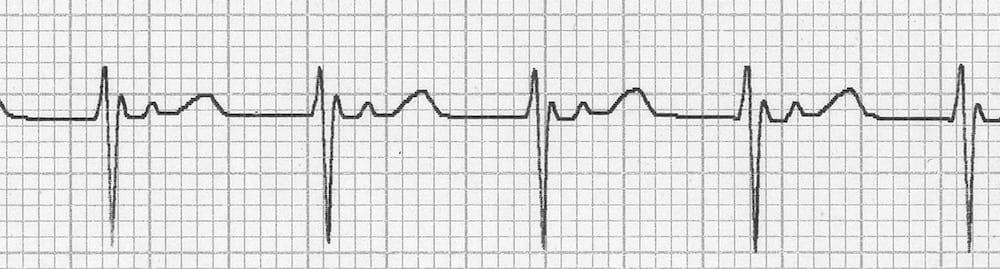
ECG Example - Accelerated Junctional Rhythm with Retrograde P in ST Segment
AJR (Lead II): Regular narrow complex rhythm at ~70-80 bpm. Note the small inverted deflections just after each QRS in the early ST segment - these are retrograde P waves, the AV junction activating the atria from below. The rate "looks normal" but the P wave morphology and position reveal the junctional origin. Source: LITFL
TYPE 3: Junctional Tachycardia
Rate: > 100 bpm (typically 120-220 bpm)
Two distinct mechanisms:
3A. Automatic Junctional Tachycardia (Enhanced Automaticity, Extreme Form)
Same mechanism as AJR but more extreme. Phase 4 depolarization slope is markedly steepened, causing the AV junction to fire > 100 bpm. Can reach 120-220 bpm.
Distinguishing features vs. re-entrant:
- Gradual onset (warm-up phenomenon)
- Slight rate variability
- Does NOT terminate with vagal maneuvers or adenosine (only transiently slows)
Clinical associations: Digoxin toxicity (most classic), inferior MI, myocarditis, post-cardiac surgery (especially in pediatrics), catecholamine infusion.
3B. Re-entrant Junctional Tachycardia (AVNRT)
A completely different mechanism - a circus movement re-entry circuit forms within the AV node using two functionally distinct pathways:
┌─────── FAST pathway ───────┐
│ (fast conduction, │
│ long refractory period) │
Atria Bundle of His → Ventricles
│ (slow conduction, │
│ short refractory period) │
└─────── SLOW pathway ───────┘
Typical AVNRT: impulse goes DOWN slow path, UP fast path
→ Atria and ventricles activated nearly simultaneously
→ P wave buried in QRS or just after (very short RP interval < 70 ms)
→ "Pseudo-r'" in V1 or "Pseudo-s" in inferior leads
Atypical AVNRT: impulse goes DOWN fast path, UP slow path
→ Long RP interval
Distinguishing features vs. automatic:
- Abrupt onset and termination ("paroxysmal")
- Regular rate without variability
- Terminates with vagal maneuvers or adenosine (breaks the circuit)
- Adenosine produces brief AV block, interrupts the circuit
ECG Features (Both Types)
| Feature | Finding |
|---|
| Rate | > 100 bpm (120-220) |
| Rhythm | Regular (re-entry) or slightly irregular (automatic) |
| P wave | Retrograde, inverted in II/III/aVF; upright in aVR and V1 |
| P position | Usually within or just after QRS (typical AVNRT) |
| RP interval | Short (< 70 ms in typical AVNRT) |
| PR interval | < 0.12 s if P precedes QRS |
| QRS | Narrow (may be wide with aberrancy) |
| Pseudo-r' in V1 | Classic sign of typical AVNRT (retrograde P distorting end of QRS) |
ECG Example - Junctional Tachycardia with Retrograde P Waves After QRS
Junctional tachycardia (re-entrant / AVNRT): Narrow complex tachycardia at ~160 bpm. Small retrograde P waves are visible just AFTER each QRS (short RP interval). These are inverted in inferior leads (II, III, aVF) - the re-entry circuit activates the atria retrogradely. The very short RP (< 70 ms) is pathognomonic of typical AVNRT. This terminates with adenosine. Source: LITFL
TYPE 4: Premature Junctional Complex (PJC)
Single early beat (not a sustained rhythm)
Mechanism - "One Early Ectopic Beat from the Junction"
An irritable focus in the AV junction fires before the next expected sinus beat. This interrupts the regular sinus rhythm with one early, abnormal beat, then sinus rhythm resumes.
