myocarditis. definition, epidemiology,etiology, pathogenesis, histopathology, clinical features, diagnosis, management,prognosis, complications,and differential diagnosis (table)
Reading File
Finding Sources
Searching PubMed
myocarditis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the material needed for a comprehensive, authoritative answer. Let me compile everything.
Myocarditis
1. Definition
Myocarditis is an inflammatory disease of the myocardium defined histologically by the presence of an inflammatory infiltrate with associated myocyte injury (degeneration or necrosis) not attributable to ischemia. It encompasses a diverse group of clinical entities in which infectious agents, immune-mediated processes, or toxins target the myocardium. The clinical spectrum ranges from asymptomatic ECG changes to fulminant hemodynamic collapse and sudden death.
- Fuster and Hurst's The Heart, 15th ed.
- Goldman-Cecil Medicine, International Edition
2. Epidemiology
| Parameter | Data |
|---|---|
| Incidence | 10-22 per 100,000 persons (estimated) |
| Global burden (2013) | ~1.5 million cases worldwide |
| % of heart failure hospitalizations | 0.5-4% (global hospital discharge data) |
| Prevalence at autopsy | 0.11-0.53% of all-cause deaths; 2-42% of sudden cardiac deaths in young adults |
| Age predilection | Young adults; myocarditis is 11-fold more common than atherosclerotic MI in patients age 18-29 |
| Sex | Males more commonly affected, especially for viral forms |
| Coxsackievirus myocarditis | 3.5-5% of all infected patients develop myocarditis |
| Smallpox vaccination | 5-6 per 10,000 vaccinated individuals |
| SARS-CoV-2 | Acute cardiac injury in 12-33% of hospitalized patients; myocarditis is a contributor |
| mRNA vaccine-associated | 1-10 per million (higher after 2nd dose, predominantly male adolescents/young adults) |
The true prevalence is difficult to estimate because the clinical presentation is highly variable and biopsy confirmation is not always obtained. Population estimates range from 1 in 100,000 to 1 in 10,000.
- Fuster and Hurst's The Heart, 15th ed.
- Goldman-Cecil Medicine
3. Etiology
Causes are broadly divided into infectious, immune-mediated/autoimmune, and toxic categories.
Infectious
Viral (most common in the Western world)
- Enteroviruses: Coxsackievirus A and B (historically dominant)
- Adenovirus, parvovirus B19, human herpesvirus 6 (HHV-6, increasingly detected)
- Epstein-Barr virus, cytomegalovirus (CMV), influenza A/B
- HIV (lymphocytic myocarditis, strong predictor of poor prognosis)
- SARS-CoV-2, hepatitis C, poliovirus, measles, mumps, rubella, rabies, RSV, dengue, yellow fever
Bacterial
- Corynebacterium diphtheriae, Staphylococcus, Streptococcus, Mycoplasma pneumoniae, Neisseria meningitidis/gonorrhoeae, Salmonella, Brucella, Haemophilus influenzae, Mycobacterium, Vibrio cholerae
Spirochetal
- Borrelia burgdorferi (Lyme disease), Treponema pallidum, Leptospira
Protozoal (most common cause worldwide)
- Trypanosoma cruzi (Chagas disease) - endemic in rural South/Central America; ~6 million infected worldwide, ~300,000 in the US
- Toxoplasma gondii (especially immunocompromised)
Parasitic/Helminthic
- Trichinella spiralis (most common helminthic cause with cardiac involvement)
- Echinococcus granulosus, Taenia solium
Rickettsial
- Coxiella burnetii, Rickettsia rickettsii, Rickettsia tsutsugamushi
Fungal
- Aspergillus, Candida, Cryptococcus, Histoplasma, Coccidioides, Blastomyces, Actinomyces
Immune-Mediated / Autoimmune
| Category | Examples |
|---|---|
| Systemic autoimmune | SLE, rheumatoid arthritis, scleroderma (SSc), polymyositis/dermatomyositis, Sjogren's syndrome, EGPA (Churg-Strauss) |
| Granulomatous | Cardiac sarcoidosis, giant cell myocarditis |
