SCROTUM HISTORY 1. Age: Carcinoma of the skin of the scrotum is a disease of individuals above 50 years of age. But malignant condition of the testis is common in young individuals-teratoma between 20 and 30 years, whereas seminoma between 30 and 40 years. Torsion of the testis is commonly seen in teen-aged boys. Hydrocele is seen even in infants, but the primary hydrocele is most common over the age of 40 years. While the secondary hydrocele is commoner between 20 and 40 years of age. Tuberculous orchitis is the disease of the young. Majority of the epididymal cysts and spermatoceles occur in men above 40 years of age. Cysts of the epididymis, though congenital, appear in the middle-aged men. 2. Occupation: Except carcinoma of the scrotal skin, other conditions do not have a definite relation with occupation. The former condition is often caused by frequent contact with soot (chimney sweep's cancer), tar or oil (mule spinner's cancer). The skin is exposed to these irritants for many years before a cancer develops. Varicocele often develops in men who are involved in work which requires prolonged standing (Bus conductors, etc.). 3. History of present illness: Malignant growth of the testis often grows silently without the knowledge of the patient and in fact he may present a lump in the epigastric or umbilical region due to secondary deposits in the lymph nodes. A history of trauma followed immediately by a swelling is the usual history of a hematocele, which maintains this size for a long time. In torsion of the testis an exciting cause is almost always present like straining at stool, lifting a heavy weight or coitus. This is due to violent contraction of the spirally attached cremaster muscle, which favors rotation of the testis around a vertical axis. Acute epididymo-orchitis begins with an ache in the groin and slight rise of temperature. This is followed by severe pain, a considerable rise of temperature with redness and swelling of the scrotum. In filariasis periodic attacks of fever, pain and swelling of the spermatic cord and scrotum are the main features. In tuberculous epididymitis, a slight ache or a trivial injury call the patient's attention towards the testis. Injury to the bulb of the urethra or bursting of a periurethral abscess-a complication of gonococcal stricture is the usual history of extravasation of urine. In gummatous orchitis, a trivial injury calls the patient's attention towards the already diseased testis. asked By this to the tis can tum ng of dix 5 LOCAL EXAMINATION A. INSPECTION 1. Skin and subcutaneous tissue: The skin of the scrotum is usually wrinkled and freely mobile over the testis. It becomes red and edematous in case of acute epididymo-orchitis In hydrocele the skin will be tense, so the normal rugosity of the skin will be lost and subcutaneous veins will be prominent. Normal rugosity of the skin will also be lost in presence of underlying pathology such as tuberculous epididymitis, gummatous orchitis, teratoma and seminoma of the testis, in an otherwise normal size scrotum. Multiple sebaceous cysts are not uncommon in scrotal skin (Figs. 40.1 and 40.2). Their features will be similar to sebaceous cyst anywhere in the body (see Page 57). Carcinomatous ulcers may occur anywhere in the scrotum but the industrial cancers are common in the cleft between the scrotum and the thigh. These ulcers are small and circular with everted edge. The floor is covered with yellowish-gray infected necrotic tissue. Ulcers usually discharge offensive, purulent or serosanguineous fluid. It must be remembered that gummatous ulcer of the scrotum resulting from extension of a gumma of the testis lies always on the anterior aspect of the scrotum. Tuberculous ulcer resulting from tuberculous epididymitis is always seen on the posterior aspect of the scrotum. These positions are reversed if the testis is anteverted. In severe infection the testis may protrude through the scrotum and appear as a granulating mass, which is known as hernia testis. Rarely the patient may present with gangrene of the scrotum for which no cause can be found out. This is known as Fournier's gangrene (idiopathic gangrene). If there are multiple sinuses one should suspect 'Watering can' perineum. One must remember that edema of the scrotum and penis may occur in medical conditions like nephritis, heart failure, etc. The surgical causes are cellulitis, filariasis, blocking of lymph vessels by cancer cells or following block dissection of inguinal lymph nodes and extravasation of urine. In case of extravasation of urine look at the perineum for evidence of injury or presence of periurethral abscess which bursts spontaneously to allow the urine to extravasate (Fig. 40.3). A few cases of cellulitis of scrotum is misdiagnosed as suppurated hydrocele. Thickening of the skin and subcutaneous tissues of the scrotum may be so enormous that the scrotum assumes the size of a watermelon (elephantiasis of the scrotum), the penis becomes buried in the scrotal swelling (Figs. 40.4 and 40.5). The skin and subcutaneous tissues of the penis may be similarly thickened to produce the typical 'Ram's Horn' penis in filariasis (Fig. 40.6). Another manifestation of filariasis is lymph scrotum in which the skin of the scrotum shows excessive rugosity with vesicles containing fluid (lymph) (Fig. 40.7). Rupture of these vesicles from friction will lead to profuse exudation of lymph (lymphorrhagia). 2. Swelling: Slight swelling of the scrotum is evident by loss of normal rugosity of the scrotum. This is seen in any infection of testis and epididymis. Other conditions like cysts of the epididymis, spermatocele, etc., do not produce obvious swelling on inspection. Hydrocele may bring forth various degrees of swelling of the scrotum-small to very big so as to hang up to knee level. A peculiar constriction is often found Fig. 40.7: Lymph scrotum with vesicles around the swelling. If the hydrocele is tense it tends to stand out (forward projection). Note the size, shape and extent of the swelling. Does it extend up along the spermatic cord to the groin? 3. Impulse on coughing: Many a time hydrocele is associated with hernia-a bubonocele or a complete inguinal hernia. Hernia shows impulse on coughing. So this part of examination cannot be dispensed with. B. PALPATION That the swelling is purely scrotal is confirmed by getting above the swelling. 