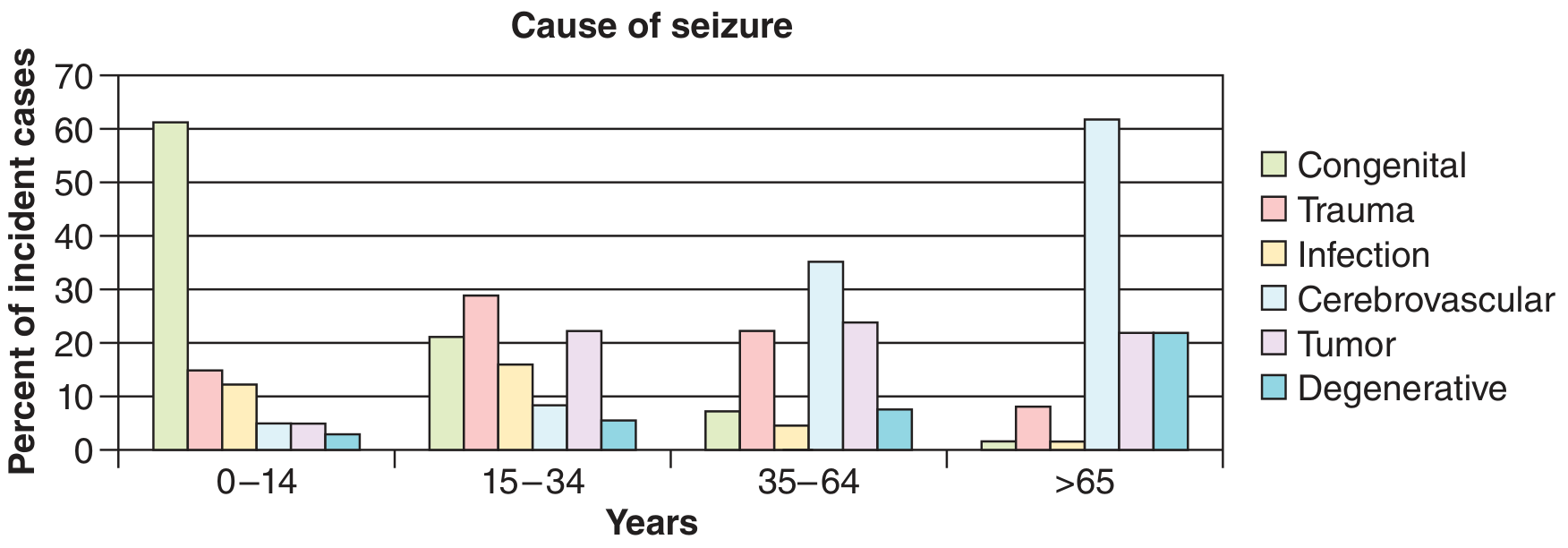
Causes of acute paraparesis
Causes of Acute Paraparesis
Localizing the Level First
| Feature | Suggests |
|---|---|
| Flaccid legs, areflexia, sensory level | Spinal cord (acute "spinal shock" phase) |
| Flaccid legs, areflexia, no sensory level | Cauda equina or peripheral nerve/muscle |
| Spastic legs, sensory level | Spinal cord (UMN) |
| Sphincter involvement | Spinal cord or cauda equina |
| Dissociated sensory loss (pain/temp ↓, proprioception preserved) | Anterior cord syndrome |
I. Spinal Cord Causes (Most Common)
A. Compressive / Extrinsic
| Cause | Key Features |
|---|---|
| Spinal epidural abscess | Fever, back pain, progressive neurological deficit; percussion tenderness; MRI confirms; emergency decompression + IV antibiotics |
| Spinal epidural hematoma | Sudden severe radicular pain → weakness; associated with anticoagulation, trauma, coagulopathy, lumbar puncture; treat with surgical decompression |
| Acute disc herniation (midline, thoracic/cervical) | Acute cord compression; trauma or spontaneous |
| Metastatic spinal cord compression | Night pain worse lying flat; known or occult malignancy (breast, lung, prostate, myeloma); MRI urgent |
| Atlanto-axial subluxation | Rheumatoid arthritis, Down syndrome, trauma |
| Acute spondylotic myelopathy | Hyperextension injury on background of cervical spondylosis; pre-existing canal stenosis; ligamentum flavum buckling |
| Subdural hematoma / empyema | Rare; similar presentation to epidural |
B. Intrinsic / Noncompressive — Vascular
| Cause | Key Features |
|---|---|
| Spinal cord infarction (anterior spinal artery syndrome) | Hyperacute onset; paraplegia/paraparesis + spinothalamic loss (pain & temp ↓) with preserved dorsal columns (proprioception intact); causes include aortic atherosclerosis, aortic dissection, aortic surgery, vertebral artery dissection/occlusion, cardiogenic emboli, vasculitis, profound hypotension; MRI brain negative for bilateral ACA infarcts |
| Spinal AVM / arteriovenous fistula | Dural AVF most common in older men; stepwise or acute myelopathy |
| Hematomyelia (intramedullary hemorrhage) | Acute painful transverse myelopathy; causes: trauma, vascular malformation, vasculitis (polyarteritis nodosa, SLE), bleeding disorders, cord neoplasm |
| Spinal subarachnoid hemorrhage | Focal deficits at bleed level, headache possible; MRI ± LP |
C. Intrinsic / Noncompressive — Inflammatory / Demyelinating
| Cause | Key Features |
|---|---|
| Acute transverse myelitis (idiopathic) | Paraplegia + sensory level + sphincter dysfunction; follows viral illness in ~30%; thoracic cord in 60–70%; MRI T2 signal change ± enhancement |
| Multiple sclerosis | Partial or complete cord syndrome; relapsing history; MRI shows other lesions; CSF oligoclonal bands |
| Neuromyelitis optica spectrum disorder (NMOSD) | Anti-AQP4 or anti-MOG antibodies; longitudinally extensive lesion (≥3 segments); often severe |
| Sarcoidosis | Multisystem involvement; serum ACE, chest CT, biopsy |
| Systemic lupus erythematosus (SLE) | Myelopathy in known or new SLE; antiphospholipid syndrome overlap |
| Behçet's disease | Orogenital ulcers, uveitis; brainstem/cord involvement |
| Acute disseminated encephalomyelitis (ADEM) | Post-infectious/post-vaccination; multifocal CNS; commoner in children |
D. Intrinsic / Noncompressive — Infectious
| Cause | Key Features |
|---|---|
| Viral myelitis — HSV-2, VZV, EBV, CMV, enterovirus, HIV, HHV-6 | CSF PCR; HIV myelopathy in advanced disease |
| HTLV-1 myelopathy (tropical spastic paraparesis) | Subacute > acute; endemic regions; serology |
| West Nile virus | Acute flaccid paralysis (anterior horn cells); fever, encephalitis possible |
| Poliomyelitis | Acute flaccid paraparesis; anterior horn cell |
| Schistosomiasis | Endemic areas; lumbosacral cord; granulomatous myelitis |
| Neurosyphilis | Meningovascular; CSF VDRL |
| Lyme disease | Borrelia; radiculomyelopathy |
| Tuberculous myelitis / Pott's disease | Vertebral destruction, epidural spread; endemic setting |
II. Cauda Equina / Conus Medullaris
- Massive midline lumbar disc prolapse — most common; acute back pain + bilateral leg weakness + urinary retention
- Cauda equina tumor (ependymoma, schwannoma, meningioma)
- Lumbosacral trauma
- HIV-related acute lumbosacral polyradiculopathy (CMV in immunocompromised)
- Spinal epidural abscess/hematoma at lumbar level
III. Cerebral / Supratentorial Causes (Rare)
| Cause | Key Features |
|---|---|
| Bilateral ACA territory infarction | Shoulder shrug (shoulder abduction) also affected |
| Superior sagittal sinus / cortical venous thrombosis | Headache, seizures, bilateral leg weakness from parasagittal involvement |
| Acute hydrocephalus | Bilateral leg weakness (stretching of periventricular fibers) |
| Parasagittal meningioma | More subacute; bilateral leg signs |
IV. Peripheral / Neuromuscular Causes
| Cause | Features |
|---|---|
| Guillain-Barré syndrome | Ascending flaccid areflexic weakness; albuminocytologic dissociation in CSF |
| Acute anterior horn cell disease — Polio, West Nile | Fever + asymmetric flaccid paralysis |
| Myopathy / periodic paralysis | Metabolic (K⁺, Ca²⁺, phosphate, Mg²⁺ disturbances); no sensory loss; no reflexes lost early |
| Toxic myopathy / botulism | Descending paralysis (botulism); rhabdomyolysis |
Approach Summary
Acute paraparesis