| Eosinophilic | Necrotizing eosinophilic myocarditis (NEM), eosinophilic granulomatosis with polyangiitis |
| Vasculitis | Kawasaki disease, Wegener's granulomatosis |
| Alloantigen-mediated | Heart transplant rejection |
| Other | Celiac disease, Whipple disease, inflammatory bowel disease |
| Drug hypersensitivity | Penicillin, sulfonamides, tetracycline, methyldopa |
Toxic
-
Drugs/chemotherapy: anthracyclines, cyclophosphamide, 5-fluorouracil, trastuzumab, interferon, interleukin-2, clozapine
-
Immune checkpoint inhibitors: ipilimumab, nivolumab, pembrolizumab, atezolizumab, durvalumab (can cause fulminant myocarditis)
-
Recreational drugs: cocaine, amphetamines, heroin, ethanol
-
Physical agents: electric shock, radiation, hyperpyrexia
-
Heavy metals: copper, iron, lead
-
Venoms: snake bite, scorpion, wasp/spider stings
-
Others: arsenic, carbon monoxide, phosphorus
-
Goldman-Cecil Medicine, Table 47-3
-
Fuster and Hurst's The Heart, Table 20-2
4. Pathogenesis
Phase 1 - Direct Myocardial Injury (Days 0-3)
Cardiotropic viruses (e.g., coxsackievirus B, parvovirus B19) enter cardiomyocytes via receptor-mediated endocytosis. Coxsackievirus B binds the coxsackievirus-adenovirus receptor (CAR). The virus replicates intracellularly and causes direct cytolytic injury, releasing danger-associated molecular patterns (DAMPs) and activating the innate immune system. Proinflammatory cytokines (TNF-alpha, IL-1beta, IL-6) are produced, recruiting natural killer (NK) cells, macrophages, and neutrophils to the myocardium.
Phase 2 - Immune-Mediated Injury (Days 4-14)
The adaptive immune response is activated. Virus-specific T lymphocytes (CD8+ cytotoxic) infiltrate the myocardium and kill virally infected cells. In genetically susceptible individuals, viral epitopes cross-react with cardiac proteins (e.g., myosin heavy chain, troponin) - molecular mimicry. This leads to production of anticardiac autoantibodies (anti-myosin, anti-beta-adrenergic receptor, anti-mitochondrial antibodies) that perpetuate myocardial inflammation even after viral clearance.
Phase 3 - Chronic/Dilated Phase (Weeks to Years)
- Ongoing autoimmune injury leads to progressive myocyte loss and replacement fibrosis
- Viral persistence in some patients maintains the inflammatory stimulus
- Results in dilated cardiomyopathy (DCM) with LV dysfunction, arrhythmias, and heart failure
- In Chagas disease, chronic immune-mediated myocarditis (with low parasite burden persisting in tissue) develops 10-20 years after acute infection
Special Mechanisms
-
Giant cell myocarditis: T-cell-mediated giant cell formation with extensive myocyte necrosis
-
Eosinophilic myocarditis: eosinophil degranulation releases major basic protein and eosinophil cationic protein, directly toxic to myocytes
-
Checkpoint inhibitor myocarditis: immune checkpoint blockade results in unregulated T-cell activation against cardiac antigens
-
Hypersensitivity myocarditis: Type IV hypersensitivity reaction, often drug-triggered, associated with eosinophilic infiltrate
-
Robbins & Kumar Basic Pathology
-
Goldman-Cecil Medicine
-
Fuster and Hurst's The Heart
5. Histopathology
Dallas Criteria (1986, still the reference standard)
Four histological patterns defined by the Dallas criteria:
| Pattern | Features |
|---|---|
| Active myocarditis | Myocyte degeneration/necrosis + definite inflammatory infiltrate ± fibrosis |
| Borderline myocarditis | Definite inflammatory infiltrate WITHOUT myocyte injury |
| Persistent myocarditis | Active inflammation on repeated biopsy |
| Resolving/Resolved myocarditis | Diminished/absent infiltrate with connective tissue healing on repeat biopsy |
Note: Dallas criteria have low sensitivity (10-20% diagnostic yield) due to patchy involvement and sampling error. Modern practice supplements with immunohistochemistry and PCR.