Sinus beat → Sinus beat → AV junction fires EARLY (PJC)
↓
Narrow QRS (early, same morphology as sinus beats)
Inverted P wave (retrograde atrial activation)
Non-compensatory pause follows (retrograde P resets SA node)
↓
Sinus rhythm resumes
Compensatory vs. non-compensatory pause:
- PJC → non-compensatory pause (total cycle = < 2x normal R-R): retrograde P resets SA node
- PVC → compensatory pause (total cycle = 2x normal R-R): SA node not reset
ECG Features
| Feature | Finding |
|---|
| Rate | Underlying rhythm rate (irregular due to early beat) |
| The PJC beat | Premature, narrow QRS - identical morphology to sinus beats |
| P wave of PJC | Inverted before, hidden within, or just after QRS |
| PR interval | < 0.12 s if P before QRS |
| Post-PJC pause | Non-compensatory |
ECG Example - PJC with Inverted P Wave
PJC: A narrow premature QRS appears early in the cycle. The P wave just before it is inverted (retrograde) with a very short PR interval (< 0.12 s) - this is bottom-to-top atrial activation. PJC is distinguished from PAC (atrial ectopic) by the inverted P + short PR, and from PVC by the narrow QRS. Source: RegisteredNurseRN
TYPE 5: Junctional Escape in Complete Heart Block
Rate: 40-60 bpm (junctional), but P waves present and dissociated
Mechanism - "Block Above, Escape Below"
3rd degree (complete) AV block means no sinus impulses conduct to the ventricles. The SA node fires normally (P waves present at normal rate), but every single impulse is blocked. Below the block, the AV junction (or ventricle) escapes and fires at its own intrinsic rate. This produces AV dissociation - P waves and QRS complexes are completely independent.
SA node fires at 75 bpm → P waves visible at 75 bpm
Complete block at AV node → no impulses get through
↓
AV junction escapes at 40-60 bpm → narrow QRS at 40-60 bpm
P waves and QRS completely UNRELATED to each other
↓
ECG: P waves march through at their own rate (75 bpm)
QRS complexes at slower junctional rate (50 bpm)
No fixed relationship between P and QRS
Occasional "capture beats" where a P fortuitously conducts
This is distinguished from isorhythmic AV dissociation (benign, rates nearly equal, occasional capture) by the complete inability of any sinus impulse to conduct.
ECG Example - Sinus Arrest with Junctional Escape (12-lead)
Junctional escape rhythm on 12-lead ECG: Slow, regular narrow complex rhythm in all leads. No visible sinus P waves (SA node has failed). The AV junction is the sole pacemaker maintaining cardiac output. This is a medical emergency requiring urgent assessment for pacemaker implantation if the cause is irreversible. Source: LITFL
TYPE 6: Regularised AF - Digoxin Toxicity + Junctional Escape
The most dangerous and classic junctional ECG pattern
Mechanism - "AF + Complete AV Block from Digoxin = Regular Rhythm"
In atrial fibrillation, the atria fire chaotically at 400-600 bpm, and the ventricular rate is irregularly irregular. Digoxin toxicity causes complete AV block - none of the AF impulses conduct to the ventricles. The AV junction escapes and produces a regular narrow-complex rhythm at 40-80 bpm, superimposed on the chaotic AF baseline.
Atrial fibrillation: irregular baseline (400-600 bpm) → continues
Digoxin → complete AV block → NO AF impulses reach ventricles
↓
AV junction escapes: REGULAR narrow complexes at 40-80 bpm
↓
ECG paradox: IRREGULAR (fibrillatory) baseline + REGULAR QRS
= "Regularised AF" = PATHOGNOMONIC of digoxin toxicity
Rule: AF is ALWAYS irregularly irregular. If AF suddenly becomes regular - digoxin toxicity must be ruled out immediately.
Also seen: Accelerated junctional rhythm in AF toxicity = regular QRS at 70-130 bpm on fibrillatory baseline.