├── Sensory level / UMN signs → Spinal cord MRI STAT
│ ├── Compressive? → Surgery/Antibiotics emergency
│ └── Noncompressive? → LP + autoimmune/infectious workup
├── No sensory level, flaccid/areflexic → Cauda equina vs. GBS vs. myopathy
└── Bilateral leg UMN + brain signs → Brain MRI (ACA infarct, SST)
55 Yr 2 episode of seizures and altered sensorium approach to pt .. history and examination
Approach to a 55-Year-Old with 2 Episodes of Seizures + Altered Sensorium
Step 1 — Initial Stabilization (Before History)
- Airway, breathing, circulation
- Capillary blood glucose immediately (hypoglycemia is the most treatable cause)
- IV access, pulse oximetry, cardiac monitor
- GCS score
- Is the patient still seizing? → If so, manage as status epilepticus
Step 2 — HISTORY
A. Confirm It Was a Seizure (Not a Mimic)
- Onset: sudden or gradual?
- Type of movements: tonic? clonic? tonic-clonic? focal limb jerking? head/eye deviation?
- Duration of episode (exact)
- Was there a cry/vocalization at onset?
- Did the patient fall? Sustain injury?
- Skin color: cyanosis, pallor?
- Loss of consciousness: complete or partial?
- Tongue biting (lateral tongue bite → seizure; tip bite → syncope)
- Incontinence (urinary/fecal)
- Post-episode behavior: confusion, drowsiness, Todd's paralysis, headache, amnesia?
- Syncope (preceded by prodrome — nausea, diaphoresis, pallor; recovery rapid)
- Cardiac arrhythmia (ventricular tachycardia; palpitations; ECG abnormality)
- TIA (loss of function, not spreading excitation; no post-ictal confusion)
- Hypoglycemic episode
- Psychogenic non-epileptic seizures (PNES)
- Migraine with aura
B. Characterize the Seizure Type
- Focal onset (aware or impaired awareness) vs. generalized → critical for workup
- Any aura beforehand? Olfactory, gustatory, déjà vu, rising epigastric feeling → temporal lobe
- Visual/sensory aura → occipital/parietal
- Second episode — same or different semiology? What interval?
- Did patient have eye/head deviation at onset? → indicates contralateral frontal focus
C. History of Present Illness
- Fever, headache, neck stiffness, photophobia → meningoencephalitis (urgent)
- Headache (progressive, worse lying flat) → raised ICP, SOL
- Focal weakness, speech disturbance, vision change → structural lesion
- Vomiting → raised ICP
- Recent head trauma (even trivial) → subdural/extradural hematoma
- Altered behavior/personality change over weeks → tumor, encephalitis (autoimmune/viral)
- Fever + rash → HSV encephalitis, bacterial meningitis, CNS vasculitis
- Polyuria, polydipsia → hypo-/hyperglycemia, hyponatremia
- Recent illness / vaccination → ADEM
- Recent travel → neurocysticercosis (endemic areas), cerebral malaria, TB
- Timeline of altered sensorium relative to seizures
D. Past Medical History
| Ask about | Relevance |
|---|---|
| Hypertension, diabetes, CAD, atrial fibrillation | Stroke, hypertensive encephalopathy |
| Prior stroke, TIA | Cortical scar → epileptic focus |
| Known malignancy (breast, lung, colon, kidney, melanoma) | Cerebral metastasis |
| HIV, immunocompromise | CNS lymphoma, CMV, toxoplasmosis, TB, cryptococcal |
| Liver disease (cirrhosis, hepatitis) | Hepatic encephalopathy |
| Renal disease | Uremic encephalopathy, hyponatremia |
| Thyroid disease | Hashimoto's encephalopathy; hypo/hyperthyroidism |
| Autoimmune disease (SLE, vasculitis) | CNS vasculitis |
| Prior seizures in childhood (febrile convulsions) | Lowers threshold |
| Prior brain surgery or CNS infection | Scar epilepsy |
E. Drug and Substance History
| Ask about | Relevance |
|---|---|
| Alcohol history — amount, last drink | Withdrawal seizures (48–72 h after cessation) |
| Benzodiazepines, barbiturates — recent reduction/stop | Withdrawal |
| Recreational drugs (cocaine, amphetamines) | Provoked seizures |
| Prescribed medications | Proconvulsant drugs (tramadol, tricyclics, fluoroquinolones, isoniazid, theophylline, lithium, clozapine) |
| Recent change in antiepileptic drug (AED) | Sub-therapeutic levels |
| Herbal / traditional medicines | CNS toxicity |
F. Family and Social History
- Family history of epilepsy
- Occupation (driver? — implications for treatment)
- Lives alone?
- Sleep deprivation, extreme physical or emotional stress
Step 3 — EXAMINATION
General Examination
| Sign | Suggests |
|---|---|
| Fever | Meningoencephalitis, brain abscess, septic encephalopathy |
| High BP (>180/120) | Hypertensive encephalopathy, posterior reversible encephalopathy syndrome (PRES) |
| Low BP | Sepsis, cardiogenic cause, Addisonian crisis |
| Tachycardia | Cardiac arrhythmia, sepsis, thyroid storm |
| Cyanosis / low SpO₂ | Hypoxic seizure |
| Pallor | Anaemia, blood loss (subdural hematoma) |
| Jaundice | Hepatic encephalopathy |
| Stigmata of chronic liver disease | Hepatic encephalopathy |
| Lymphadenopathy | Lymphoma, malignancy, TB |
| Skin rash | Meningococcal purpura, SLE, HSV, neurofibromatosis, tuberous sclerosis |
| Head trauma signs: Battle's sign, raccoon eyes, haemotympanum, CSF leak | Base of skull fracture → intracranial bleed |
| Tongue laceration (lateral) | Confirms seizure |
| Incontinence signs | |
| Needle marks / drug track marks | Substance abuse |
Neurological Examination (Systematic)
1. Level of Consciousness & Cognition
- GCS (E+V+M) — document precisely
- MMSE / orientation — time, place, person
- Is this true postictal drowsiness or new encephalopathy?