Gross Pathology
- Heart may appear normal or dilated
- In advanced/acute stages: myocardium is flabby, mottled with pale and hemorrhagic areas
- Mural thrombi may be present
Microscopic Features by Type
Lymphocytic myocarditis (viral)
- Edema, interstitial inflammatory infiltrates, myocyte injury
- Diffuse lymphocytic infiltrate (most common pattern)
- Often patchy - may not be sampled on endomyocardial biopsy (EMB)
- Resolves without sequelae or heals by fibrosis
Hypersensitivity myocarditis
- Interstitial and perivascular infiltrates with lymphocytes, macrophages, and a high proportion of eosinophils
Giant cell myocarditis (GCM)
- Multinucleated giant cells + extensive myocyte necrosis
- Mixed infiltrate: T lymphocytes, eosinophils, macrophages
- No granuloma formation (distinguishing from sarcoidosis)
- Fulminant course, poor prognosis
Cardiac sarcoidosis
- Non-caseating granulomas with Langhans giant cells
- Involving myocardium, conduction system
Chagas myocarditis
- Intracellular T. cruzi amastigotes within myocytes
- Inflammatory infiltrate: lymphocytes, macrophages, eosinophils
- Chronic phase: fibrosis, ventricular aneurysm (especially posterolateral LV)
SLE myocarditis
-
Small focal fibrinoid necrosis with lymphocyte/plasma cell infiltration
-
Immune complex deposition around myocyte bundles
-
Granular immunofluorescent staining with complement deposition
-
Robbins & Kumar Basic Pathology, p. 375
-
Goldman-Cecil Medicine
6. Clinical Features
The presentation ranges from entirely asymptomatic to fulminant cardiovascular collapse. Three major clinical syndromes:
A. Acute Chest Pain Syndrome (most common)
- Mimics acute coronary syndrome (ACS)
- Sharp or pressure-like chest pain, often pleuritic
- Usually preceded by a viral prodrome (1-4 weeks prior): fever, myalgias, upper respiratory illness, gastroenteritis
- Elevated troponin, ECG changes
- Normal coronary arteries on angiography
B. New-Onset Heart Failure
- Exertional dyspnea, fatigue, palpitations
- Signs of LV dysfunction: orthopnea, PND, peripheral edema
- Global or regional wall motion abnormalities on echo
C. Arrhythmic Presentation
- Palpitations, presyncope, syncope, or sudden cardiac death
- Ventricular tachycardia/fibrillation, AV block, multifocal PVCs
Fulminant Myocarditis
- Severe hemodynamic collapse requiring inotropic/mechanical support
- Paradoxically better long-term prognosis if patient survives acute phase
- Early warning signs: sinus tachycardia, narrow pulse pressure, cool/mottled extremities, elevated lactate
Symptoms and Signs Summary
| Symptom/Sign | Features |
|---|---|
| Chest pain | Sharp, pleuritic, or pressure-like |
| Dyspnea | Exertional or at rest; orthopnea |
| Fever | Common, especially with viral etiology |
| Fatigue / malaise | Universal |
| Palpitations | Due to arrhythmias |
| Syncope | Ventricular arrhythmia or complete AV block |
| S3 gallop | LV dysfunction |
| Rub | If associated pericarditis (myopericarditis) |
| JVP elevation, edema | Biventricular failure |
| Hypotension | Fulminant myocarditis |
- Fuster and Hurst's The Heart, 15th ed.