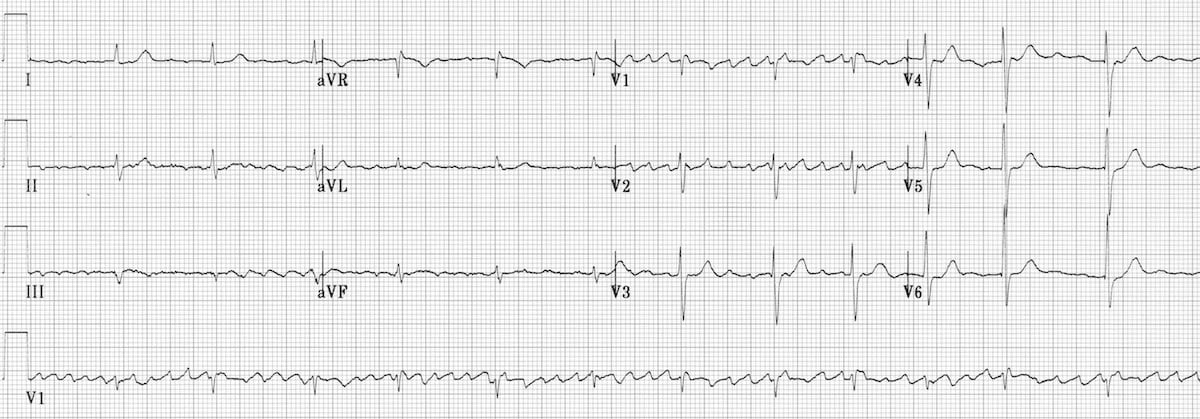
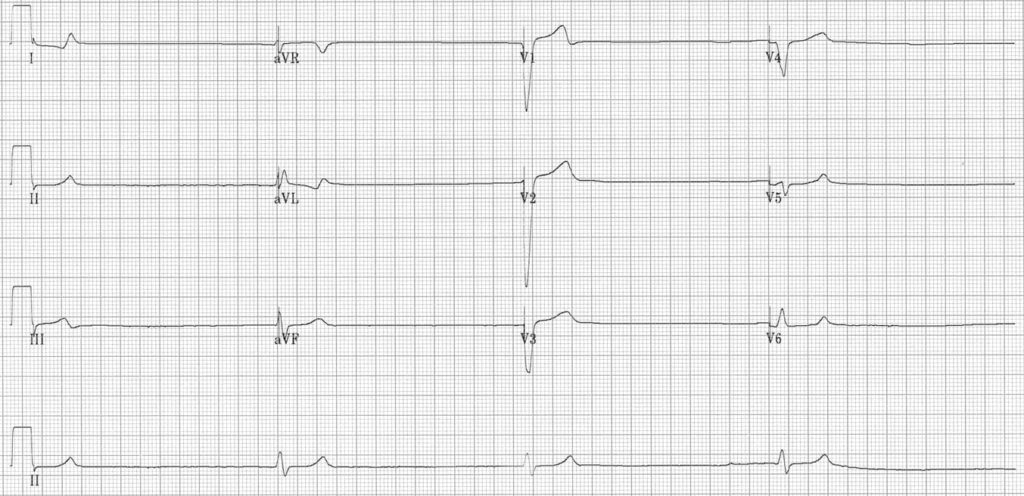
ECG Example - Regularised AF (Digoxin Toxicity, 12-lead)
Regularised AF - Digoxin toxicity (12-lead): The baseline shows coarse fibrillatory AF waves (best seen in V1 and Lead I). Despite this, the QRS complexes are completely REGULAR at ~60 bpm with narrow morphology. This paradox - AF that is regular - means complete AV block is present, with the AV junction providing an escape rhythm. STOP digoxin. Check digoxin level. Consider Digoxin Fab (Digibind) if symptomatic. Source: LITFL
SECTION 6: SIDE-BY-SIDE ECG COMPARISON
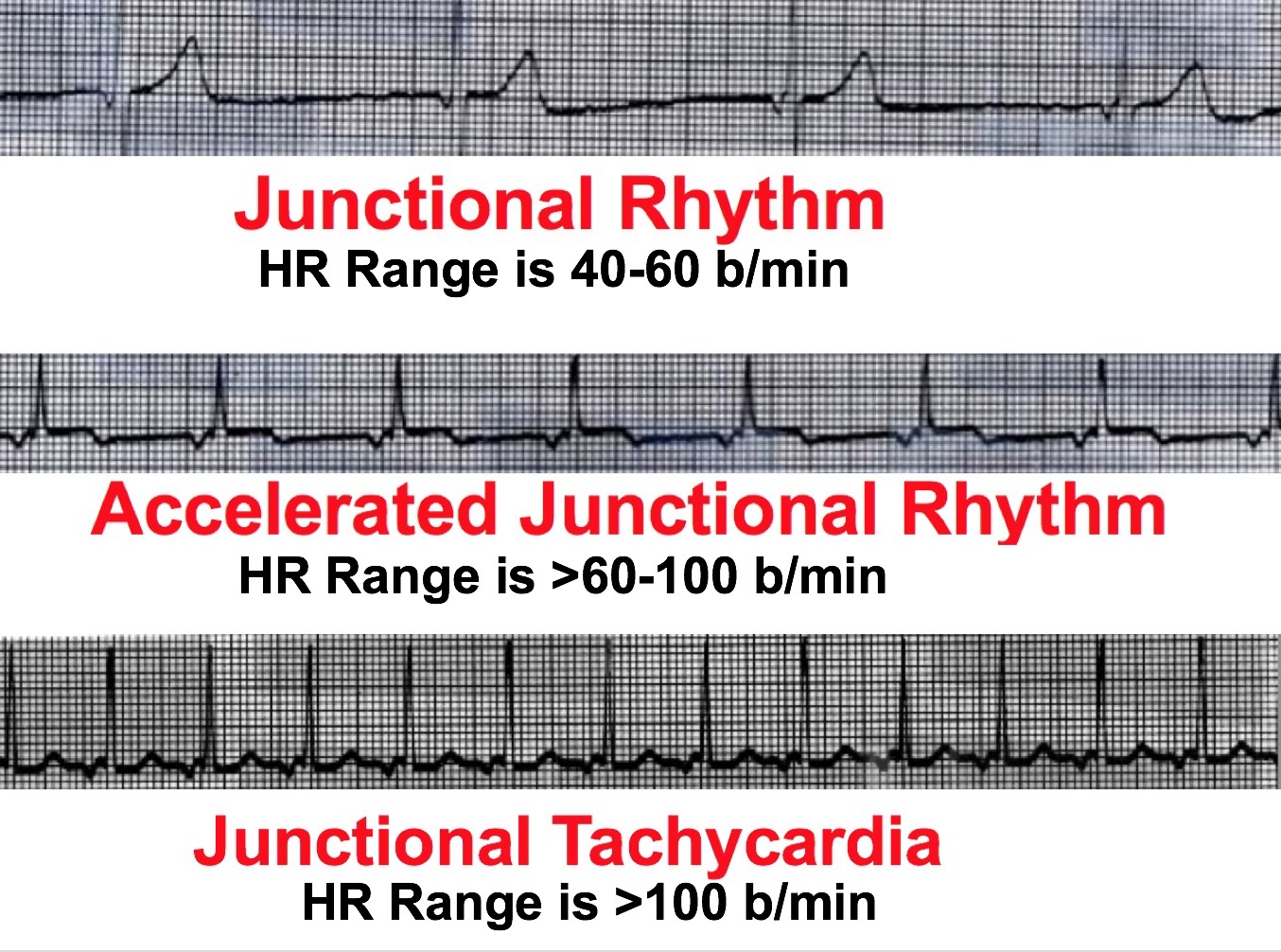
Side-by-side ECG comparison of all three main sustained junctional rhythms. All three share: narrow QRS + absent normal upright sinus P waves. What changes is only the RATE. Top (40-60): protective escape. Middle (60-100): enhanced automaticity. Bottom (>100): tachycardia. Source: UNM
SECTION 7: MASTER ECG RECOGNITION TABLE
| Feature | Junctional Escape | Accelerated Junctional | Junctional Tachycardia | PJC | Complete Heart Block |
|---|
| Rate | 40-60 bpm | 60-100 bpm | > 100 bpm | Single early beat | Junctional 40-60; sinus faster |
| Rhythm | Regular | Regular | Regular | Irregular (1 early) | Regular QRS; regular P; no relation |
| P wave | Absent or retrograde | Absent, retrograde, or AV dissociation | Retrograde (inverted II/III/aVF) | Inverted, before/within/after QRS | P present, dissociated from QRS |
| PR interval | < 0.12 s or absent | < 0.12 s or absent | < 0.12 s if P before QRS | < 0.12 s | None (no relationship) |
| QRS | Narrow | Narrow | Narrow | Narrow | Narrow (junctional escape) |