- Postictal state: usually improves steadily over 20–60 min; persisting confusion → structural/metabolic
2. Meningeal Signs
- Neck stiffness (Kernig's sign, Brudzinski's sign) → meningitis, SAH, encephalitis
- Note: may be absent in immunocompromised / elderly
3. Cranial Nerves
| CN | What to look for |
|---|---|
| CN II | Papilloedema (raised ICP), visual field defect |
| CN III, IV, VI | Pupil asymmetry (herniation!), gaze palsy, VI palsy (false localizing, raised ICP) |
| CN VII | Facial asymmetry → frontal lobe lesion (contralateral) |
| CN XII | Tongue deviation |
4. Motor System
- Focal weakness → contralateral structural lesion
- Todd's paralysis — transient hemiparesis after focal seizure (30 min – 36 h); clears spontaneously
- Tone: hypotonia (metabolic/toxic), spasticity (structural)
- Pronator drift
- Plantar response (upgoing Babinski → UMN lesion or postictal)
5. Sensory System
- Hemisensory loss → contralateral parietal lesion
6. Cerebellar
- Ataxia, nystagmus → posterior fossa lesion, drug toxicity (phenytoin, carbamazepine)
7. Deep Tendon Reflexes
- Hyperreflexia + Babinski → UMN lesion
- Hyporeflexia → metabolic, drug effect
8. Fundoscopy (MANDATORY)
- Papilloedema → raised ICP → LP contraindicated before imaging
Differential Diagnosis Framework (55-Year-Old)
Seizures + Altered Sensorium at 55 yrs
│
├── STRUCTURAL (most common in this age)
│ ├── Stroke (ischemic / hemorrhagic)
│ ├── Subdural / extradural hematoma
│ ├── Brain tumor (primary glioma or metastasis)
│ └── Brain abscess / granuloma (TB, NCC)
│
├── METABOLIC / SYSTEMIC
│ ├── Hypo/hyperglycemia
│ ├── Hyponatremia (Na⁺ <125 mEq/L)
│ ├── Uremic encephalopathy
│ ├── Hepatic encephalopathy
│ ├── Hypocalcemia / hypomagnesemia
│ ├── Hypoxia / hypercapnia
│ └── Hypertensive encephalopathy / PRES
│
├── INFECTIVE / INFLAMMATORY
│ ├── Bacterial meningitis
│ ├── Viral encephalitis (HSV most important)
│ ├── Autoimmune encephalitis (anti-NMDAR, LGI1, CASPR2)
│ ├── TB meningoencephalitis
│ └── Cerebral malaria / neurocysticercosis
│
├── TOXIC / DRUG
│ ├── Alcohol withdrawal (48–72 h after last drink)
│ ├── Benzodiazepine/barbiturate withdrawal
│ └── Drug toxicity (proconvulsants)
│
└── VASCULAR
└── Cerebral venous sinus thrombosis (CVST)
Red Flags Demanding Immediate Action
| Red Flag | Action |
|---|---|
| Fever + meningism | LP after imaging → treat empirically for bacterial meningitis + HSV encephalitis BEFORE LP |
| Focal deficits / papilloedema | CT brain before LP |
| Ongoing altered sensorium >30 min post-seizure | Rule out non-convulsive status epilepticus → urgent EEG |
| Severe hypertension + encephalopathy | Treat as PRES / hypertensive emergency |
| Known malignancy | MRI with contrast |
| Anticoagulated / alcoholic / elderly | Exclude intracranial bleed |
| Glucose < 3 mmol/L | IV dextrose immediately |
25 Yr female with wasting of left hand wasting with motor weakness 3 month without sensory involved Differential
25-Year-Old Female: Left Hand Wasting + Pure Motor Weakness (3 months, No Sensory Loss)
Key Diagnostic Features to Lock In
- Young female, 25 years
- Unilateral (left hand)
- Wasting + weakness (lower motor neuron pattern — flaccid, ± fasciculations, ± hyporeflexia)
- 3 months — subacute/chronic, not acute
- No sensory loss — this is the critical differentiating feature
Localization First
| Level | Pattern | Sensory |
|---|---|---|
| Anterior horn cell | Pure LMN wasting, fasciculations, no sensory | Absent (pure motor cells) |
| Anterior root (motor root) | Pure LMN, segmental distribution | Absent |
| Intrinsic cord (syrinx, early) | Dissociated sensory loss + LMN at level | May be absent early |
| Lower trunk / medial cord brachial plexus | C8-T1 wasting | Usually some sensory in medial forearm/hand |
| Pure motor peripheral nerve | Deep palmar ulnar, posterior interosseous | No sensory |
| Muscle | Wasting without reflex change early | No sensory |
Differential Diagnosis (Most Likely to Least in This Patient)
1. Hirayama Disease (Benign Monomelic Amyotrophy / Juvenile Segmental Muscular Atrophy) ⭐ TOP DIAGNOSIS
"The most common presentation is one of an idiopathic, slowly progressive, painless weakness and atrophy in one hand or forearm... The condition remains limited to only a few myotomes." — Bradley and Daroff's Neurology
- Classic age of onset: teens to early 30s
- More common in women in Indian subcontinent (though 60% are male overall)
- Predominantly C7–T1 myotomes → intrinsic hand muscles + forearm
- "Oblique atrophy" pattern — thenar, hypothenar, interossei wasted; brachioradialis spared
- Pure LMN, no sensory loss, no UMN signs, no cranial nerve involvement
- Painless, slow progression over 2–3 years then stabilizes
- Proposed mechanism: dynamic cord compression during neck flexion (disproportionate dural sac growth)
- EMG: active and chronic denervation at C7–T1; NCS show reduced CMAPs, near-normal SNAPs
- MRI cervical spine (dynamic — flexion views): flattening of anterior cord, loss of attachment of posterior dura, asymmetric cord atrophy
2. Cervical Myelopathy — Syringomyelia
"Syringomyelia... damage to the fibers crossing in the anterior commissure destined for the spinothalamic tract... By the time descending tracts are affected, segmental motoneuron and corticospinal tract damage are almost always present." — Bradley and Daroff's
- Syrinx classically causes cape-like dissociated sensory loss (pain/temp lost, proprioception preserved)
- However, early syrinx can present with pure hand wasting (anterior horn cell damage at the level of the syrinx) before sensory fibres are involved
- Associated with Chiari malformation (Type I most common), trauma, tumors, arachnoiditis
- May later develop UMN signs in legs (descending tract involvement)
- 25-year-old female + no sensory involvement yet → must exclude with MRI
- MRI spine: T2 fluid-filled cavity within cord over multiple segments
3. True Neurogenic Thoracic Outlet Syndrome (TOS)