- Grainger & Allison's Diagnostic Radiology
- Goldman-Cecil Medicine
7. Diagnosis
Laboratory Investigations
- Cardiac troponin I/T: elevated (key biomarker; degree of elevation does not predict severity)
- CK-MB: elevated
- BNP/NT-proBNP: elevated if heart failure present
- ESR, CRP: elevated (non-specific inflammation)
- CBC: leukocytosis; eosinophilia in hypersensitivity/eosinophilic myocarditis
- Viral serology: rising antibody titers for specific viruses
- ANA, anti-dsDNA, ENA panel, RF, myositis immunoblot: if autoimmune etiology suspected
- Complement (C3/C4): consumed in SLE
- Blood cultures: if bacterial etiology suspected
- Borrelia serology: if Lyme disease suspected
Electrocardiogram (ECG)
- Non-specific ST-T changes (most common)
- Diffuse ST elevation (if myopericarditis)
- Sinus tachycardia
- New LBBB or RBBB
- PR prolongation, AV block (1st, 2nd, or 3rd degree)
- PVCs, non-sustained or sustained VT
- QTc prolongation
Echocardiography
- Global or regional wall motion abnormalities (may mimic STEMI)
- LV dilation, reduced ejection fraction
- Diastolic dysfunction
- Pericardial effusion (myopericarditis)
- Mural thrombus
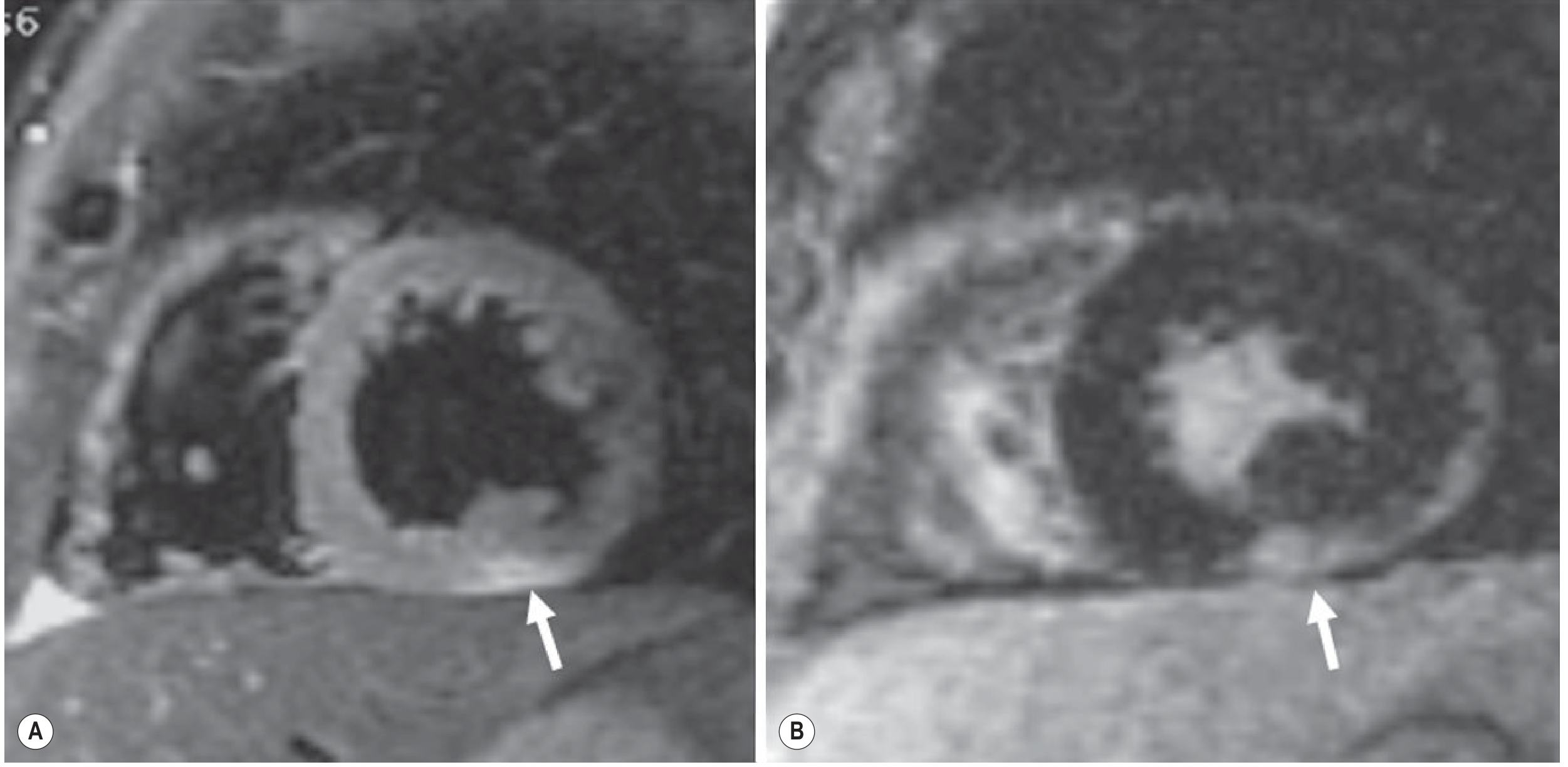
Cardiac MRI (CMR) - Key Non-invasive Diagnostic Tool
The Lake Louise Criteria (updated 2018) for CMR diagnosis of myocarditis:
| CMR Finding | Significance |
|---|---|
| T2-weighted edema (STIR sequences) | Myocardial edema/inflammation |
| Early gadolinium enhancement (EGE) | Myocardial hyperemia/capillary leak |
| Late gadolinium enhancement (LGE) | Myocardial fibrosis/necrosis - non-ischemic, subepicardial pattern, predominantly lateral/inferior wall |
| T1 mapping / T2 mapping | More sensitive parametric assessment |
Key imaging distinction: In myocarditis, LGE is subepicardial (often lateral or inferior wall). In MI, LGE is subendocardial or transmural in a coronary distribution. In Takotsubo, LGE is typically absent.
Chest X-Ray
- May be normal
- Cardiomegaly in dilated/fulminant cases
- Pulmonary congestion if heart failure present
Coronary Angiography
- Performed to exclude obstructive CAD when presentation mimics ACS
- Normal coronaries in myocarditis
Endomyocardial Biopsy (EMB)
The gold standard for definitive diagnosis, but with limitations.
Indications (ESC/AHA guidelines):
- New-onset heart failure (<2 weeks) with hemodynamic compromise (fulminant myocarditis)
- New-onset heart failure (2 weeks - 3 months) with dilated LV, new ventricular arrhythmias, Mobitz II/complete AV block, or failure to respond to standard therapy within 1-2 weeks