1. Skin: If there is an ulcer, palpate it thoroughly as described in Chapter 4. A carcinomatous ulcer of the scrotum is diagnosed by yellowish-gray slough on the floor, hard base and everted margin. In the early stage the ulcer is freely mobile, but if the malignant ulcer becomes tethered to the underlying testis, it becomes fixed and moves with the testis. At this stage it is difficult decide whether the lesion is a primary skin cancer or a testicular tumor ulcerating through the skin. An anteriorly placed ulcer which is fixed to the testis is probably a gummatous ulcer, whereas a posteriorly placed ulcer which is fixed to the epididymis is a tuberculous ulcer. The testis cannot be separated from the protruded necrotic mass in case of hernia testis, but the testis can be easily separated in hernia of a hydrocele. Edema of the scrotum will 'pit on pressure: 2. Swelling: This is first examined in the usual line as discussed in Chapter 3, noting temperature, tenderness, extent, size, shape, surface, margin and is a vaginal hydrocele. Le.. a collection of scrous fluid in the tunica vaginalis (Fig. 40.8). The two cardinal signs of a hydrocele are: fluctuation and consistency. The most common cystic swelling translucency. FLUCTUATION (Fig. 40.9): This test cannot be performed in the traditional way, as the whole scrotum is very much mobile. So this test is performed by holding the upper pole of the scrotal swelling between the thumb and the fingers of one hand to make the swelling tense and steady, while intermittent pressure is applied at the lower pole with the thumb and the fingers of the other hand. This will push the fluid inside the tunica vaginalis upwards, the thumb and the fingers holding the upper pole of the swelling will be pushed apart from each other making this test positive. TRANSLUCENCY (Figs. 40.10 and 40.11): This test is best performed in darkness. A pencil torch is placed laterally over the swollen scrotum. A red glow will be seen throughout the scrotum indicating presence of clear fluid inside the scrotum. This can be better visualized through a roll of paper placed on the other side of the scrotum even in day light. The common mistake the students often make is to place the torch on the posterior aspect of the scrotum and the roll of paper anteriorly. The testis comes in the way of the light and this test becomes false negative. Uncomplicated hydrocele and the cyst of the epididymis are translucent but spermatocele is not translucent as the fluid it contains is not clear. REDUCIBILITY: This is tested by raising the scrotum and compressing the swelling gently. Congenital hydrocel, and a varicocele are reducible. In case of the former always examine the abdomen for ascites as congenital hydrocele is often associated with tuberculous peritonitis IMPULSE ON COUGHING: Many a time scrotal swelling may be associated with a hernia, varicocele or lymph varix. The root of the scrotum is held and the patient is asked to cough. An impulse either expansile in nature (hernia or congenital hydrocele) or thrill-like (varicocele or lymph varix) may be obtained. If this test is omitted, these conditions may be missed and treatment will be incomplete. 3. Testis: Examination of a scrotal swelling cannot be complete without palpation of the testis, epididymis and spermatic cord. Note its position, size, shape, surface, consistency, weight, mobility and testicular sensation. Note the position of the testis-whether normal, anteverted (the epididymis lies anteriorly and the body lies posteriorly), completely inverted, i.e., upside down (the globus major lies inferiorly) or incompletely inverted, i.e., the testis lies horizontally. These latter two positions predispose torsion of the testis. Whether the testis is normal in size, larger, or smaller than normal size? Smaller testis is an underdeveloped testis. Larger testis is often pathological-gummatous or with a tumor. Whether the surface is smooth or nodular? Whether the consistency is uniform or heterogenous? Note the weight of the organ in respect of its size. This is done by balancing the testis on the palm of the hand. The testis becomes relatively heavy in a case of neoplasm and old hematocele, but is comparatively light in a gumma of the testis. Testicular sensation is very important. This is a peculiar sickening sensation felt by the patient when a mild pressure is applied on the testis. In gumma and malignant tumor of the testis, the testicular sensation quickly dwindles away (more so in case of gumma). In case of malignancy one should be very gentle and should not squeeze roughly lest the malignant cells should be dislodged and thrown into the venous and lymphatic channels. It must be remembered that testis may be absent from the scrotum (in undescended testis, ectopic testis and retractile testis). The testis is mainly affected in mumps, syphilis and neoplasm. 4. Epididymis: This is normally felt as a firm nodular structure attached to the posterior aspect of the testis. Its large upper part is known as head (globus major), the middle part as body and the lower as tail (globus minor). Epididymis is mainly affected in tuberculosis, filariasis and acute (both gonococcal and nongonococcal) epididymo-orchitis. In tuberculosis the globus minor is first affected (the infection being mostly retrograde) and becomes enlarged, nodular and slightly tender. Only in blood-borne infection the globus major may be involved first. Gradually, the whole epididymis becomes enlarged, firm, craggy and slightly tender. Softening of the epididymis and formation of cold abscess in the posterior aspect of the scrotum is a great diagnostic point in favor of tuberculosis. In filariasis the epididymis also enlarges and becomes firm. Acute reflux epididymitis and postoperative epididymitis following prostatectomy) or from mumps. Remember syphilis attacks the testis and tuberculosis affects the epididymis. Later on in both these conditions the disease spreads to the other organ. In filariasis, both the testis and epididymis are simultaneously involved. 5. Spermatic cord: This is best palpated at the root of the scrotum between the thumb and the index finger simultaneously on both sides. The vas deferens will be felt as hard whipcord slipping between the thumb and the index finger. Besides the vas, the fingers normally feel a number of strings, which are nothing but fibers of cremaster muscle. The spermatic cord is thickened and tender in any inflammatory condition of the epididymis either acute or chronic. The vas is thickened and beaded in tuberculous epididymitis. The cord is not affected in syphilis but becomes thickened and slightly tender in filariasis. Lymph varix is also a feature of filariasis. A lymph varix feels soft and doughy whereas a varicocele feels like a 'bag of worms. Both these conditions will yield a thrill-like impulse on coughing, but a varicocele more readily reduces than a lymph varix. In malignancy of the testis the growth may be extended upwards along the cord. In this case the cord will feel hard and nodular. 6. Lymph nodes: It is an extremely important part of examination. The skin of the scrotum drains into the inguinal group of lymph nodes whereas the testis and epididymis drain into the pre- and para-aortic lymph nodes at the level of the origin of the testicular artery from the aorta, i.e., at the transpyloric plane. These groups of lymph nodes must be palpated (Fig. 40.12). The left supraclavicular group of lymph nodes may be involved as in case of malignancies in other abdominal organs by lymphatic spread of malignant cells along the thoracic duct. epididymo-c philitic or Urine shou Acute epidi Ecoli, Strep epididymiti Chest X-ray ofpulmona cases of tes Intravenou act posit so to det brought ab Lymphang the para-a shrinkage Aschhe and huma level (100 Inow whe secondar Aspiration fluid is m hydrocel of 1.022-case of se better pa bydrocel Prostati epididym architis. Fig. 40.12: A lump in the epigastric region of the abdomen from secondary deposits in the lymph nodes from malignant growth of the testis. GENERAL EXAMINATION Lungs should be examined particularly in case of tuberculous epididymo-orchitis to exclude tuberculous affection of the lung and malignancy of the testis to exclude secondary deposits in the lung. One should look for other syphilitic stigmas (see page 67) in cases of gummatous orchitis. Kidneys should be examined in cases of tuberculous epididymitis and varicocele of recent onset. In about 60% of cases there is either active