I now have comprehensive information from textbooks. Here is the complete structured answer:
Carcinoma of the Maxillary Sinus — Comprehensive Answer
a) Most Probable Diagnosis & Histopathological Types (4 marks)
Most Probable Diagnosis: Carcinoma of the Maxillary Sinus (Maxillary Antrum)
The clinical triad in this patient — a chronic tobacco chewer with unilateral nasal obstruction, blood-stained discharge, loosening of upper teeth, facial swelling, cheek fullness, infraorbital hypoesthesia, diplopia, and a proliferative middle meatus growth — is classic for advanced malignancy of the maxillary sinus.
Histopathological Types (in order of frequency):
| Type | Frequency | Notes |
|---|
| Squamous Cell Carcinoma (SCC) | ~80% | Most common; directly linked to tobacco use |
| Adenocarcinoma | ~10% | Associated with wood dust, nickel, chromium exposure |
| Adenoid Cystic Carcinoma | ~5% | Predilection for perineural spread |
| Undifferentiated Carcinoma | Rare | Aggressive, poor prognosis |
| Melanoma | Rare | Tends to remodel rather than destroy bone |
| Lymphoma / Plasmacytoma | Rare | Often remodel bone |
| Sarcoma / Rhabdomyosarcoma | Rare | More common in children |
| Esthesioneuroblastoma | Rare | Arises from olfactory neuroepithelium |
— Cummings Otolaryngology Head and Neck Surgery; K J Lee's Essential Otolaryngology
b) Clinical Features According to Direction of Spread (6 marks)
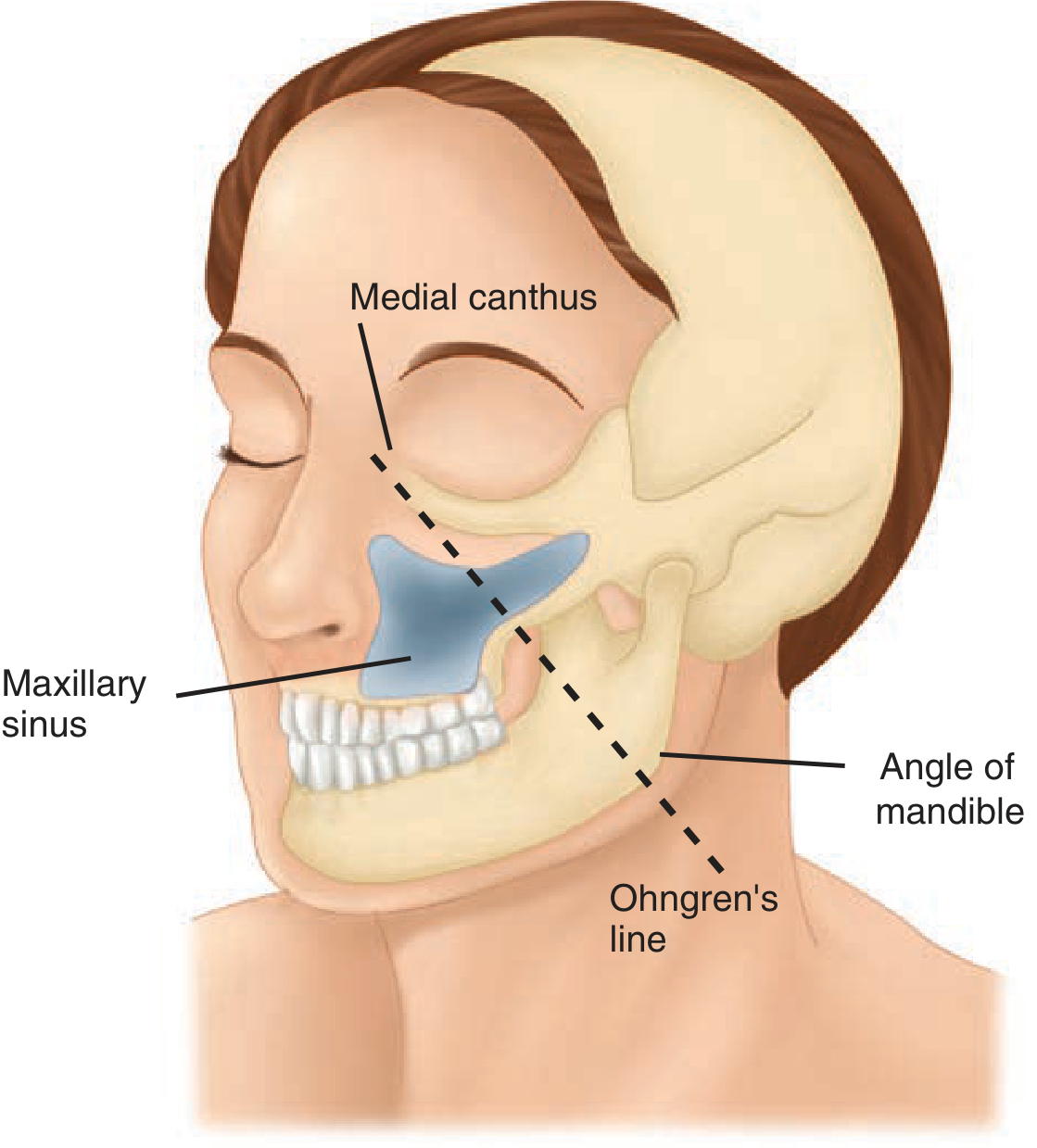
The maxillary sinus has six walls and tumor spread produces distinct symptom clusters depending on which wall is breached. Ohngren's line — drawn from the medial canthus of the eye to the angle of the mandible — divides the maxillary sinus into a superoposterior (infrastructure-poor, suprastructure-rich) portion with poor prognosis and an anteroinferior portion with better prognosis.