- Suspicion of giant cell myocarditis (rapid-onset VT or progressive HF in a young patient)
Limitations:
-
Patchy disease leads to sampling error
-
Dallas criteria sensitivity: 10-20% in some series
-
Modern approach: supplement with immunohistochemistry (CD3, CD20, CD68 T-cell/macrophage markers) and PCR-based viral genome detection (DNA/RNA extraction from biopsy)
-
Goldman-Cecil Medicine
-
Grainger & Allison's Diagnostic Radiology
-
Fuster and Hurst's The Heart
8. Management
General Principles
- Identify and remove the trigger (discontinue offending drug, treat underlying infection)
- Supportive care first in all patients
- NSAIDs are contraindicated (harmful in animal models of myocarditis; unlike pericarditis)
- Physical activity restriction: athletes should abstain from competitive sports for at least 3-6 months following acute myocarditis
A. Supportive / Heart Failure Management
| Drug Class | Indication |
|---|---|
| ACE inhibitors / ARBs | HFrEF (afterload reduction) |
| Beta-blockers (cardioselective) | HFrEF - use with caution; avoid in fulminant (negative inotropic effect) |
| Loop diuretics | Fluid overload / pulmonary congestion |
| Aldosterone antagonists (spironolactone) | Ongoing HF symptoms |
| Anticoagulation | LV thrombus, AF, eosinophilic/necrotizing myocarditis |
| Antiarrhythmics | Significant ventricular arrhythmias |
| ICD | Sustained VT, high-risk for SCD (after recovery period) |
B. Hemodynamic Support (Fulminant Myocarditis)
- Inotropic agents: dobutamine, levosimendan
- Vasopressors: noradrenaline preferred over dopamine (fewer arrhythmias)
- Intra-aortic balloon pump (IABP)
- Ventricular assist devices (VAD)
- Extracorporeal membrane oxygenation (ECMO): shown to be effective as a bridge to recovery or transplantation in fulminant myocarditis
- Cardiac transplantation: for refractory, end-stage cases
C. Immunosuppressive Therapy
| Myocarditis Type | Recommendation |
|---|---|
| Viral / idiopathic | Immunosuppression NOT routinely recommended (no mortality benefit in RCTs) |
| Giant cell myocarditis (GCM) | Immunosuppression recommended: prednisone + cyclosporine ± azathioprine |
| Cardiac sarcoidosis | Corticosteroids (prednisone) |
| Eosinophilic myocarditis / NEM | High-dose corticosteroids |
| Autoimmune (ANA+, SLE, polymyositis) | Immunosuppression (steroids + azathioprine) guided by EMB showing HLA-DR upregulation |
| Checkpoint inhibitor myocarditis | Immediate IV corticosteroids to prevent progression to fulminant myocarditis |