tuberculosis in the renal tract or evidence of previous disease. Varicocele may be a sequel to adenocarcinoma of the kidney of the same side. Rectal examination should always be performed in epididymo-orchitis either acute or chronic. Acute prostatitis often precedes epididymo-orchitis. The seminal vesicles are often enlarged and tender in cases of tuberculous epididymitis. HYDROC This car classifie cong commu small fo gradual opening endude SPECIAL INVESTIGATIONS Blood should be examined for eosinophilia and microfilaria in filariasis. Lymphocytosis and increased erythrocyte sedimentation rate (ESR) may be seen in cases of tuberculous epididymo-orchitis. Positive Wassermann reaction (WR) and Kahn tests favor the diagnosis of Urine should be examined as a routine in cases of acute and chronic epididymo-orchitis Acute epididymitis often results from retrograde passage of infected urine and presence of E. coli, Streptococcus, Staphylococcus or even proteus may be detected in urine. In tuberculous epididymitis many a time one will find tubercle bacilli in the urine. of pulmonary tuberculosis. This is also important to exclude secondary deposits in the lungs in Chest X-ray is an important investigation in tuberculous epididymo-orchitis to exclude presence cases of testicular tumors particularly the teratomas. Intravenous pyelography should also be performed in cases of testicular tumors to know the exact positions of the kidneys so that they may be properly shielded during radiotherapy and also to detect retroperitoneal lymphatic metastasis that might have displaced the ureters or brought about deformity of the renal pelvis, Lymphangiography is an important part of investigation to determine secondary deposits in the para-aortic lymph nodes which have not shown clinical enlargement. Its value in assessing shrinkage of enlarged nodes by radiotherapy is also great. Aschheim-Zondek test will be positive in cases of Sertoli cell tumor (interstitial cell tumor) and human chorionic gonadotrophin in 12-hour collection of urine will be higher than normal level (100 iu) in chorion carcinoma (malignant teratoma trophoblastic) of the testis. Ultrasonography is extremely helpful not only to know the position of the testis, but also to know whether they are normal or not. This investigation is helpful in hydrocele, hematocele, secondary hydrocele, torsion of testis, etc. Aspiration of a cystic swelling may clinch the diagnosis in a spermatocele or chylocele. The fluid is milky in spermatocele but in case of the cyst of the epididymis the fluid is clear. In hydrocele an amber color fluid may be obtained whose specific gravity remains in the range of 1.022-1.024; it contains water, inorganic salts, cholesterol, fibrinogen and 6% of albumin. In case of secondary hydrocele from testicular tumor the fluid will be blood stained. To facilitate better palpation of testis and epididymis fluid should be aspirated out in case of secondary hydrocele. Prostatic massage may demonstrate presence of gonococci în cases of acute gonococcal epididymo-orchitis and may demonstrate tubercle bacilli in cases of tuberculous epididymo- Orchitis HYDROCELE This can be classified into congenital and acquired varieties. Acquired variety can be further classified into primary (idiopathic) and secondary (from diseases of the testis and epididymis). In congenital hydrocele (Fig. 40.13), the processus vaginalis remains patent and it freely communicates with the peritoneal cavity. But usually the communicating orifice remains too small for hernia to develop. This condition is mainly diagnosed by the fact that the hydrocele gradually disappears when the patient lies down but it returns in the erect posture. The small opening prevents emptying of the hydrocele by digital pressure. In bilateral cases one should exclude ascites from tuberculous peritonitis. Primary hydrocele is mostly seen in middle-aged men but occasionally it is seen in early childhood. This may be unilateral or bilateral. The main and only complaint is the swelling of the scrotum and that is why the patient often presents with enormous swelling. One can 'get above the swelling' if it is a pure hydrocele, the only exception is the infantile hydrocele. The color and temperature of the overlying skin are normal. Primary hydrocele is not tender but secondary hydrocele may be tender. It is dull on percussion in contradistinction to the hernia, which is often resonant (due to presence of intestine inside the hernial sac). The fluid of the hydrocele surrounds the body of the testis making the testis impalpable. If one can feel the testis separate from the scrotal swelling then the swelling is not a hydrocele but may be a cyst of the epididymis or spermatocele. In about 5% of cases inguinal hernia is associated with this condition. So one should not omit to look for impulse on coughing. The diagnosis of hydrocele is made by fluctuation and translucency te I want in detail and simifief version of hydrocele ...history local examination general examination investigations and complications differential diagnos
HYDROCELE - Complete Clinical Guide
DEFINITION
TYPES / CLASSIFICATION
| Type | What happens | Key feature |
|---|---|---|
| Congenital (Communicating) | Processus vaginalis stays open; peritoneal fluid flows freely into scrotum | Disappears when lying down, reappears on standing |
| Primary (Idiopathic) | Processus is closed; fluid accumulates from imbalance of production vs. absorption | Most common; middle-aged men; painless |
| Secondary | Caused by underlying disease (infection, tumor, trauma, torsion) | Tender; men >40 yrs; always investigate cause |
| Infantile | Mid-portion of processus open; communicates with tunica but not peritoneum | Presents in infancy/childhood |
| Hydrocele of the Cord | Isolated cyst along the spermatic cord | Oval swelling above the testis |
HISTORY
A. Age
- Primary hydrocele: Most common in men >40 years
- Secondary hydrocele: More common between 20-40 years (due to underlying conditions like epididymo-orchitis or tumor)
- Congenital hydrocele: Present from infancy (patent processus vaginalis)
B. Symptoms
- The chief complaint is scrotal swelling - often the only symptom in primary hydrocele
- Swelling is usually painless and grows slowly, which is why patients often present late with enormous swelling
- Pain or tenderness suggests secondary hydrocele (underlying disease)
- Swelling may be intermittent in congenital type (reduces when lying down)
- In congenital hydrocele: bilateral swelling should raise suspicion of ascites (tuberculous peritonitis)
C. Past History / Associated History
- History of injury - trauma can cause secondary hydrocele (hematocele)
- History of urinary symptoms, epididymitis or STI - suggests secondary hydrocele
- In a young man, an acute hydrocele should raise suspicion of testicular tumor until proven otherwise
LOCAL EXAMINATION
A. Inspection
-
Skin: Color and temperature are normal in primary hydrocele. In secondary hydrocele the skin may be red if there is underlying infection. The normal rugosity (wrinkles) of scrotal skin is lost because the skin is stretched tense over the fluid.
-
Swelling:
- Can range from small to very large (even hanging to knee level)
- A peculiar constriction is often seen around the base of the swelling
- Tense hydrocele tends to stand out forward (anterior projection)
- Note: size, shape, extent - does it extend up along the spermatic cord to the groin?