| Onset | Gradual (escape) | Gradual | Gradual (auto) / Sudden (re-entry) | Single early beat | Progressive |
| Vagal response | No change | Slight slowing | Terminates (re-entry) / Slows (auto) | N/A | No change |
| Classic cause | Inferior MI, vagal, sick sinus | Digoxin toxicity, inferior MI | Digoxin, AVNRT, post-op | Caffeine, ischemia, hypokalemia | Inferior MI, Lyme disease, digoxin |
SECTION 8: DIFFERENTIAL DIAGNOSIS
| Condition | Key ECG Differentiator |
|---|
| Sinus bradycardia | Upright normal sinus P wave before each QRS; normal PR (0.12-0.20 s) |
| Complete (3rd degree) AV block | P waves present, regular but dissociated from (slower) QRS; QRS wide if ventricular escape |
| Accelerated idioventricular rhythm (AIVR) | Wide QRS (> 0.12 s); rate 50-110; no P waves; often in MI/reperfusion |
| Atrial flutter with high block | Saw-tooth flutter waves at 250-350 bpm visible (esp. II, III, aVF, V1) |
| AVNRT | Rate 150-250; P buried in QRS or just after; pseudo-r' in V1; terminates with adenosine |
| Sinus arrest | Long pause (no P, no QRS), then escape beat |
| Atrial tachycardia | P wave present and upright but different morphology from sinus; PR normal or slightly prolonged |
SECTION 9: CLINICAL PRESENTATION
| Hemodynamic State | Symptoms |
|---|
| Asymptomatic | Incidental ECG finding; young athletes during sleep |
| Mildly symptomatic | Palpitations, fatigue, mild dizziness |
| Moderate symptoms | Near-syncope, dyspnea, reduced exercise tolerance |
| Hemodynamically significant | Hypotension, syncope, chest pain, shock |
| AV dissociation specific | Cannon A waves in JVP (atria contracting against closed AV valves), neck pounding |