"True neurogenic TOS... compression of the lower trunk (C8/T1)... weakness and wasting of intrinsic muscles of the hand and diminished sensation on the palmar aspect of the fifth digit." — Harrison's Principles
- Caused by anomalous fibrocartilaginous band from elongated C7 transverse process (cervical rib) to first rib
- C8/T1 compression → hand intrinsic wasting
- Pain is mild or absent — can initially appear as pure motor
- Sensory loss on 5th digit/medial forearm — may be minimal or absent early
- Young women, often exacerbated by arm position
- CXR: elongated C7 transverse process / cervical rib
- EMG/NCS: reduced SNAP medial forearm, low CMAP ulnar > median
- Treatment: surgical band resection (wasting usually does not recover but progression halts)
4. Multifocal Motor Neuropathy (MMN) with Conduction Block
"Pure LMN involvement... enters the differential diagnosis of benign focal amyotrophy and the PMA variant of ALS. It is important to search for this since it is treatable." — Bradley and Daroff's
- Autoimmune; anti-GM1 antibodies in ~50%
- Asymmetric, pure motor — starts distally, upper > lower limbs
- No sensory loss (distinguishes from CIDP)
- Fasciculations may be present
- Can begin with focal hand wasting in a young adult
- EMG/NCS: focal conduction block outside carpal tunnel → pathognomonic
- Treatable — high-dose IVIG; this makes the diagnosis essential to establish
- CK mildly elevated; anti-GM1 IgM elevated
5. Compressive Focal Motor Neuropathy
| Nerve Compressed | Pattern |
|---|---|
| Deep palmar branch of ulnar nerve (at Guyon's canal — motor division) | Hypothenar + interossei wasting; no sensory loss |
| Posterior interosseous nerve (radial nerve deep branch) | Wrist/finger extension weakness; no sensory loss |
| Anterior interosseous nerve | Loss of pinch (FPL + FDP index); no sensory loss |
- Relevant in occupational/repetitive trauma
- EMG/NCS confirms level and type
6. Cervical Radiculopathy — C8/T1 Root (Predominantly Motor)
- Disc prolapse or osteophyte compressing C8 or T1 motor root
- Can produce hand intrinsic weakness and wasting
- Sensory involvement is typical but can be minimal or overlooked
- C8: ring/little finger, medial forearm sensory if affected; intrinsic + FDP weakness
- T1: intrinsic hand muscles (abductor pollicis brevis, interossei)
- MRI cervical spine confirms
- 25-year-old: less common but possible (disc herniation)
7. Pancoast Tumor (Superior Sulcus Tumor)
- Lung apex tumor invading lower brachial plexus (C8/T1)
- Progressive hand intrinsic wasting
- Horner's syndrome (ptosis, miosis, anhidrosis) — highly specific association
- Usually painful (shoulder/arm pain)
- Sensory involvement of medial forearm/hand expected
- 25-year-old female: rare but must not miss — especially if smoker
- CXR, CT thorax, MRI brachial plexus
8. Lower Brachial Plexopathy — Other Causes
- Radiation plexopathy (prior radiotherapy)
- Neoplastic infiltration (lymphoma, metastasis — less likely at 25)
- Neuralgic amyotrophy (Parsonage-Turner syndrome) — usually starts with severe pain, then weakness; sensory loss usually follows
9. Spinal Muscular Atrophy (SMA) — Adult Onset
- SMA Type III (Kugelberg-Welander) / Type IV: onset in adulthood possible
- Pure LMN, symmetric or asymmetric, no sensory loss
- Proximal > distal typically, but distal hand involvement can occur
- Slowly progressive
- Genetic: SMN1 deletion/mutation
- Creatine kinase may be elevated
10. Monomelic Motor Neuropathy — Hereditary (CMT Variants)
- Charcot-Marie-Tooth (CMT) — usually bilateral, but rare asymmetric presentations
- Distal hereditary motor neuropathy (dHMN): pure motor, distal wasting, no sensory loss
- Family history may be absent in sporadic cases
- Nerve conduction/genetic testing
Less Likely in a 25-Year-Old Female (but to Exclude)
| Condition | Reason to list |
|---|---|
| ALS | Very unlikely at 25, usually absent UMN signs in early hand-onset PMA variant; rule out |
| Lead poisoning | Pure motor neuropathy; radial nerve ("wrist drop"); occupational exposure |
| Porphyria | Acute intermittent porphyria → pure motor neuropathy; episodic; urine porphyrins |
| Inclusion body myositis | Older patients; long finger flexors + quadriceps; CK elevated |
| Focal myositis | Rare; MRI muscle |
Summary Table
| Diagnosis | Pure Motor? | Age / Sex | Key Feature | Investigation |
|---|---|---|---|---|
| Hirayama disease | ✅ | Young adult, F | Oblique atrophy, stabilizes, neck flexion aggravates | Cervical MRI (flexion views), EMG |
| Syringomyelia | ✅ early | Young adult | Dissociated sensory loss (may be absent early), Chiari | MRI spine |
| Neurogenic TOS | ✅ | Young female | Cervical rib, C7 transverse process | CXR, NCS, EMG |
| MMN | ✅ | Any age | Conduction block, anti-GM1 | NCS (conduction block), anti-GM1 |
| Deep palmar ulnar neuropathy | ✅ | Any | Motor-only branch compression | NCS, EMG |
| C8/T1 radiculopathy | Mostly | Any | Disc prolapse | MRI cervical spine |
| Pancoast tumor | ± | Any | Horner's, shoulder pain | CXR, CT thorax |
| SMA adult | ✅ | Any | SMN1 mutation | Genetic testing, EMG |
| dHMN | ✅ | Young | Family history, bilateral eventually | NCS, genetics |
Priority Investigations
- MRI cervical spine (with dynamic flexion views if Hirayama suspected) — exclude syrinx, Chiari, cord atrophy, disc herniation
- EMG / Nerve conduction studies — localizes to anterior horn vs. root vs. plexus vs. peripheral nerve; identifies conduction block (MMN), characterizes denervation pattern
- Chest X-ray / CT thorax — cervical rib, Pancoast tumor
- Anti-GM1 IgM antibodies — MMN
- Genetic testing (SMN1, PMP22) — if SMA or CMT suspected
- Urine porphyrins — if episodic or occupational exposure
- Serum CK — elevated in myopathic or neurogenic conditions
- Blood lead levels — if occupational risk
Unilateral with pure motor only
Unilateral Hand Wasting — Pure Motor Only (No Sensory)
Anatomical Logic: Where Can a Purely Motor, Unilateral Lesion Sit?