-
Impulse on coughing: Must always be checked because ~5% of hydroceles are associated with an inguinal hernia (bubonocele or complete hernia)
B. Palpation
- In a pure scrotal hydrocele, you can palpate the spermatic cord above the swelling (you can "get above" it)
- Exception: infantile hydrocele - you cannot get above it
- Normal temperature, non-tender in primary hydrocele
- Tender in secondary hydrocele
- Cannot be done the classical way (scrotum too mobile)
- Method: Hold the upper pole between thumb and fingers of one hand (to make it tense and steady). Apply intermittent pressure at the lower pole with the other hand. The fluid inside pushes upward, separating the fingers at the upper pole = positive fluctuation
- Best performed in darkness
- Place a pencil torch laterally over the swollen scrotum; view through a roll of paper placed on the other side
- A bright red glow throughout = positive = fluid is clear = hydrocele
- Common student mistake: placing torch posteriorly - the testis blocks the light giving a false negative result
- Uncomplicated hydrocele: transilluminates brightly
- Spermatocele: does NOT transilluminate (fluid is turbid/milky, not clear)
- Raise the scrotum and compress gently
- Congenital hydrocele is reducible (fluid drains back to peritoneal cavity)
- Primary acquired hydrocele is NOT reducible
- Dull on percussion (fluid, not gas)
- Hernia is often resonant (due to intestinal gas inside) - this helps differentiate
- The fluid of the hydrocele completely surrounds and encloses the testis, making it impalpable
- If you can feel the testis separately from the swelling, it is NOT a hydrocele - think cyst of epididymis or spermatocele
GENERAL EXAMINATION
| System | What to look for | Why |
|---|---|---|
| Abdomen | Ascites, abdominal masses, epigastric lymph nodes | Bilateral congenital hydrocele = rule out TB peritonitis; testicular tumor can metastasize to pre-aortic nodes (presents as epigastric lump) |
| Kidneys | Renal mass (bimanual palpation) | Varicocele with recent onset = may be due to renal cell carcinoma |
| Lymph nodes | Inguinal nodes (scrotal skin drainage); pre/para-aortic nodes at transpyloric plane (testis drainage); left supraclavicular nodes | Spread of malignancy |
| Lungs | Auscultation, chest expansion | Rule out pulmonary TB (secondary hydrocele from TB orchitis), lung secondaries from testicular tumor |
| Rectum (PR) | Prostate, seminal vesicles | Secondary hydrocele from epididymitis - rule out prostatitis; TB seminal vesicles |
| General | Edema of lower limbs, face | Cardiac failure, nephrotic syndrome can cause scrotal edema mimicking hydrocele |
INVESTIGATIONS
| Investigation | Purpose |
|---|---|
| Scrotal Ultrasound | Most important - confirms diagnosis, assesses testis (rule out tumor), characterizes fluid |
| Aspiration of fluid | Fluid analysis - amber colored, specific gravity 1.022-1.024, contains water, inorganic salts, cholesterol, fibrinogen, 6% albumin; blood-stained fluid = think tumor; milky fluid = think spermatocele or chylocele |
| Urine examination | Routine - detect infection (E. coli, Strep, Staph); TB bacilli in tuberculous cases |
| Blood - Full count + ESR | Eosinophilia + microfilaria = filariasis; lymphocytosis + high ESR = TB |
| Chest X-ray | Rule out pulmonary TB; rule out lung metastases from testicular tumor |
| IVP (Intravenous Pyelography) | In testicular tumors - locate kidneys for radiotherapy shielding; detect retroperitoneal metastasis displacing ureters |
| Lymphangiography | Detect para-aortic lymph node deposits not yet clinically enlarged |
| Tumor markers | AFP, beta-hCG - elevated in malignant teratoma; hCG >100 IU in 12hr urine = choriocarcinoma |
| Wassermann Reaction (WR) / Kahn test | Positive = syphilitic orchitis causing secondary hydrocele |
Key rule: If tumor is suspected, do NOT aspirate the hydrocele - risk of malignant cell implantation along the needle track.
COMPLICATIONS
-
Hematocele - Bleeding into the hydrocele sac (from spontaneous rupture of blood vessels in the sac wall, post-aspiration, or trauma). The fluid becomes blood-stained and the hydrocele loses its translucency.
-
Infection / Pyocele - Secondarily infected hydrocele, causing acute painful swollen scrotum with fever. Can be confused with suppurated hydrocele or cellulitis.
-
Rupture - Spontaneous or traumatic rupture of the sac, leading to extravasation of fluid into scrotal tissues.
-
Atrophy of the Testis - Long-standing large hydrocele can compress the testicular vessels and lead to gradual testicular atrophy.
-
Hernia into the Hydrocele - In large hydroceles, abdominal contents (intestine) can herniate into the hydrocele sac.
-
Recurrence - After aspiration or sclerotherapy; less common after surgical repair.
-
Calcification - Chronic hydrocele can develop calcium deposits in the wall (calcified hydrocele).
-
Infertility - Raised temperature inside large hydrocele can impair spermatogenesis over time.
DIFFERENTIAL DIAGNOSIS
| Condition | How to distinguish from Hydrocele |
|---|---|
| Inguinal Hernia | Resonant on percussion (gas-containing bowel); impulse on coughing; can't get above the swelling; reduces on lying down; gurgling sound on reduction |
| Epididymal Cyst / Spermatocele | Testis is palpable SEPARATELY from the cyst; cyst lies behind/above testis; epididymal cyst fluid is crystal clear; spermatocele fluid is milky and contains sperms; spermatocele does NOT transilluminate |
| Hematocele | Does NOT transilluminate; history of trauma; dull, heavy; no fluctuation |
| Varicocele | Feels like a "bag of worms"; thrill-like impulse on coughing; reduces on lying down; left side more common; associated with left renal vein pathology |
| Testicular Tumor | Hard, heavy testis; testicular sensation lost; irregular surface; does NOT transilluminate unless secondary hydrocele co-exists; ultrasound confirms |
| Lymph Varix (Filariasis) | Soft, doughy feel; thrill on coughing; less readily reducible than varicocele; eosinophilia; history of filariasis in endemic area |
| Epididymo-orchitis | Tender, hot, red scrotum; fever; urethral discharge; urinary symptoms; WBC elevated |
| Torsion of Testis | Sudden severe pain; tender; high-riding testis; loss of cremasteric reflex; Doppler shows absent blood flow |
TREATMENT (Summary)
- Congenital hydrocele in infants: Wait until 18 months - most resolve spontaneously. If persistent, herniotomy (ligation of patent processus vaginalis).
- Small primary hydrocele: Conservative - no treatment needed if asymptomatic.
- Large symptomatic primary hydrocele: Surgery is the mainstay.
- Lord's operation (Plication): Suitable for thin-walled sac; minimal dissection; interrupted absorbable sutures plicate the tunica.
- Jaboulay's procedure (Eversion): Hydrocele sac is everted and anchored behind the testis with sutures; risk of scrotal hematoma from cut edges.
- Excision of sac: For thick-walled secondary hydrocele.
- Aspiration ± Sclerotherapy (tetracycline): For unfit/elderly patients; fluid always re-accumulates; risk of hematocele from aspiration.
- Secondary hydrocele: Treat the underlying cause first.