Key point: Junctional rhythms may be more symptomatic than their rate suggests because retrograde atrial activation or AV dissociation causes loss of the atrial kick (which normally contributes 20-30% of cardiac output).
SECTION 10: INVESTIGATIONS
Step 1 - Immediate (All Patients)
| Investigation | Purpose |
|---|
| 12-lead ECG | Define P wave morphology, position, rate, QRS width; look for ischemia, digoxin effect |
| Rhythm strip (Lead II + V1) | Best leads for P wave visibility |
| Serum electrolytes | K+, Na+, Mg2+, Ca2+ - hypokalemia is key trigger |
| Serum digoxin level | In any patient on digoxin (toxic > 2.0 ng/mL) |
| TSH | Hypothyroidism |
| Cardiac biomarkers | Troponin, CK-MB if ischemia suspected |
| FBC/CRP | Myocarditis |
| Blood glucose | Hypoglycemia |
| ABG/SpO2 | Hypoxia and acidosis as triggers |
Step 2 - Targeted (Based on Clinical Context)
| Investigation | When to Order |
|---|
| Echocardiogram | Structural heart disease, wall motion abnormality, cardiomyopathy |
| 24h Holter monitor | Paroxysmal junctional rhythm, correlation with symptoms |
| Event recorder / implantable loop recorder | Infrequent episodes |
| Exercise stress test | Rate response to exercise; exclude ischemia |
| Coronary angiography | Inferior MI suspected |
| EP (electrophysiology) study | Persistent, drug-refractory, or re-entrant tachycardia |
| Drug/medication review | Beta-blockers, CCBs, digoxin, antiarrhythmics - dose and timing |
| Thyroid profile | Hypothyroidism screen |
| Lyme serology | Endemic area + AV block |
SECTION 11: MANAGEMENT AND APPROACH
Step 1: ABC Assessment and Hemodynamic Status
First question: Is the patient symptomatic and hemodynamically unstable?