Cortex / Corticospinal tract
↓ (UMN — wasting rare, no fasciculations)
Anterior Horn Cell ←── Pure motor, unilateral = MOST SPECIFIC LEVEL
↓
Anterior (Motor) Root ←── Pure motor if dorsal root spared
↓
Brachial Plexus lower trunk / medial cord
↓ (sensory usually co-involved, but minimal early)
Pure Motor Peripheral Nerve branch
↓ (deep palmar ulnar, AIN, PIN)
Muscle ←── No sensory, but wasting pattern differs
The Focused Differential (Unilateral, Pure Motor, Young Female, Subacute)
1. ⭐ Hirayama Disease (Benign Monomelic Amyotrophy)
- 25-year-old, unilateral hand/forearm wasting, pure LMN, no sensory loss, no UMN signs, no pain
- C7–T1 anterior horn cell degeneration, confined to one limb
- "Oblique atrophy" — all intrinsic hand muscles + forearm flexors wasted, brachioradialis spared (C5/6 — above the lesion)
- Mini-polymyoclonus (finger tremor on extension) — characteristic
- Progression over 2–3 years then arrests spontaneously
- ♀ in Indian subcontinent: less gender bias than in Japan
- No fasciculations at rest typically (distinguishes from ALS)
- EMG: chronic + active denervation C7–T1, normal SNAPs
- MRI cervical spine in neutral AND flexion: asymmetric cord atrophy, loss of posterior dural attachment, anterior displacement of posterior dura on flexion, intramedullary T2 signal at C5–C8
2. Syringomyelia (Early / Eccentric Syrinx)
- An eccentric syrinx can selectively destroy one side's anterior horn cells before crossing fibres or dorsal columns are involved — producing unilateral pure motor wasting
- Associated with Chiari I malformation (common in young women), post-traumatic, idiopathic
- Sensory loss (dissociated — pain/temp only, cape distribution) typically follows later
- Should always be excluded in any young person with unilateral hand wasting
- MRI spine: T2 hyperintense CSF-filled cavity; look for tonsillar descent (Chiari)
3. Multifocal Motor Neuropathy (MMN)
- Pure motor, asymmetric, distal upper limb onset — classic presentation
- Mimics anterior horn cell disease but is demyelinating and treatable
- No sensory loss (distinguishes it from CIDP)
- Unilateral hand onset is well-described
- Anti-GM1 IgM antibodies (~50%)
- NCS: focal conduction block outside standard entrapment sites — pathognomonic
- Responds to high-dose IVIG — critical not to miss
4. Pure Motor Focal Neuropathy (Compressive/Entrapment)
| Nerve | Site | Muscles Wasted | Clue |
|---|---|---|---|
| Deep (motor) branch of ulnar nerve | Guyon's canal (motor division only) | Hypothenar, interossei, adductor pollicis | No sensory loss, occupational/cycle/crutch pressure |
| Anterior interosseous nerve (AIN) | Proximal forearm | FPL, FDP (index), pronator quadratus | "Pinch sign" — can't make O with thumb+index |
| Posterior interosseous nerve (PIN) | Radial tunnel | Finger/wrist extensors | Wrist drop without sensory loss |
- Deep ulnar motor branch = most relevant for intrinsic hand wasting without sensory loss
- Cause: ganglion, repetitive pressure (cyclists, typists), occupational
5. Neurogenic Thoracic Outlet Syndrome (True TOS)
- Anomalous fibrocartilaginous band, elongated C7 transverse process / cervical rib → compresses lower trunk (C8/T1)
- Wasting of intrinsic hand muscles, predominantly motor
- Sensory loss (medial forearm, 5th digit) is classically mild or absent — can appear pure motor
- Young women are disproportionately affected
- CXR: elongated C7 transverse process
- NCS/EMG: reduced CMAP ulnar > median; reduced SNAP medial forearm (if sensory affected at all)
6. C8 or T1 Motor Root Compression (Radiculopathy — Motor Predominant)
- Cervical disc herniation compressing C8 or T1 root
- Dorsal (sensory) root can be spared if compression is purely anterior (ventral root lesion)
- Hand intrinsic wasting (T1) or FDP/FPL weakness (C8)
- Young adults: soft disc prolapse possible
- MRI cervical spine confirms
7. Spinal Muscular Atrophy (SMA) — Focal / Asymmetric Variant
- Adult-onset SMA (Type III/IV) or distal hereditary motor neuropathy (dHMN) can start asymmetrically
- Pure LMN, no sensory loss — by definition
- Family history may be absent
- SMN1 gene testing; EMG shows widespread chronic denervation beyond clinically affected limb
8. Monomelic Amyotrophy Secondary to Intrinsic Cord Lesion
- Intramedullary tumor (ependymoma, astrocytoma) at cervical cord level
- Selective anterior horn involvement before sensory tracts affected
- Rare but must be excluded with MRI
What Makes This NOT ALS
| Feature | This Patient | ALS |
|---|---|---|
| Age | 25 ♀ | Usually >40 |
| Distribution | Unilateral hand, confined | Spreads relentlessly |
| UMN signs | Absent | Usually present (brisk reflexes, Babinski) |
| Bulbar | Absent | Develops |
| Progression | 3 months, stable hand | Relentless progression |
| Fasciculations | Not mentioned | Widespread |
Ranked Summary
| Rank | Diagnosis | Key Distinguishing Feature |
|---|---|---|
| 1 | Hirayama disease | Young, oblique atrophy, arrests, dynamic MRI |
| 2 | Syringomyelia (early eccentric) | MRI cord signal, Chiari |
| 3 | MMN | Conduction block on NCS, anti-GM1, treatable |
| 4 | Deep ulnar motor branch neuropathy | Hypothenar + interossei only, occupational |
| 5 | True neurogenic TOS | Cervical rib, C8/T1, young female |
| 6 | C8/T1 radiculopathy | MRI disc prolapse |
| 7 | SMA / dHMN | Genetic, EMG beyond affected limb |
| 8 | Intramedullary tumor | MRI cord |
Minimum Workup
- MRI cervical spine — neutral + flexion (Hirayama), T2 (syrinx, Chiari, tumor, disc)
- EMG + NCS — pattern of denervation, conduction block, SNAP intact?
- Anti-GM1 IgM — MMN
- CXR — cervical rib / elongated C7 transverse process
- SMN1 gene test — if EMG shows widespread denervation beyond one limb
Procide in case of meningitis with raised ict and how to collect csf in large hydrocephalus case
Procedure in Meningitis with Raised ICP + CSF Collection in Hydrocephalus
PART 1: Approach to LP in Suspected Meningitis with Raised ICP
The Core Dilemma
"Antibiotics should not be delayed awaiting successful lumbar puncture. Antibiotics will not affect PCR or bacterial antigen testing." — Rosen's Emergency Medicine
Step 1 — Start Empirical Treatment IMMEDIATELY
| Drug | Dose | Target |
|---|---|---|
| Ceftriaxone | 2 g IV q12h | S. pneumoniae, N. meningitidis, H. influenzae |
| Vancomycin | 40–60 mg/kg/day ÷ q8–12h | Resistant pneumococcus |
| Ampicillin | 2 g IV q4h | Add if age >50, immunocompromised, or Listeria suspected |
| Dexamethasone | 0.15 mg/kg q6h × 4 days | Start with or just before first antibiotic dose → reduces mortality and neurological sequelae in pneumococcal meningitis |
| Aciclovir | 10 mg/kg IV q8h | If HSV encephalitis cannot be excluded |
If blood cultures can be drawn within 10 minutes — do so before antibiotics. If not feasible, give antibiotics first.