It should to easy to revise and don't include extra matter ...give only from the inform i provided
HYDROCELE - Revision Notes
DEFINITION
TYPES
| Type | Key Feature |
|---|---|
| Congenital | Processus vaginalis stays patent; communicates with peritoneum |
| Primary (Idiopathic) | Most common; middle-aged men; no known cause |
| Secondary | Due to disease of testis/epididymis; men 20-40 yrs |
HISTORY
- Primary hydrocele → most common >40 years
- Secondary hydrocele → common 20-40 years
- Congenital hydrocele → seen even in infants
- Main complaint = scrotal swelling only (that is why patient presents late with enormous swelling)
- Usually painless (primary)
- Secondary hydrocele may be tender
- Congenital hydrocele → disappears on lying down, returns on standing
LOCAL EXAMINATION
INSPECTION
- Skin is tense → normal rugosity (wrinkles) lost
- Subcutaneous veins prominent
- Size can be small to very large (hanging to knee level)
- A peculiar constriction often seen around the base of swelling
- Tense hydrocele tends to stand out forward
- Check for impulse on coughing (5% cases associated with inguinal hernia)
PALPATION
- In pure hydrocele → can get above the swelling ✓
- Exception → infantile hydrocele (cannot get above it)
- Normal method not possible (scrotum too mobile)
- Method: Hold upper pole tense with one hand → apply intermittent pressure at lower pole → fingers at upper pole pushed apart = positive
- Best done in darkness
- Pencil torch placed laterally; roll of paper on the other side
- Red glow throughout = positive
- Common mistake: torch placed posteriorly → testis blocks light → false negative
- Primary hydrocele → transilluminates ✓
- Spermatocele → does NOT transilluminate (fluid is not clear)
- Raise scrotum + compress gently
- Congenital hydrocele is reducible
- In bilateral congenital hydrocele → always examine abdomen for ascites (associated with TB peritonitis)
- Dull on percussion (vs. hernia which is resonant)
- Fluid surrounds body of testis → testis is impalpable
- If testis is palpable separately → swelling is NOT a hydrocele (think cyst of epididymis / spermatocele)
- Must not omit this step
- Expansile impulse → hernia or congenital hydrocele
GENERAL EXAMINATION
| System | What to look for | Reason |
|---|---|---|
| Lungs | Examination | Rule out TB (in secondary hydrocele from TB orchitis) |
| Kidneys | Palpation | Varicocele of recent onset → may be from renal adenocarcinoma |
| Rectum (PR) | Prostate + seminal vesicles | Prostatitis precedes epididymo-orchitis; TB seminal vesicles enlarged and tender |
| Abdomen | Ascites | Bilateral congenital hydrocele → rule out TB peritonitis |
INVESTIGATIONS
| Test | Finding / Purpose |
|---|---|
| Aspiration of fluid | Amber color; SG 1.022-1.024; contains water, inorganic salts, cholesterol, fibrinogen, 6% albumin |
| Blood-stained fluid → secondary hydrocele from testicular tumor | |
| Ultrasonography | Know position of testis; detect hematocele, secondary hydrocele, torsion |
| Urine examination | Routine in all cases of epididymo-orchitis |
| Blood | Eosinophilia + microfilaria → filariasis; Lymphocytosis + high ESR → TB |
| Chest X-ray | Rule out pulmonary TB; secondary deposits in lungs (teratoma) |
| IVP | Testicular tumors - locate kidneys, detect retroperitoneal metastasis |
| Lymphangiography | Para-aortic lymph node deposits (not yet clinically enlarged) |
| WR / Kahn test | Positive → syphilitic orchitis |
| Aschheim-Zondek | Positive → Sertoli cell tumor |
| hCG (12hr urine) | >100 IU → choriocarcinoma of testis |
Remember: Fluid should be aspirated in secondary hydrocele to allow better palpation of testis and epididymis.
DIFFERENTIAL DIAGNOSIS
| Condition | Key Distinguishing Point |
|---|---|
| Inguinal Hernia | Resonant on percussion; impulse on coughing; cannot get above swelling |
| Cyst of Epididymis | Testis palpable separately; fluid is crystal clear; transilluminates |
| Spermatocele | Testis palpable separately; fluid is milky; does NOT transilluminate |
| Hematocele | Does NOT transilluminate; history of trauma; no fluctuation |
| Varicocele | "Bag of worms" feel; thrill-like impulse on coughing; more readily reducible than lymph varix |
| Lymph Varix (Filariasis) | Soft, doughy feel; thrill on coughing; less readily reducible than varicocele |
| Testicular Tumor | Hard, heavy; testicular sensation lost; secondary hydrocele fluid is blood-stained |
QUICK MEMORY AID
HYDROCELE = Fluid in tunica vaginalis
2 CARDINAL SIGNS:
1. FLUCTUATION (upper pole held, lower pole pressed)
2. TRANSLUCENCY (torch lateral → red glow)
Testis IMPALPABLE (fluid surrounds it)
CAN get above the swelling (except infantile)
DULL on percussion
PRIMARY → >40 yrs, painless, NOT reducible
CONGENITAL → reducible, intermittent, check for ascites
Aspiration fluid → amber, SG 1.022-1.024
Blood-stained fluid → TUMOR (do NOT aspirate if tumor suspected!)