Ohngren's line — from medial canthus to angle of mandible — Schwartz's Principles of Surgery
1. Medial Wall → Nasal Cavity
- Unilateral nasal obstruction (present)
- Blood-stained / purulent nasal discharge (present)
- Proliferative growth visible in the middle meatus (present)
- Epiphora (nasolacrimal duct involvement)
2. Inferior Wall → Oral Cavity / Hard Palate
- Loosening and displacement of upper molar/premolar teeth (present)
- Ill-fitting dentures
- Palatal swelling, ulceration, or perforation
- Trismus (if pterygoid plates involved)
3. Anterior Wall → Cheek / Face
- Fullness and swelling of the cheek (present)
- Palpable bony hard mass over cheek
- Skin infiltration (late sign)
4. Superior Wall → Orbital Floor
- Proptosis / upward displacement of the globe
- Diplopia (present) — due to infraorbital nerve / inferior rectus involvement
- Infraorbital hypoesthesia / anesthesia (present) — infraorbital nerve compression
- Epiphora from nasolacrimal duct obstruction
5. Posterior Wall → Pterygopalatine Fossa / Infratemporal Fossa
- Trismus (pterygoid muscle invasion)
- Referred otalgia
- Numbness over the cheek, upper lip (V2 involvement)
- Swelling in the temporal fossa
6. Superior–Posterior Extension → Skull Base / Orbit / Brain
- Proptosis
- Visual disturbance / blindness (optic nerve)
- Cavernous sinus syndrome (III, IV, VI cranial nerve palsies)
- Intracranial involvement → headache, seizures (late)
Lymph Node Spread
- Submandibular (Level I) and upper jugular (Level II) nodes most commonly involved
- Occurs in ~25% of sinonasal malignancies at presentation
- Retropharyngeal nodes also at risk
— Cummings Otolaryngology Head and Neck Surgery, p. 794; K J Lee's Essential Otolaryngology
c) Investigations for Diagnosis and Their Justification (5 marks)
1. CT Scan of Paranasal Sinuses (with contrast) — FIRST-LINE
- Role: Evaluates bony erosion and destruction of sinus walls, orbital floor, hard palate, pterygoid plates, anterior skull base
- CT is superior to MRI for bone integrity assessment
- Identifies extent of bony involvement for surgical planning
- T-staging: determines T1–T4 classification (AJCC)
- Detects cervical lymphadenopathy
2. MRI of Paranasal Sinuses (with gadolinium) — COMPLEMENTARY / SUPERIOR for SOFT TISSUE
- Role: Differentiates tumor from trapped/obstructed secretions (tumor shows lower T2 signal; secretions show high T2)
- Superior to CT in 94–98% correlation with surgical findings
- Assesses perineural spread (critical for adenoid cystic carcinoma)
- Detects orbital fat invasion, dural involvement, intracranial extension
- Evaluates cavernous sinus involvement
- Irregular dural thickening >5 mm with enhancement = 100% PPV for dural invasion
3. Biopsy (Histopathological Examination) — DEFINITIVE
- Route: Endoscopic biopsy via nasal cavity / transoral if palatal involvement
- Role: Confirms malignancy, establishes histological type (SCC vs adenocarcinoma vs adenoid cystic etc.)
- Guides choice of chemotherapy and radiation protocol
- Tissue marker studies: p40/p63 (SCC), CK7/CK20, S100 (melanoma), CD20/CD3 (lymphoma), synaptophysin (neuroendocrine)
4. Nasal Endoscopy
- Role: Direct visualisation and assessment of extent of nasal cavity and middle meatus involvement
- Allows guided biopsy
- Assesses resectability and medial extent
5. OPG (Orthopantomogram) / Dental X-ray
- Role: Assesses degree of upper alveolar/molar tooth involvement and mandibular integrity
- Useful before surgery for dental rehabilitation planning
6. Chest X-ray / CT Chest
- Role: Screens for pulmonary metastases (distant spread)
- Part of staging workup
7. PET-CT (if available)
- Role: Detects occult nodal and distant metastases
- Guides radiation field planning
8. Blood Investigations
- CBC, LFT, RFT — baseline before chemotherapy/surgery
- Serum calcium — if bony involvement extensive
— Cummings Otolaryngology Head and Neck Surgery, p. 793–795; K J Lee's Essential Otolaryngology
d) Management (Medical + Surgical Indications) (marks)
Management of maxillary sinus carcinoma is multimodal — surgery forms the cornerstone, combined with radiotherapy and/or chemotherapy.
