Ecg condition with explaination
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching Images
STEMI NSTEMI ST elevation depression ECG changes myocardial infarction
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I have everything needed for a comprehensive, well-illustrated answer. Here it is:
ECG Changes in Acute Coronary Syndromes: STEMI & NSTEMI
Overview: Acute Coronary Syndromes (ACS)
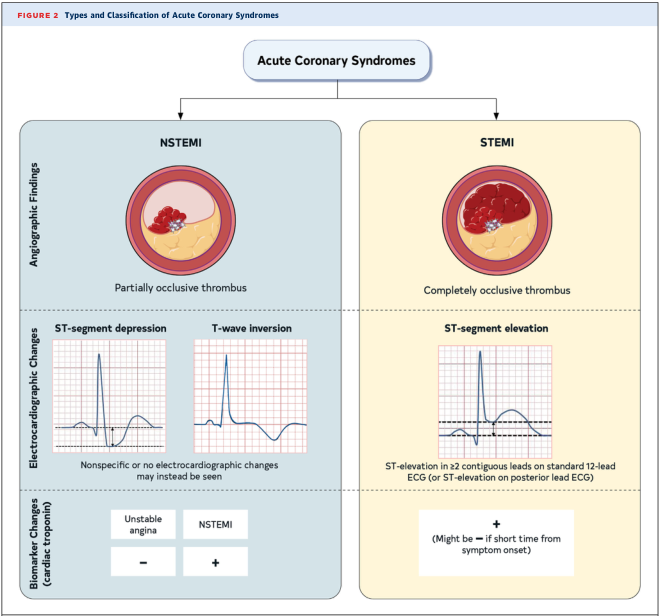
ACS is classified based on two factors: coronary artery occlusion and ECG changes.
| Feature | STEMI | NSTEMI / Unstable Angina |
|---|---|---|
| Thrombus | Complete occlusion | Partial occlusion |
| ECG | ST elevation | ST depression / T-wave inversion / normal |
| Troponin | Positive (may be negative very early) | Positive (NSTEMI) / Negative (UA) |
The Physiology Behind ST Changes
Why does the ST segment move?
Severe acute ischemia lowers the resting membrane potential of affected myocytes and shortens their action potential duration. This creates a voltage gradient between normal and ischemic zones, generating currents of injury that shift the ST segment on the surface ECG.
- Transmural ischemia (full wall thickness) → ST vector points outward → ST elevation in overlying leads
- Subendocardial ischemia (inner layer only) → ST vector points inward toward cavity → ST depression in overlying leads (+ ST elevation in aVR)
(Harrison's Principles of Internal Medicine, 22e)
STEMI — ST-Elevation Myocardial Infarction
Definition
ST elevation in ≥2 contiguous leads caused by complete coronary occlusion → transmural ischemia and necrosis.
ECG Sequence (Evolution Over Time)
| Stage | Time | ECG Finding |
|---|---|---|
| Hyperacute | Minutes | Tall, peaked "hyperacute" T waves |
| Acute | Hours | ST elevation (convex/tombstone morphology) |
| Evolving | Hours–days | ST elevation + pathological Q waves develop |
| Subacute | Days–weeks | ST normalises; T-wave inversions appear |
| Chronic/Old | Weeks–months | Persistent Q waves; T waves may normalise |
Key ECG Features
- ST elevation: ≥1 mm in limb leads, ≥2 mm in precordial leads
- Morphology: Convex ("tombstone") upward curve — not concave
- Reciprocal ST depression: in leads 180° opposite the infarct territory
- Q waves: pathological if >40 ms wide or >25% of R-wave height
- aVR elevation: global subendocardial ischemia / left main disease
🫀 Anterior STEMI (LAD occlusion)
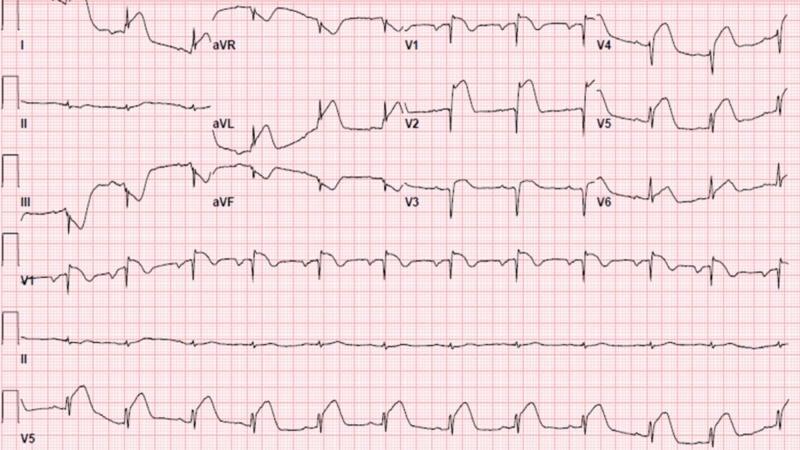
Massive ST elevation in V1–V3 ("tombstoning"), with reciprocal ST depression in inferior leads (II, III, aVF). Classic proximal LAD occlusion.