Step 2 — Identify Features of Raised ICP / Risk of Herniation
| Feature | Why Dangerous |
|---|---|
| Papilloedema on fundoscopy | Confirms raised ICP |
| New focal neurological deficit | Suggests mass lesion |
| Depressed consciousness (GCS ≤12) | Impaired autoregulation |
| Seizure within last 1 week | May indicate focal lesion |
| Immunocompromised state (HIV, transplant, steroids) | Atypical mass lesion (toxoplasmosis, lymphoma) |
| Known CNS lesion / SOL | Obvious |
| Abnormal posturing / decerebrate | Impending herniation |
Step 3 — Performing the LP Safely When ICP is Raised
- No midline shift, no mass lesion, no herniation → LP can proceed, but with precautions
- Signs of herniation / large mass / obliterated cisterns → LP is contraindicated (see alternative CSF collection below)
Safe LP Technique When ICP is Elevated:
-
Position: Lateral decubitus (left lateral) — never sitting position when ICP is raised (sitting raises CSF pressure further at lumbar level)
-
Needle: Use a pencil-point (atraumatic) spinal needle (Whitacre 22G) — lower risk of post-LP herniation than cutting needle; smaller bore
-
Level: L3–L4 or L4–L5 interspace (below the conus at L1–L2)
-
Stylet IN: Always remove stylet slowly, never rapidly decompress
-
Measure opening pressure: Normal <20 cm H₂O; in meningitis often 20–40+ cm H₂O
-
Volume removed: Collect minimum volume necessary (3–4 tubes, ~8–12 mL total) — do not open tap and let CSF drain freely
-
Do NOT drain large volumes — risk of downward herniation
-
Mannitol cover: If opening pressure >40 cm H₂O or patient deteriorates during LP:
- Stop immediately
- Give Mannitol 0.5–1 g/kg IV over 20 minutes
- Consider neurosurgical consult for EVD
-
After LP: Keep patient flat for 1 hour; monitor closely for signs of coning (Cushing's triad — hypertension, bradycardia, irregular respirations)
Step 4 — Managing ICP in Meningitis (Adjunctive Measures)
| Intervention | Indication / Details |
|---|---|
| Head elevation 30° | Reduces ICP while maintaining cerebral perfusion |
| Mannitol 20% (0.5–1 g/kg IV) | Acute ICP rise; osmotic diuresis; duration 3–4 hours |
| Hypertonic saline (3%) | Alternative to mannitol; preferred in hypovolemic patients |
| Avoid hypotonic fluids | Use isotonic NS for maintenance |
| Hyperventilation (PCO₂ 30–35 mmHg) | Temporary bridge only; vasoconstriction reduces CBF |
| Dexamethasone | Reduces cerebral oedema in bacterial meningitis |
| Avoid hyperthermia | Fever worsens ICP; paracetamol/cooling |
| Avoid hyponatraemia | SIADH common in meningitis; fluid restriction if Na falls |
| External ventricular drain (EVD) | If obstructive hydrocephalus develops; provides ICP monitoring + CSF drainage |
When LP is Absolutely Contraindicated in Meningitis
| Condition | Action |
|---|---|
| CT shows transtentorial herniation / uncal herniation | NO LP; treat ICP; consider EVD |
| Posterior fossa mass / cerebellar herniation risk | NO LP (most dangerous) |
| Overlying skin infection at LP site | Avoid direct LP; consider C1–C2 lateral cervical puncture by neurosurgeon |
| Thrombocytopenia < 20,000 or coagulopathy (INR >1.5) | Correct first; or obtain CSF from EVD if already in situ |
PART 2: CSF Collection in Large / Obstructive Hydrocephalus
Option 1 — External Ventricular Drain (EVD) / Ventriculostomy
- Kocher's point (most common site): 1 cm anterior to the coronal suture, 2–3 cm lateral to midline (mid-pupillary line) on the non-dominant side
- Catheter placed into the frontal horn of the lateral ventricle
- Provides:
- Direct CSF sampling (ventricular CSF in meningitis) — highest diagnostic yield
- Continuous ICP monitoring
- Therapeutic CSF drainage to control ICP
- Note: ventricular CSF in meningitis may show higher cell counts, lower glucose, higher protein than lumbar CSF — interpret accordingly
Option 2 — Sampling Via Existing VP Shunt / Reservoir
- Shunt tap (by neurosurgeon or trained neurologist):
- Insert 23–25G butterfly needle into the shunt reservoir under sterile conditions
- Aspirate 2–3 mL CSF gently (do not aspirate hard — risk of pulling choroid plexus)
- Send for cell count, protein, glucose, culture, sensitivity
- Also culture the shunt hardware itself if shunt infection suspected
- The shunt itself may be the source of infection (S. epidermidis, S. aureus — shunt meningitis)
Option 3 — C1–C2 Lateral Cervical Puncture (Cisternal Puncture)
- Performed under fluoroscopic guidance between C1 and C2 vertebrae
- Accesses the lateral cervical subarachnoid space
- Used when:
- LP site infected / impossible
- Communicating hydrocephalus but lumbar route blocked
- Requires experienced operator (neurosurgery/interventional radiology)
Option 4 — Cisternal Puncture (Suboccipital)
- Needle inserted into the cisterna magna (suboccipital approach)
- Access between the posterior arch of C1 and the foramen magnum
- Rarely used; significant risk of brainstem injury if not performed by an expert
- Reserved for special circumstances (lumbar block, spinal deformity)
Summary Flowchart
Suspected Meningitis
|
↓
IMMEDIATELY: Blood cultures + empirical antibiotics + dexamethasone + aciclovir
|
↓
Any risk features for raised ICP?
(focal signs, papilloedema, GCS≤12, immunocompromised, seizure)
|
YES | NO
| → LP immediately (lateral decubitus, thin needle, minimal volume)
↓
CT Brain STAT
|
No herniation → LP with ICP precautions
|
Herniation / obstructive hydrocephalus
|
↓
NEUROSURGERY: EVD / shunt tap / Ommaya reservoir
↓
Ventricular CSF sent for analysis + culture
ICP controlled with EVD drainage
Peripheral vertigo vs central vertigo
Peripheral Vertigo vs. Central Vertigo
Anatomy in Brief
| Peripheral | Central | |
|---|---|---|
| Lesion site | Labyrinth (inner ear) or VIII cranial nerve (up to root entry zone) | Brainstem (vestibular nuclei) or cerebellum or their connections |
| Common structures | Semicircular canals, utricle, saccule, vestibular nerve | Lateral medulla, pons, cerebellum, 4th ventricle |
Master Comparison Table
| Feature | Peripheral | Central |
|---|---|---|
| Onset | Sudden, abrupt | Gradual or sudden (sudden in stroke) |
| Severity of vertigo | Severe, intense rotational sensation | Mild to moderate (can be severe in hemorrhage/stroke) |
| Duration | BPPV: seconds (<1 min); Neuritis: hours to days | TIA: minutes; others: weeks to months (continuous) |
| Fatigability | Yes — diminishes with repeated positioning (BPPV) | No — persistent, non-fatigable |
| Effect of head position | Strongly positional (BPPV); aggravated by movement | Usually little change with position |
| Nausea/vomiting | Severe, prominent | Variable, often milder |
| Imbalance / gait | Mild–moderate; patient can stand; veers toward lesion side | Severe; patient often cannot stand or walk without support |
| Nystagmus direction | Unidirectional — fixed fast phase direction; horizontal ± torsional | Direction-changing on lateral gaze; may be purely vertical or purely torsional |
| Fixation effect | Suppressed by visual fixation | Not suppressed by fixation |
| Latency after positioning | 2–20 seconds | Brief / immediate |
| Habituation | Yes — fatigues with repeat maneuvers | No |
| Hearing loss / tinnitus | Present in labyrinthitis, Ménière disease | Rare (except in AICA infarction) |
| Neurological signs | Absent | Usually present — dysarthria, dysphagia, diplopia, facial numbness, limb ataxia, weakness |
| Head impulse test | Positive (corrective saccade — vestibular nerve dysfunction) | Negative (eyes hold fixation — central compensation) |
| Recovery | Rapid (days–weeks with vestibular neuritis) | Slow |
Nystagmus — The Key Discriminator
"Spontaneous nystagmus of peripheral origin is typically horizontal or horizontal-torsional and does not change direction with gaze. Spontaneous nystagmus of central origin can be purely vertical or torsional and usually changes direction with changes in gaze." — Cummings Otolaryngology
| Nystagmus Feature | Peripheral | Central |
|---|---|---|
| Direction | Horizontal ± torsional (mixed) | Purely vertical, purely torsional, or direction-changing |
| Direction change with gaze | No — always beats to same side regardless of gaze | Yes — changes direction with direction of gaze |
| Fixation | Suppressed (Alexander's law) | Not suppressed (persists with fixation) |
| Latency on Dix-Hallpike | 2–20 seconds | Immediate / no latency |
| Fatigability on repeat testing | Yes | No |
| Purely downbeating nystagmus | Never | Central (cervicomedullary junction, Arnold-Chiari) |
| Purely upbeating nystagmus | Never | Central (brainstem) |
| See-saw nystagmus | Never | Central (parasellar, midbrain) |
The HINTS Exam (Bedside — For Acute Vestibular Syndrome)
| Component | Peripheral (Reassuring) | Central (Alarming) |
|---|---|---|
| H — Head Impulse Test | Positive (corrective catch-up saccade) | Negative (no saccade — eyes stay fixed) |
| IN — Nystagmus | Unidirectional, horizontal | Direction-changing with lateral gaze |
| TS — Test of Skew | Absent skew deviation | Present vertical skew (ocular misalignment on cover test) |
HINTS positive for central = negative HIT + direction-changing nystagmus + skew deviation → stroke until proven otherwise → MRI DWI urgently
⚠️ HINTS should only be used in acute vestibular syndrome (constant vertigo); not valid in BPPV. Requires experienced examiner.