↓
Symptomatic/Unstable Asymptomatic/Stable
(hypotension, syncope, ↓
chest pain, dyspnea) Identify cause → Treat cause
↓
Atropine IV (0.5 mg,
repeat to 3 mg total)
↓
If fails: Transcutaneous pacing
(external pads, sedation if time allows)
↓
Transvenous pacing
(definitive temporary pacing)
Step 2: Identify and Treat the Underlying Cause
| Cause | Specific Management |
|---|
| Digoxin toxicity | Stop digoxin immediately; atropine for bradycardia; Digoxin immune Fab (Digibind) for life-threatening toxicity; IV phenytoin for refractory junctional tachycardia from digoxin; Oral potassium for ectopic rhythms (if no high-grade AV block); avoid cardioversion |
| Beta-blocker excess | Hold/reduce dose; glucagon IV (1-5 mg) for reversal; calcium gluconate |
| CCB excess | Hold/reduce dose; IV calcium gluconate 1g; high-dose insulin therapy for severe cases |
| Inferior MI | IV fluids, reperfusion (primary PCI or fibrinolytics), atropine for symptomatic bradycardia, temporary pacing if needed; rhythm usually self-resolves with reperfusion |
| Electrolyte imbalance | K+ replacement for hypokalemia; Mg2+ supplementation |
| High vagal tone (athlete) | Reassure; no treatment |
| Post-cardiac surgery JET | Mild hypothermia (35-36°C), IV amiodarone, temporary atrial pacing at rate slightly above junctional rate to restore AV synchrony |
| Hypothyroidism | Thyroid hormone replacement (levothyroxine) |
| Hypoxia/acidosis | Correct oxygenation, ventilation, pH |
Step 3: Rhythm-Specific Decisions
Junctional Escape Rhythm (40-60 bpm)
- Do NOT terminate if due to SA node failure (this is the patient's only pacemaker)
- Treat underlying cause first
- Symptomatic: Atropine 0.5-1 mg IV (repeat every 3-5 min to max 3 mg) - accelerates SA node and enhances AV conduction
- Atropine fails: Transcutaneous pacing → Transvenous pacing
- Cause irreversible + bradycardia persists: Permanent pacemaker (most common indication in 3rd degree AV block or sick sinus syndrome)
Accelerated Junctional Rhythm (60-100 bpm)
- Usually well tolerated - often requires only monitoring
- Treat underlying cause (digoxin level, ischemia, electrolytes)
- No antiarrhythmic usually needed if asymptomatic
- Monitor ECG and digoxin level if digitalis-related
Junctional Tachycardia (> 100 bpm)
Re-entrant (AVNRT):
- Vagal maneuvers (Valsalva, carotid sinus massage - if no carotid disease)
- Adenosine 6 mg IV rapid push (can repeat 12 mg × 2) - terminates re-entry circuit
- Verapamil 5-10 mg IV or Metoprolol IV if adenosine fails
- Synchronized DC cardioversion if hemodynamically unstable
- Long-term: beta-blockers, CCBs, or radiofrequency catheter ablation (curative)
Automatic (enhanced automaticity):
- Treat underlying cause first
- Does not terminate with adenosine
- IV amiodarone or beta-blockers for rate control if needed
- Digoxin Fab if digoxin-related
Digoxin-toxic junctional tachycardia:
- Stop digoxin
- Digoxin immune Fab (Digibind)
- Avoid cardioversion (risk of refractory VF in digoxin toxicity)
- IV phenytoin for refractory cases
PJCs
- Isolated, infrequent: no treatment required
- Frequent/symptomatic: remove precipitants (caffeine, alcohol, electrolyte correction)
- If from structural disease: treat underlying condition
Step 4: Long-term Decisions
| Situation | Long-term Plan |
|---|
| Reversible cause corrected | No further action; ECG follow-up |
| Persistent symptomatic bradycardia (2nd/3rd degree block) | Permanent pacemaker |
| Recurrent AVNRT | Radiofrequency catheter ablation of slow pathway (> 95% curative) |
| Persistent AJR from ischemia | Revascularization + follow-up ECG |
| Sick sinus syndrome | Permanent pacemaker if symptomatic |
SECTION 12: CLINICAL APPROACH ALGORITHM
ECG shows: Regular/irregular narrow complex rhythm
with absent/inverted P waves
↓
JUNCTIONAL RHYTHM
↓
Step 1: Hemodynamics?