🫀 Anterolateral STEMI (proximal LAD)

ST elevation in V1–V6, I, aVL + hyperacute T waves V2–V4 + reciprocal depression in II, III, aVF.
🫀 Inferior STEMI (RCA or LCx occlusion)
ST elevation in II, III, aVF + reciprocal depression in I, aVL + posterior changes (tall R and ST depression in V1–V3).
Lead Localisation of STEMI
| Territory | Leads with ST Elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD (proximal) |
| Anterolateral | V1–V6, I, aVL | LAD (proximal) |
| Lateral | I, aVL, V5–V6 | LCx or diagonal |
| Inferior | II, III, aVF | RCA (usually) or LCx |
| Posterior | Tall R + ST depression V1–V3 | RCA or LCx |
| Right ventricle | V1, V3R–V4R | Proximal RCA |
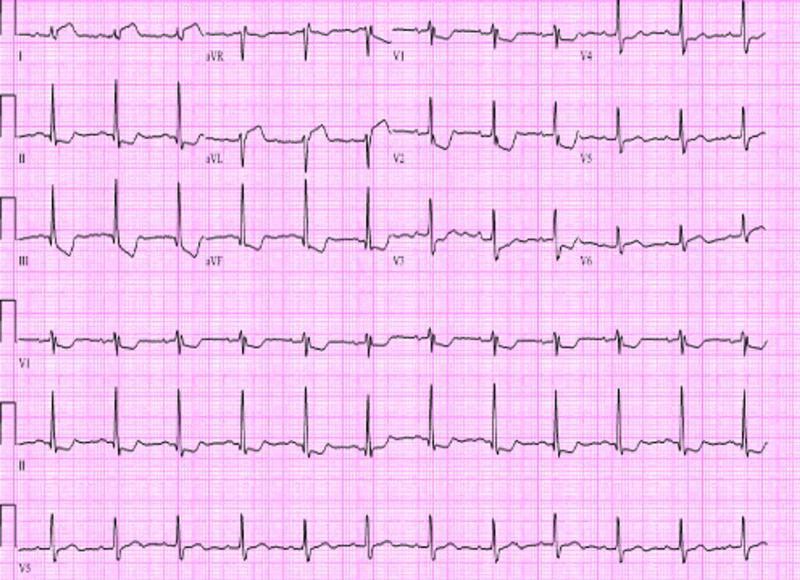
NSTEMI — Non-ST-Elevation MI
Definition
Partial coronary occlusion → subendocardial ischemia. Troponin is elevated (differentiating from unstable angina, where troponin is negative).
ECG Features
- ST depression: ≥0.5 mm, horizontal or downsloping (more specific than upsloping)
- T-wave inversion: often deep, symmetric, most prominent in the territory of the affected artery
- Wellens' Sign: deep symmetric T-wave inversions in V2–V4 → critical LAD stenosis (high-risk NSTEMI equivalent)
- ECG may be normal in 30–40% of NSTEMI cases — diagnosis depends on troponin
Differentiating ST Depression Morphologies
| Morphology | Significance |
|---|---|
| Horizontal/downsloping | High specificity for ischemia |
| Upsloping | Lower specificity; can be normal variant |
| Downsloping with T inversion | Strongly suggests significant ischemia |
Differential Diagnosis of ST Elevation (not all STEMI!)
| Cause | Clue |
|---|---|
| Acute pericarditis | Diffuse saddle-shaped elevation + PR depression; involves all leads |
| Early repolarization | Young patients, concave ST elevation, J-point notch |
| LBBB | Wide QRS, discordant ST-T changes |
| Brugada syndrome | Coved ST elevation in V1–V2, RBBB-like |
| Takotsubo syndrome | Post-stress, anterior ST changes, apical ballooning |
| Hyperkalemia | Peaked T waves, wide QRS |
| LV aneurysm | Persistent ST elevation weeks after MI |
(Goldman-Cecil Medicine; Harrison's 22e)
Management Principle
The ECG distinction is immediately actionable:
- STEMI → Emergency reperfusion within 90 minutes (primary PCI) or 30 minutes (thrombolysis if PCI unavailable)
- NSTEMI → Anticoagulation, antiplatelets, risk-stratified PCI (usually within 24–72 hours)
ECG should be obtained within 10 minutes of arrival for any patient with chest pain. If initial ECG is non-diagnostic, repeat in 5–10 minutes. — Textbook of Family Medicine, 9e
Sources: Harrison's Principles of Internal Medicine 22e | Goldman-Cecil Medicine | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.