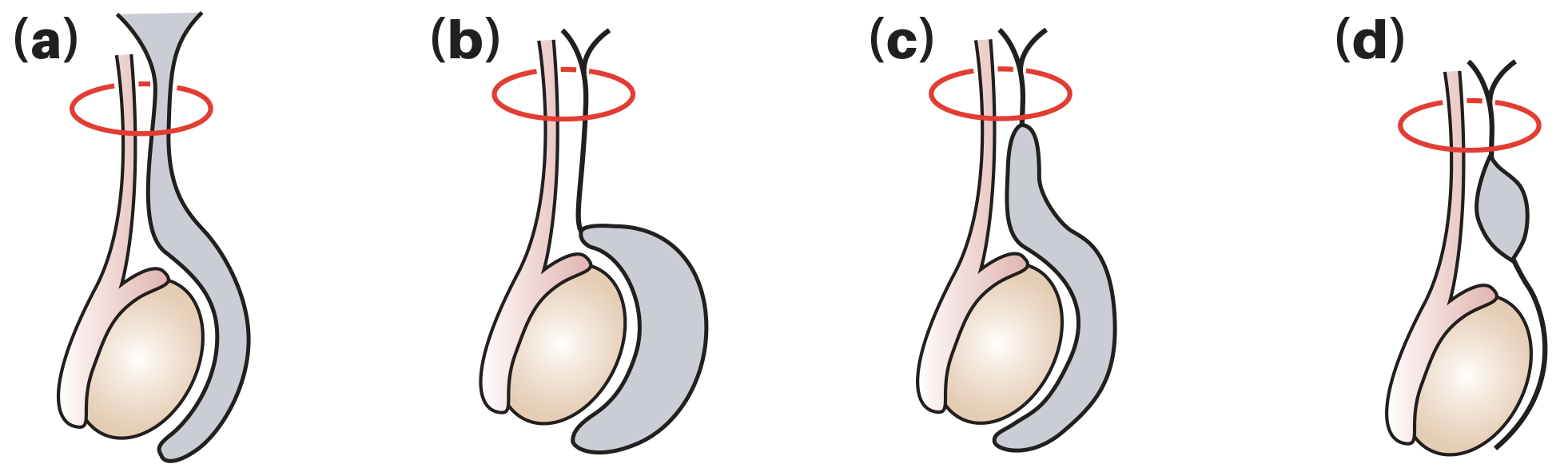
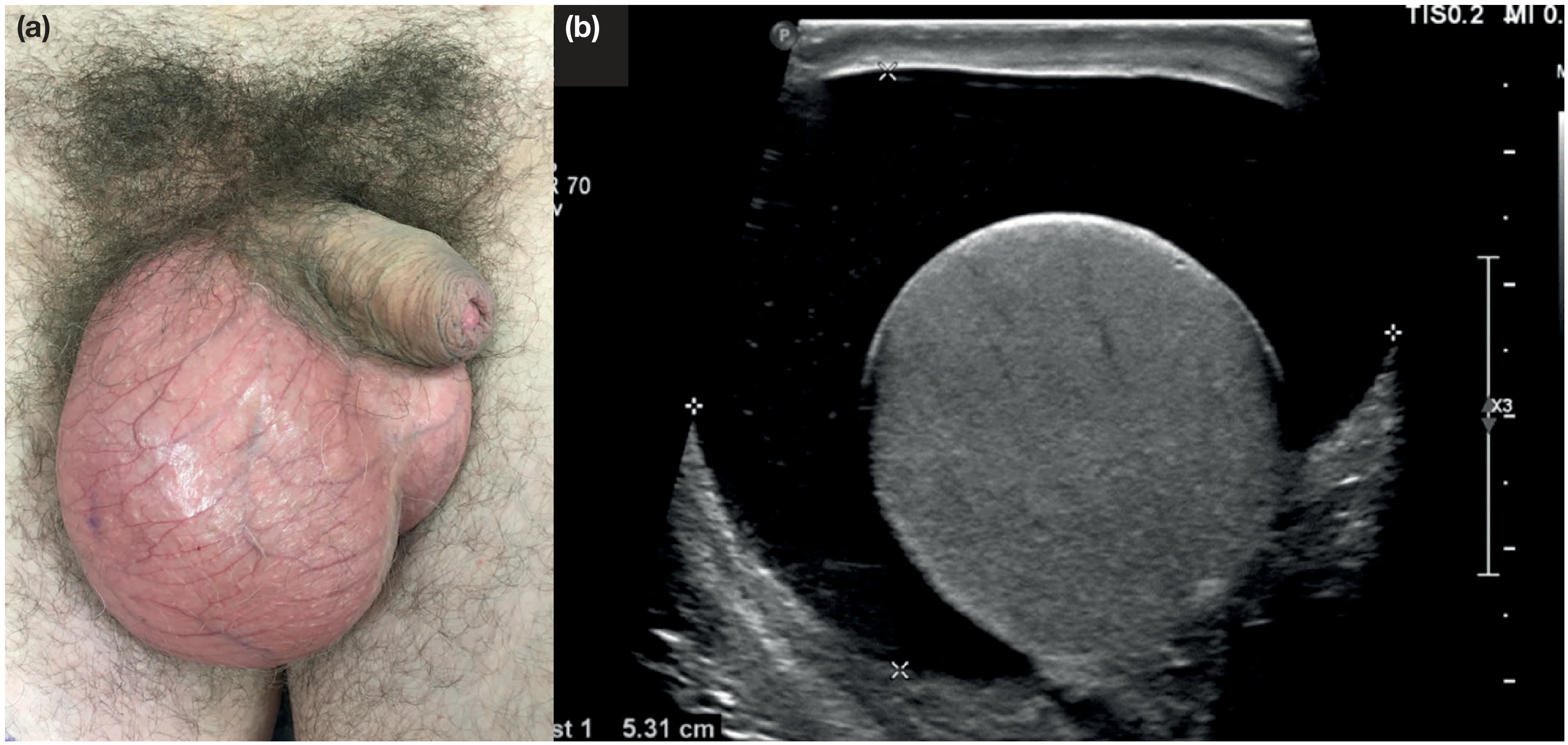
Here is a detailed yet simplified clinical guide to **Hydrocele** covering every aspect you requested: --- # HYDROCELE - Complete Clinical Guide --- ## DEFINITION A **hydrocele** is an abnormal collection of serous (clear) fluid in a part of the processus vaginalis - usually in the **tunica vaginalis** surrounding the testis. Think of it as a water-filled balloon wrapped around the testis inside the scrotum. **Incidence:** Affects ~1% of adult men. Over 80% of newborn boys have a patent (open) processus vaginalis, but most close on their own within 18 months of age. --- ## TYPES / CLASSIFICATION  *Figure: (a) Vaginal/primary hydrocele - most common; (b) Infantile hydrocele; (c) Congenital/communicating hydrocele; (d) Hydrocele of the cord* | Type | What happens | Key feature | |------|-------------|-------------| | **Congenital (Communicating)** | Processus vaginalis stays open; peritoneal fluid flows freely into scrotum | Disappears when lying down, reappears on standing | | **Primary (Idiopathic)** | Processus is closed; fluid accumulates from imbalance of production vs. absorption | Most common; middle-aged men; painless | | **Secondary** | Caused by underlying disease (infection, tumor, trauma, torsion) | Tender; men >40 yrs; always investigate cause | | **Infantile** | Mid-portion of processus open; communicates with tunica but not peritoneum | Presents in infancy/childhood | | **Hydrocele of the Cord** | Isolated cyst along the spermatic cord | Oval swelling above the testis | --- ## HISTORY ### A. Age - **Primary hydrocele:** Most common in men **>40 years** - **Secondary hydrocele:** More common between **20-40 years** (due to underlying conditions like epididymo-orchitis or tumor) - **Congenital hydrocele:** Present from **infancy** (patent processus vaginalis) ### B. Symptoms - The **chief complaint is scrotal swelling** - often the only symptom in primary hydrocele - Swelling is usually **painless** and grows slowly, which is why patients often present late with enormous swelling - **Pain or tenderness** suggests secondary hydrocele (underlying disease) - Swelling may be **intermittent** in congenital type (reduces when lying down) - In congenital hydrocele: bilateral swelling should raise suspicion of **ascites (tuberculous peritonitis)** ### C. Past History / Associated History - History of **injury** - trauma can cause secondary hydrocele (hematocele) - History of **urinary symptoms, epididymitis or STI** - suggests secondary hydrocele - In a **young man**, an acute hydrocele should raise suspicion of **testicular tumor** until proven otherwise --- ## LOCAL EXAMINATION ### A. Inspection 1. **Skin:** Color and temperature are **normal** in primary hydrocele. In secondary hydrocele the skin may be red if there is underlying infection. The normal rugosity (wrinkles) of scrotal skin is lost because the skin is stretched tense over the fluid. 2. **Swelling:** - Can range from small to **very large** (even hanging to knee level) - A peculiar constriction is often seen around the base of the swelling - Tense hydrocele tends to **stand out forward** (anterior projection) - Note: size, shape, extent - does it extend up along the spermatic cord to the groin? 3. **Impulse on coughing:** Must always be checked because ~5% of hydroceles are associated with an **inguinal hernia** (bubonocele or complete hernia) ### B. Palpation The two **cardinal signs** of hydrocele are **fluctuation** and **translucency**. **1. Getting above the swelling:** - In a pure scrotal hydrocele, you can palpate the spermatic cord above the swelling (you can "get above" it) - Exception: infantile hydrocele - you cannot get above it **2. Temperature and Tenderness:** - Normal temperature, non-tender in primary hydrocele - Tender in secondary hydrocele **3. Fluctuation Test:** - Cannot be done the classical way (scrotum too mobile) - Method: Hold the **upper pole** between thumb and fingers of one hand (to make it tense and steady). Apply intermittent pressure at the **lower pole** with the other hand. The fluid inside pushes upward, separating the fingers at the upper pole = **positive fluctuation** **4. Translucency Test (most important):** - Best performed in **darkness** - Place a **pencil torch laterally** over the swollen scrotum; view through a roll of paper placed on the other side - A **bright red glow** throughout = positive = fluid is clear = hydrocele - Common student mistake: placing torch posteriorly - the testis blocks the light giving a false negative result - Uncomplicated hydrocele: **transilluminates brightly** - Spermatocele: does NOT transilluminate (fluid is turbid/milky, not clear) **5. Reducibility:** - Raise the scrotum and compress gently - **Congenital hydrocele** is reducible (fluid drains back to peritoneal cavity) - Primary acquired hydrocele is NOT reducible **6. Percussion:** - **Dull** on percussion (fluid, not gas) - Hernia is often **resonant** (due to intestinal gas inside) - this helps differentiate **7. Palpation of Testis:** - The fluid of the hydrocele completely **surrounds and encloses** the testis, making it **impalpable** - If you can feel the testis separately from the swelling, it is NOT a hydrocele - think cyst of epididymis or spermatocele **8. Surface:** Smooth, well-defined, egg-shaped swelling **9. Consistency:** Soft and cystic (unless wall is very thick in chronic/secondary hydrocele) **Clinical photo and ultrasound of a large primary right-sided hydrocele:**  --- ## GENERAL EXAMINATION | System | What to look for | Why | |--------|-----------------|-----| | **Abdomen** | Ascites, abdominal masses, epigastric lymph nodes | Bilateral congenital hydrocele = rule out TB peritonitis; testicular tumor can metastasize to pre-aortic nodes (presents as epigastric lump) | | **Kidneys** | Renal mass (bimanual palpation) | Varicocele with recent onset = may be due to renal cell carcinoma | | **Lymph nodes** | Inguinal nodes (scrotal skin drainage); pre/para-aortic nodes at transpyloric plane (testis drainage); left supraclavicular nodes | Spread of malignancy | | **Lungs** | Auscultation, chest expansion | Rule out pulmonary TB (secondary hydrocele from TB orchitis), lung secondaries from testicular tumor | | **Rectum (PR)** | Prostate, seminal vesicles | Secondary hydrocele from epididymitis - rule out prostatitis; TB seminal vesicles | | **General** | Edema of lower limbs, face | Cardiac failure, nephrotic syndrome can cause scrotal edema mimicking hydrocele | --- ## INVESTIGATIONS | Investigation | Purpose | |--------------|---------| | **Scrotal Ultrasound** | Most important - confirms diagnosis, assesses testis (rule out tumor), characterizes fluid | | **Aspiration of fluid** | Fluid analysis - amber colored, specific gravity 1.022-1.024, contains water, inorganic salts, cholesterol, fibrinogen, 6% albumin; blood-stained fluid = think tumor; milky fluid = think spermatocele or chylocele | | **Urine examination** | Routine - detect infection (E. coli, Strep, Staph); TB bacilli in tuberculous cases | | **Blood - Full count + ESR** | Eosinophilia + microfilaria = filariasis; lymphocytosis + high ESR = TB | | **Chest X-ray** | Rule out pulmonary TB; rule out lung metastases from testicular tumor | | **IVP (Intravenous Pyelography)** | In testicular tumors - locate kidneys for radiotherapy shielding; detect retroperitoneal metastasis displacing ureters | | **Lymphangiography** | Detect para-aortic lymph node deposits not yet clinically enlarged | | **Tumor markers** | AFP, beta-hCG - elevated in malignant teratoma; hCG >100 IU in 12hr urine = choriocarcinoma | | **Wassermann Reaction (WR) / Kahn test** | Positive = syphilitic orchitis causing secondary hydrocele | > **Key rule:** If tumor is suspected, **do NOT aspirate** the hydrocele - risk of malignant cell implantation along the needle track. --- ## COMPLICATIONS 1. **Hematocele** - Bleeding into the hydrocele sac (from spontaneous rupture of blood vessels in the sac wall, post-aspiration, or trauma). The fluid becomes blood-stained and the hydrocele loses its translucency. 2. **Infection / Pyocele** - Secondarily infected hydrocele, causing acute painful swollen scrotum with fever. Can be confused with suppurated hydrocele or cellulitis. 3. **Rupture** - Spontaneous or traumatic rupture of the sac, leading to extravasation of fluid into scrotal tissues. 4. **Atrophy of the Testis** - Long-standing large hydrocele can compress the testicular vessels and lead to gradual testicular atrophy. 5. **Hernia into the Hydrocele** - In large hydroceles, abdominal contents (intestine) can herniate into the hydrocele sac. 6. **Recurrence** - After aspiration or sclerotherapy; less common after surgical repair. 7. **Calcification** - Chronic hydrocele can develop calcium deposits in the wall (calcified hydrocele). 8. **Infertility** - Raised temperature inside large hydrocele can impair spermatogenesis over time. --- ## DIFFERENTIAL DIAGNOSIS | Condition | How to distinguish from Hydrocele | |-----------|----------------------------------| | **Inguinal Hernia** | Resonant on percussion (gas-containing bowel); impulse on coughing; can't get above the swelling; reduces on lying down; gurgling sound on reduction | | **Epididymal Cyst / Spermatocele** | Testis is palpable SEPARATELY from the cyst; cyst lies behind/above testis; epididymal cyst fluid is crystal clear; spermatocele fluid is milky and contains sperms; spermatocele does NOT transilluminate | | **Hematocele** | Does NOT transilluminate; history of trauma; dull, heavy; no fluctuation | | **Varicocele** | Feels like a "bag of worms"; thrill-like impulse on coughing; reduces on lying down; left side more common; associated with left renal vein pathology | | **Testicular Tumor** | Hard, heavy testis; testicular sensation lost; irregular surface; does NOT transilluminate unless secondary hydrocele co-exists; ultrasound confirms | | **Lymph Varix (Filariasis)** | Soft, doughy feel; thrill on coughing; less readily reducible than varicocele; eosinophilia; history of filariasis in endemic area | | **Epididymo-orchitis** | Tender, hot, red scrotum; fever; urethral discharge; urinary symptoms; WBC elevated | | **Torsion of Testis** | Sudden severe pain; tender; high-riding testis; loss of cremasteric reflex; Doppler shows absent blood flow | --- ## TREATMENT (Summary) - **Congenital hydrocele in infants:** Wait until 18 months - most resolve spontaneously. If persistent, **herniotomy** (ligation of patent processus vaginalis). - **Small primary hydrocele:** Conservative - no treatment needed if asymptomatic. - **Large symptomatic primary hydrocele:** Surgery is the mainstay. - **Lord's operation (Plication):** Suitable for thin-walled sac; minimal dissection; interrupted absorbable sutures plicate the tunica. - **Jaboulay's procedure (Eversion):** Hydrocele sac is everted and anchored behind the testis with sutures; risk of scrotal hematoma from cut edges. - **Excision of sac:** For thick-walled secondary hydrocele. - **Aspiration ± Sclerotherapy (tetracycline):** For unfit/elderly patients; fluid always re-accumulates; risk of hematocele from aspiration. - **Secondary hydrocele:** Treat the underlying cause first. --- *Sources: Bailey and Love's Short Practice of Surgery (28th Edition), p. 1586-1588; user-provided clinical text on Scrotum examination* I want this in pointwise