├─ Unstable → ABC, Atropine, Pacing
└─ Stable → proceed to Step 2
↓
Step 2: Determine TYPE by rate
├─ < 40 bpm → Junctional bradycardia (severe, needs pacing)
├─ 40-60 bpm → Junctional ESCAPE (passive, protective)
├─ 60-100 bpm → ACCELERATED junctional (active, look for cause)
└─ > 100 bpm → Junctional TACHYCARDIA (active, treat)
↓
Step 3: Identify CAUSE
├─ Digoxin on medication list? → Check level
├─ Beta-blocker / CCB? → Dose review
├─ Inferior ST elevation? → Treat MI
├─ Hypokalemia / electrolytes? → Replace
├─ Young athletic patient + vagal? → Benign, reassure
└─ Post-op cardiac surgery? → JET protocol
↓
Step 4: Treat CAUSE (primary)
↓
Step 5: Treat RHYTHM (if symptoms persist)
├─ Escape + bradycardia → Atropine → Pacing
├─ Tachycardia (re-entry) → Vagal → Adenosine → Ablation
└─ Tachycardia (automatic) → Treat cause → Amiodarone
↓
Step 6: Long-term
├─ Reversible → Follow-up ECG
└─ Irreversible + symptomatic → Permanent pacemaker
SECTION 13: SPECIAL CLINICAL NOTES
Digoxin Toxicity - Braunwald's Heart Disease
Digoxin has an extremely narrow therapeutic index (optimal trough 0.5-1.0 ng/mL). Toxicity (> 2.0 ng/mL) produces a spectrum of junctional arrhythmias:
- Ectopic junctional beats
- Accelerated AV junctional pacemaker (70-130 bpm)
- Regularised AF (complete AV block + junctional escape)
- 1st, 2nd, 3rd degree AV block
Management: Oral potassium for ectopic rhythms (even with normal K+, unless high-grade AV block); atropine for bradycardia; antidigoxin Fab fragments (Digibind) for life-threatening cases - dose calculated from estimated ingested dose or serum level.
Braunwald's Heart Disease, 2 Vol Set, p. 164
Inferior MI and Junctional Rhythm
The RCA supplies the SA node (60% of population) and AV node (90% of population). Inferior MI (RCA territory) can cause:
- Sinus bradycardia (SA node ischemia)
- Junctional escape rhythm (SA failure)
- 1st/2nd/3rd degree AV block (AV node ischemia)
These rhythm disturbances usually resolve with reperfusion (PCI/fibrinolytics). If they persist, pacemaker placement may be needed.
Frameworks for Internal Medicine, p. 29-30
Pediatric JET (Junctional Ectopic Tachycardia)
Most common post-cardiac surgery (VSD closure, AV canal repair, Fontan). Risk factors: younger age, heterotaxy, longer aortic cross-clamp time. Management: mild hypothermia (35-36°C) to slow the junctional rate, IV amiodarone, temporary overdrive atrial pacing at rate slightly faster than the junctional rate (restores AV synchrony). Congenital JET has higher morbidity/mortality than postoperative JET.
KEY POINTS SUMMARY
| Point | Detail |
|---|
| Origin | AV node or Bundle of His |
| Normal AV junction rate | 40-60 bpm |
| Core ECG hallmark | Narrow QRS + absent or inverted (retrograde) P waves |
| Why QRS is narrow | Anterograde conduction through normal His-Purkinje |
| Why P is inverted | Retrograde (bottom-to-top) atrial activation |
| Most common cause of escape | SA node suppression (vagal, MI, medications) |
| Classic drug | Digoxin toxicity |
| Classic MI | Inferior MI (RCA → SA node + AV node ischemia) |
| Never do this | Terminate junctional escape if it is the only rhythm (→ asystole) |
| Regularised AF | Digoxin toxicity + complete AV block = RED FLAG |
| First drug for symptomatic bradycardia | Atropine 0.5-1 mg IV |
| Terminating AVNRT | Adenosine 6-12 mg IV; vagal maneuvers |
| Definitive for irreversible bradycardia | Permanent pacemaker |
| Curative for recurrent AVNRT | Radiofrequency catheter ablation |
| Benign in | Young athletes with high vagal tone |
Sources: Tintinalli's Emergency Medicine (9e); Textbook of Family Medicine (9e); Morgan & Mikhail's Clinical Anesthesiology (7e); Frameworks for Internal Medicine; Harriet Lane Handbook (23e); Harrison's Principles (22e); Braunwald's Heart Disease (2 Vol Set); StatPearls NBK507715; LITFL ECG Library; eMedicine Junctional Rhythm