| Lymphocytic myocarditis refractory to standard therapy | Consider immunosuppression (prednisolone 1 mg/kg/day tapering + azathioprine 1 mg/kg/day x 90-100 days) |
Evidence note: A key RCT (Myocarditis Treatment Trial, n=111) found no mortality benefit of prednisolone + cyclosporine or azathioprine in biopsy-proven myocarditis overall. A separate RCT showed LVEF improvement with immunosuppression in patients with HLA expression on EMB, but no mortality difference at 2 years. - Goldman-Cecil Medicine
D. Specific Treatments
| Condition | Specific Therapy |
|---|---|
| Lyme carditis | Doxycycline or IV ceftriaxone; temporary pacemaker for high-degree AV block |
| Chagas disease | Benznidazole or nifurtimox (acute phase); standard HF therapy in chronic phase |
| Diphtheria | Antitoxin + antibiotics |
| Toxoplasmosis | Pyrimethamine + sulfadiazine |
| HIV myocarditis | Antiretroviral therapy (ART) |
| Antiviral therapy (viral myocarditis) | Interferon-beta (for enterovirus/adenovirus genome-positive cases) studied but not standard practice |
| IVIG | Studied in pediatric myocarditis; some benefit in acute phase |
9. Prognosis
| Outcome Group | Proportion | Features |
|---|---|---|
| Complete recovery | ~50% | Mild cases, preserved/recovered LVEF |
| Slow LV decline | ~25% | Progressive LV dysfunction over months-years |
| Rapid deterioration | ~25% | Severe LV dysfunction, transplant or death |
Predictors of Poor Prognosis
- Initial biventricular failure
- Sustained ventricular arrhythmias
- Low cardiac output at presentation
- LVEF <50% at presentation
- Syncope
- Failure to recover LV function within 6 months
Prognosis by Subtype
| Subtype | Prognosis |
|---|---|
| Lymphocytic (viral) | Generally favorable; majority recover |
| Fulminant myocarditis | Better long-term prognosis than acute non-fulminant (paradox) - if patient survives acute phase with support |
| Giant cell myocarditis (GCM) | Very poor - frequent need for transplantation or death without aggressive immunosuppression |
| Necrotizing eosinophilic myocarditis (NEM) | Very poor - frequently fatal without recognition and treatment |
| Chagas (chronic) | Progressive decline; 20-30% develop cardiomyopathy over decades |
| HIV myocarditis | Poor; mortality correlates with HIV disease stage |
| Checkpoint inhibitor myocarditis | High fatality (~25-50% if not rapidly treated) |
| Cardiac sarcoidosis | Variable; high risk of sudden death from AV block/VT |
- Fuster and Hurst's The Heart, 15th ed.