HYDROCELE
DEFINITION
- Abnormal collection of serous fluid in the tunica vaginalis around the testis
- Acquired varieties → Primary (idiopathic) or Secondary (from diseases of testis/epididymis)
TYPES
- Congenital → processus vaginalis remains patent; communicates with peritoneal cavity
- Primary → idiopathic; middle-aged men; most common
- Secondary → due to underlying testis/epididymis disease
HISTORY
- Primary hydrocele → most common >40 years
- Secondary hydrocele → common 20–40 years
- Congenital hydrocele → seen even in infants
- Main complaint = scrotal swelling only
- Patient often presents late with enormous swelling (painless → ignored)
- Primary → not tender
- Secondary → may be tender
- Congenital → disappears on lying down, returns on standing
- Bilateral congenital → suspect ascites from TB peritonitis
LOCAL EXAMINATION
A. INSPECTION
- Skin is tense → normal rugosity (wrinkles) lost
- Subcutaneous veins become prominent
- Size: small → very large (may hang up to knee level)
- A peculiar constriction often seen around the swelling
- Tense hydrocele → tends to stand out forward
- Check impulse on coughing → ~5% cases have associated inguinal hernia
B. PALPATION
- Pure hydrocele → can get above the swelling ✓
- Exception → infantile hydrocele (cannot get above it)
- Classical method not possible (scrotum too mobile)
- Hold upper pole tense with one hand → press lower pole intermittently with other hand → fingers at upper pole pushed apart = positive
- Best done in darkness
- Pencil torch placed laterally → roll of paper on the other side
- Red glow = positive
- Common mistake → torch placed posteriorly → testis blocks light → false negative
- Primary hydrocele → transilluminates ✓
- Spermatocele → does NOT transilluminate (fluid not clear)
- Raise scrotum + compress gently
- Congenital hydrocele → reducible
- Primary hydrocele → NOT reducible
- Bilateral + reducible → examine abdomen for ascites (TB peritonitis)
- Dull (fluid)
- Hernia → resonant (intestinal gas)
- Fluid surrounds testis → testis is impalpable
- If testis palpable separately → NOT hydrocele → think cyst of epididymis / spermatocele
- Expansile impulse → hernia or congenital hydrocele
- Must not be omitted
GENERAL EXAMINATION
- Lungs → rule out pulmonary TB (in TB epididymo-orchitis causing secondary hydrocele)
- Kidneys → examine in varicocele of recent onset → may be renal adenocarcinoma
- Rectum (PR) → prostate (acute prostatitis precedes epididymo-orchitis); seminal vesicles enlarged + tender in TB
- Abdomen → ascites in bilateral congenital hydrocele → rule out TB peritonitis
INVESTIGATIONS
- Aspiration of fluid → amber color; SG 1.022–1.024; contains water, inorganic salts, cholesterol, fibrinogen, 6% albumin
- Blood-stained fluid → secondary hydrocele from testicular tumor → aspirate to allow better palpation
- Ultrasonography → position of testis; hematocele; secondary hydrocele; torsion
- Urine → routine in epididymo-orchitis; detect E. coli, Strep, Staph; TB bacilli in TB cases
- Blood → eosinophilia + microfilaria → filariasis; lymphocytosis + high ESR → TB
- Chest X-ray → rule out pulmonary TB; lung deposits from teratoma
- IVP → testicular tumors → locate kidneys; detect retroperitoneal metastasis displacing ureters
- Lymphangiography → detect para-aortic deposits not yet clinically enlarged; assess response to radiotherapy
- WR / Kahn test → positive → syphilitic orchitis
- Aschheim-Zondek test → positive → Sertoli cell tumor
- hCG (12hr urine) → >100 IU → choriocarcinoma of testis
⚠️ If tumor suspected → DO NOT aspirate (risk of malignant needle-track implantation)
DIFFERENTIAL DIAGNOSIS
- Inguinal Hernia → resonant on percussion; impulse on coughing; cannot get above swelling
- Cyst of Epididymis → testis palpable separately; fluid clear; transilluminates
- Spermatocele → testis palpable separately; fluid milky; does NOT transilluminate
- Hematocele → does NOT transilluminate; history of trauma
- Varicocele → "bag of worms"; thrill-like impulse on coughing; readily reducible
- Lymph Varix → soft, doughy; thrill on coughing; less readily reducible than varicocele
- Testicular Tumor → heavy, hard; testicular sensation lost; fluid blood-stained
QUICK RECALL BOX
CARDINAL SIGNS → Fluctuation + Translucency
Testis → IMPALPABLE (fluid surrounds it)
CAN get above swelling (except infantile)
DULL on percussion
Congenital → REDUCIBLE + intermittent
Primary → >40 yrs, painless, NOT reducible
Aspiration fluid → amber, SG 1.022–1.024
Blood-stained → TUMOR (do NOT aspirate if tumor suspected!)
Torch → LATERALLY (not posteriorly → false negative)