STAGING (AJCC T-Classification — Maxillary Sinus)
| Stage | Description |
|---|
| T1 | Limited to maxillary sinus mucosa, no bony erosion |
| T2 | Bone erosion including hard palate / middle meatus (not posterior wall or pterygoid plates) |
| T3 | Posterior wall maxillary sinus, subcutaneous tissues, orbital floor/medial wall, pterygoid fossa, ethmoid sinus |
| T4a | Anterior orbital contents, skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid/frontal sinuses |
| T4b | Orbital apex, dura, brain, middle cranial fossa, cranial nerves other than V2, nasopharynx, clivus |
(T4b = unresectable)
MEDICAL MANAGEMENT
1. Induction Chemotherapy (Neoadjuvant)
- Platinum-based regimens: Cisplatin + 5-Fluorouracil (PF) or TPF (Docetaxel + Cisplatin + 5-FU)
- Used in locally advanced / borderline resectable disease to downstage tumor
- Facilitates organ preservation (orbit, palate)
2. Concurrent Chemoradiation
- Cisplatin (100 mg/m² every 3 weeks) concurrent with radiation
- Used postoperatively when adverse features present (positive margins, perineural invasion, nodal involvement with extracapsular spread)
- Also used as primary definitive treatment in unresectable T4b disease
3. Targeted Therapy
- Cetuximab (anti-EGFR): Used in recurrent/metastatic SCC when cisplatin is contraindicated
- Pembrolizumab / Nivolumab (PD-1 inhibitors): For recurrent/metastatic disease, especially PD-L1–positive tumors
4. Radiation Therapy (RT)
- Definitive RT: For unresectable disease or patients unfit for surgery
- Dose: 60–70 Gy in conventional fractionation
- Modern techniques: IMRT (intensity-modulated RT) reduces dose to orbit, brain, optic structures
- Postoperative adjuvant RT: 60–66 Gy, started within 6 weeks of surgery
SURGICAL MANAGEMENT
Surgery is the primary treatment for resectable disease. Choice of procedure depends on extent of tumor and Ohngren's classification.
Indications for Surgery:
- Resectable T1–T4a disease without involvement of orbital apex, dura, brain, or clivus
- T4b features (orbital apex, dura, brain) generally render the tumor unresectable
- Orbital exenteration is indicated when orbital fat is invaded; periorbita alone does not require exenteration
A. Infrastructure Maxillectomy (below Ohngren's line)
- Removes: floor and walls below the infraorbital nerve
- Indications: T1–T2, tumors confined to lower half of maxillary sinus, alveolus, palate
- Approach: transoral / sublabial
B. Total Maxillectomy (Total / Radical)
- Removes: entire maxilla including orbital floor
- Indications: T2–T3, tumors involving the full sinus
- Approach: Weber-Ferguson incision (lateral rhinotomy extended below the nostril, through upper lip to gingival sulcus)
- May include orbital floor resection; orbital contents preserved if periorbita intact
C. Total Maxillectomy + Orbital Exenteration
- Indications: Tumor invading orbital fat (not just bony orbit)
- Radical procedure; significant functional and cosmetic deficit
D. Craniofacial Resection
- Indications: Tumor involving cribriform plate or anterior skull base
- Combined neurosurgical + ENT approach
- Removes ethmoids, cribriform plate, sometimes dura
E. Neck Dissection
- Selective neck dissection (levels I–III) indicated when clinically node-positive
- Elective neck dissection considered for N0 neck when tumor > T2 (high occult nodal risk)
RECONSTRUCTION
- Prosthetic obturator: for palatal defects after maxillectomy
- Free flaps (anterolateral thigh, rectus abdominis): for large soft tissue defects
- Titanium mesh / orbital implants for orbital floor reconstruction
SUMMARY ALGORITHM
Biopsy-proven maxillary sinus carcinoma
↓
Staging (CT + MRI + CXR ± PET-CT)
↓
┌──────────────────────────────────┐
│ Resectable (T1–T4a) │ Unresectable (T4b)
│ │
│ Surgery (Maxillectomy) │ Concurrent chemoradiation
│ + Postop RT ± Chemo │ or palliative chemotherapy
└──────────────────────────────────┘
— Cummings Otolaryngology Head and Neck Surgery; K J Lee's Essential Otolaryngology; Schwartz's Principles of Surgery 11th Edition
Key Teaching Points for This Case
- The diplopia + infraorbital hypoesthesia indicate superior wall / orbital floor breach (T3 at minimum)
- Loosening of teeth = inferior wall involvement
- Cheek fullness = anterior wall erosion
- This patient has spread in ≥3 directions → likely T3 or T4a disease
- Most patients present with advanced disease because the sinus acts as a "silent" compartment in early stages