Causes
Peripheral Vertigo Causes
| Condition | Key Features |
|---|---|
| BPPV (most common overall) | Brief (<1 min), positional, posterior semicircular canal; positive Dix-Hallpike → upbeat + torsional nystagmus; treat with Epley maneuver |
| Vestibular neuritis | Acute severe sustained vertigo, hours to days; post-viral; no hearing loss; positive HIT; spontaneous horizontal nystagmus beating away from lesion |
| Labyrinthitis | Same as neuritis + hearing loss (cochlear involvement) |
| Ménière disease | Triad: recurrent episodic vertigo (hours) + unilateral sensorineural hearing loss + tinnitus ± ear fullness; endolymphatic hydrops |
| Perilymphatic fistula | Post-Valsalva / trauma; pressure-related vertigo |
| Acoustic neuroma (vestibular schwannoma) | Progressive unilateral hearing loss + vertigo; VIII nerve |
| Otosclerosis, chronic otitis | Middle ear disease with vestibular involvement |
| Drug toxicity | Aminoglycosides, cisplatin, furosemide — ototoxic |
Central Vertigo Causes
| Condition | Key Features |
|---|---|
| Vertebrobasilar TIA/stroke | Elderly + atherosclerosis; vertigo + neurological symptoms; HINTS negative HIT; MRI DWI |
| Wallenberg syndrome (PICA infarction) | Vertigo + ipsilateral facial numbness + contralateral body pain/temp loss + dysphagia + Horner's + ataxia |
| AICA infarction | Vertigo + ipsilateral hearing loss + facial palsy + cerebellar signs |
| Cerebellar hemorrhage | Sudden severe vertigo + headache + vomiting + inability to stand; emergency (decompression needed) |
| Multiple sclerosis | Young adult; vertigo from demyelinating plaque in vestibular nuclei; INO often present |
| Vestibular migraine | Most common central cause overall; recurrent vertigo with migrainous features; no fixed neurological signs |
| Brainstem tumor | Progressive; associated cranial nerve palsies |
| Posterior fossa tumors | Medulloblastoma, ependymoma — children; vertigo + papilloedema |
| Arnold-Chiari malformation | Downbeat nystagmus; neck-position-related |
| Wernicke's encephalopathy | Triad: vertigo/ataxia + confusion + ophthalmoplegia; thiamine deficiency |
Dix-Hallpike Test (Peripheral vs. Central Positional Vertigo)
| Feature | Peripheral (BPPV) | Central Positional |
|---|---|---|
| Latency | 2–20 seconds | Immediate / none |
| Nystagmus | Upbeat + torsional (toward lower ear) | Variable, any direction |
| Duration | <60 seconds, stops spontaneously | Persists >60 seconds |
| Fatigues on repeat | Yes | No |
| Patient subjective vertigo | Severe, matches nystagmus | May be mild despite nystagmus |
Clinical Danger Signs — "This is Central Until Proven Otherwise"
| Red Flag | Think |
|---|---|
| Negative head impulse test in acute continuous vertigo | Posterior fossa stroke |
| Direction-changing nystagmus | Cerebellar/brainstem |
| Purely vertical nystagmus (downbeat or upbeat) | Central (never peripheral) |
| Severe truncal ataxia — cannot walk at all | Cerebellar stroke/hemorrhage |
| Vertical skew deviation | Brainstem |
| New neurological symptoms: diplopia, dysarthria, dysphagia, facial numbness, limb weakness | Posterior circulation |
| Sudden onset severe headache + vertigo | Cerebellar hemorrhage → CT STAT |
| Hearing loss + ipsilateral facial palsy + vertigo | AICA infarction |
| Known vascular risk factors (age, hypertension, DM, smoker) | Vertebrobasilar disease |
Summary Mnemonic: "CENTRAL is DANGEROUS"
| Peripheral | Central | |
|---|---|---|
| Nystagmus | Unidirectional | Direction-changing |
| Ataxia | Mild | Able to walk? No |
| Neurological signs | None | Present |
| Gaze suppression | Gone (fixation suppresses) | Remains despite fixation |
| Ear symptoms | Present (hearing loss, tinnitus) | Absent |
| Recovery | Rapid | Often slow |
| Onset | Often positional | Unprovoked or continuous |
| Urge to treat | Epley, betahistine | Surgery, thrombolysis, steroids |
Convulsive status epilepticus vs non Convulsive status epilepticus crisp
Convulsive vs. Non-Convulsive Status Epilepticus
Definition
- t1 (5 min) = treat now (abnormal, self-termination unlikely)
- t2 (30 min) = long-term neuronal injury begins
Master Comparison Table
| Feature | Convulsive SE (CSE) | Non-Convulsive SE (NCSE) |
|---|---|---|
| Definition | Continuous or repetitive tonic-clonic motor activity ≥5 min with impaired consciousness | Electrographic seizure activity ≥30 min with altered behavior/cognition but no prominent motor activity |
| Consciousness | Lost — unresponsive | Altered but variable — confusion, staring, automatisms; may appear awake |
| Motor features | Prominent — tonic-clonic jerking, rigidity | Absent or minimal — subtle twitching, eye deviation, facial myoclonus only |
| Visibility | Obvious — cannot miss it | Occult — easily missed; "encephalopathy" in disguise |
| EEG necessity | Confirms and monitors; clinical diagnosis possible | EEG is mandatory — cannot diagnose without it |
| Urgency | Immediate life-threatening emergency | Also emergency, but NCSE with coma is particularly resistant and deadly |
| Mortality | ~20% | NCSE without coma: lower; NCSE with coma: ~50–60% |
| Prognosis | Bad if delayed; better if treated early | Worse overall — diagnosis delayed, treatment less effective |
| Systemic effects | Severe — hyperthermia, acidosis, rhabdomyolysis, aspiration | Milder systemic effects; neuronal injury still occurs |
Types (ILAE Classification)
Convulsive SE
- Generalized tonic-clonic SE — most dangerous; bilateral motor activity + LOC
- Focal motor SE (including epilepsia partialis continua) — unilateral jerking; consciousness may be preserved
- Tonic SE — sustained stiffening; often in Lennox-Gastaut
- Myoclonic SE with coma — post-anoxic; very poor prognosis
Non-Convulsive SE
| Type | Consciousness | Behavior | Setting |
|---|---|---|---|
| Absence SE (generalized) | Present but slowed | Staring, slow responses, unresponsive to complex commands | Childhood/adolescence; classic EEG 3 Hz spike-wave |