10. Complications
| Complication | Notes |
|---|---|
| Dilated cardiomyopathy (DCM) | Most important long-term complication; ~10-20% of all DCM cases preceded by myocarditis |
| Chronic heart failure | Consequence of persistent LV dysfunction |
| Ventricular arrhythmias | VT, VF - may cause sudden cardiac death; multifocal PVCs (often inferior LV origin, RBBB superior axis) |
| Sudden cardiac death (SCD) | 2-42% of SCD in young adults; arrhythmia or hemodynamic collapse |
| Complete AV block | Especially in GCM, Lyme, sarcoidosis; may require temporary or permanent pacemaker |
| Mural thrombus / thromboembolism | Due to LV stasis; systemic embolism/stroke |
| Pericarditis / Myopericarditis | Concurrent pericardial involvement |
| Right heart failure | Biventricular failure in severe cases |
| Cardiac transplantation | End-stage refractory cases |
| Arrhythmogenic substrate | LGE on CMR = persistent fibrotic scar = substrate for reentrant VT even after apparent clinical recovery |
11. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Acute MI (STEMI/NSTEMI) | CAD risk factors; obstructive coronaries on angiography; LGE subendocardial/transmural in coronary territory; ST elevation localizes to territory; older age group |
| Takotsubo (stress) cardiomyopathy | Female, post-emotional/physical stress; apical ballooning on echo; LGE typically absent on CMR; spontaneous recovery within weeks |
| Dilated cardiomyopathy (DCM) | Gradual onset; no acute inflammatory prodrome; CMR may show mid-wall LGE (not subepicardial) |
| Acute pericarditis | Pleuritic chest pain improved by sitting forward; friction rub; diffuse PR depression + ST elevation (saddle-shaped) on ECG; no or minimal troponin rise; no LV dysfunction |
| Hypertrophic cardiomyopathy (HCM) | Asymmetric septal hypertrophy; dynamic outflow obstruction; genetic testing; no inflammatory markers |
| Arrhythmogenic cardiomyopathy (ACM) | Right or biventricular involvement; fatty infiltration on CMR; desmosomal gene mutations; epsilon waves, LBBB-morphology VT |
| Cardiac sarcoidosis | Non-caseating granulomas on EMB; FDG-PET shows patchy uptake; hilar adenopathy on CXR/CT; AV block; may coexist with systemic sarcoidosis |
| Giant cell myocarditis | Rapid-onset severe HF + VT/AV block in young patients; requires EMB for diagnosis (giant cells); no granulomas |
| Lyme carditis | Endemic exposure; tick bite history; Borrelia serology positive; predominant conduction system disease (AV block); less severe LV dysfunction |
| Septic cardiomyopathy | Context of systemic sepsis/bacteremia; diffuse LV depression; no specific inflammatory infiltrate on biopsy; improves with treatment of infection |
| Peripartum cardiomyopathy (PPCM) | Last month of pregnancy or within 5 months postpartum; LV dilatation; may have autoimmune component |
| Cardiac amyloidosis | Restrictive pattern; increased wall thickness with "sparkling" echo; low-voltage ECG; specific LGE pattern (diffuse subendocardial); Congo red staining on biopsy |
| Acute rheumatic fever | Young patient; preceding Group A streptococcal pharyngitis; Jones criteria; mitral/aortic valvular involvement; elevated ASO titers |
| Drug toxicity (anthracyclines) | History of chemotherapy; cumulative dose-dependent cardiotoxicity; no inflammatory infiltrate on biopsy |
Key Sources
- Fuster and Hurst's The Heart, 15th Edition (Chapter 20)
- Goldman-Cecil Medicine, International Edition (Chapter 47)
- Robbins & Kumar Basic Pathology (p. 375)
- Grainger & Allison's Diagnostic Radiology
- Braunwald's Heart Disease, A Textbook of Cardiovascular Medicine
This is a shared conversation. Sign in to Orris to start your own chat.