| Focal NCSE with impaired consciousness | Impaired | Automatisms, confusion, cycling fluctuations | Temporal lobe origin most common |
| Focal NCSE without impaired consciousness (aura continua) | Intact | Sensory/psychic symptoms only | Patient aware throughout |
| NCSE with coma | Absent | Comatose; subtle signs only (eye deviation, small twitches) | Post-CSE, post-anoxia, ICU patients; worst prognosis |
EEG Patterns
| SE Type | EEG Pattern |
|---|---|
| Active CSE | Continuous high-voltage rhythmic discharge |
| Subtle CSE (late) | Periodic discharges on flat background — most dangerous stage; motor activity may have ceased but brain still seizing |
| Absence SE | Continuous or near-continuous 3 Hz generalized spike-and-wave |
| Focal NCSE | Rhythmic focal ictal discharges; may wax and wane |
| NCSE with coma | Continuous or nearly continuous epileptiform activity; diagnosis requires clinical–EEG correlation + therapeutic trial |
"The definitive diagnosis of NCSE requires EEG confirmation. Even CSE must be differentiated from psychogenic status epilepticus, which may require video-EEG." — Bradley and Daroff's
"8% of comatose patients in the ICU are found to be in NCSE — continuous EEG monitoring is essential." — Plum and Posner
Clinical Clues to NCSE
- Prolonged postictal confusion (>30–60 min after apparent seizure cessation)
- Unexplained altered consciousness / encephalopathy in ICU
- Coma of unknown cause
- Subtle motor signs: eye deviation, repetitive eye blinking, facial twitching, subtle limb myoclonus
- "Waxing and waning" consciousness
- Known epilepsy with unexplained behavioural change
- Failure to regain consciousness after treatment of CSE → suspect subtle CSE / NCSE with coma
Treatment Protocol
Phase 1 — Stabilization (0–5 min)
- ABC, IV access, O₂, glucose check (give 50 mL 50% dextrose if low + thiamine 100 mg IV)
- Vital signs, cardiac monitor
Phase 2 — Initial Therapy (5–20 min) — Benzodiazepines
| Drug | Dose | Route |
|---|---|---|
| Lorazepam | 0.1 mg/kg IV (max 4 mg; repeat × 1) | IV (preferred) |
| Midazolam | 0.2 mg/kg IM (max 10 mg) | IM (if no IV access — equally effective) |
| Diazepam | 0.15 mg/kg IV OR 0.2 mg/kg rectal | IV or rectal |
Lorazepam 0.1 mg/kg IV controls CSE in 64.9% of cases within 20 min (VA Cooperative Study)
Phase 3 — Second-Line Agents (20–40 min, if benzodiazepines fail)
| Drug | Dose |
|---|---|
| Levetiracetam | 60 mg/kg IV (max 4500 mg) over 10 min |
| Valproate | 40 mg/kg IV (max 3000 mg) over 10 min |
| Fosphenytoin | 20 mg/kg PE IV at 150 mg PE/min |
| Phenobarbital | 15 mg/kg IV at 60 mg/min |
Phase 4 — Refractory SE (>40 min, failed 2 agents)
- Midazolam infusion 0.2 mg/kg bolus → 0.05–2 mg/kg/h
- Propofol 2 mg/kg bolus → 5–10 mg/kg/h (caution: propofol infusion syndrome)
- Thiopental/pentobarbital coma — burst-suppression target
Phase 5 — Super-Refractory SE (>24 h on anaesthetic infusion)
- Ketamine infusion
- Inhaled isoflurane
- Immunotherapy (steroids, IVIG, plasmapheresis — if autoimmune encephalitis suspected)
- Ketogenic diet
- Therapeutic hypothermia
Key Differences — Crisp Summary
| CSE | NCSE | |
|---|---|---|
| Diagnosis | Clinical | EEG mandatory |
| Visibility | Obvious | Hidden — easily confused with encephalopathy |
| Motor activity | Prominent | Minimal/absent |
| ICU prevalence | Presents acutely | 8% of unexplained coma |
| NCSE with coma | N/A | Worst prognosis; post-anoxic, post-CSE |
| Treatment response | Better to benzodiazepines (65%) | Poorer, especially with coma (18%) |
| Systemic complications | Severe (acidosis, rhabdomyolysis, hyperthermia) | Less systemic; neuronal injury ongoing |
| EEG monitoring after CSE treatment | Recommended | Mandatory |
Cryptococal meningitis crisp and diagnosis and rx details
Cryptococcal Meningitis
Organism & Epidemiology
- Cryptococcus neoformans — encapsulated basidiomycete yeast; C. gattii in immunocompetent hosts
- Ubiquitous in soil, pigeon droppings; inhalation → primary pulmonary infection → haematogenous spread to CNS
- Most common AIDS-defining meningitis globally; most common cause of adult meningitis in Sub-Saharan Africa
- Occurs when CD4+ count <100 cells/μL in HIV; also affects transplant recipients, haematologic malignancies, high-dose steroids
- Universally fatal if untreated
Pathophysiology
- Inhibits phagocytosis
- Reduces inflammation → CSF often has surprisingly few cells (minimal pleocytosis)
- Accumulates in Virchow-Robin spaces → gelatinous pseudocysts in basal ganglia
- Blocks CSF resorption → raised ICP — the primary cause of death and neurological damage
Clinical Features
| Feature | Detail |
|---|---|
| Headache | Most common presenting symptom; progressive, severe |
| Fever | Often low-grade or absent |
| Meningism | Present in only ~50% — often ABSENT, especially in HIV |
| Altered consciousness | Confusion, personality change, cognitive impairment |
| Cranial nerve palsies | II (vision), VI, VII — from raised ICP or basilar involvement |
| Photophobia | Present |
| Papilloedema | Raised ICP |
| Seizures | Less common |
| Coma | Late/severe disease |
⚠️ Classic meningeal signs may be absent in >50% of immunocompromised patients. Think cryptococcal meningitis in any HIV patient with headache.
MRI Brain
Diagnosis
CSF Analysis — Key Tests
| Test | Sensitivity (HIV) | Sensitivity (non-HIV) | Notes |
|---|---|---|---|
| Cryptococcal antigen (CrAg) — CSF | ~100% | 86–95% | Rapid, specific; test of choice |
| India ink | 82% | ~50% | Positive = characteristic halo around encapsulated yeast |
| Fungal culture | 100% | ~90% | Gold standard but takes weeks |
| Gram stain | Lower | — | Weakly Gram-positive; often not visualised |
| Serum CrAg | ~100% | — | Excellent screening test; use in all HIV patients with CD4 <100 |
CSF Biochemistry (Typical Pattern)
| Parameter | Finding |
|---|---|
| Opening pressure | Elevated (often >25 cm H₂O; may be >40) |
| WBC | Minimal — 0–50 cells/μL (mononuclear); sometimes normal |
| Protein | Elevated |
| Glucose | Low (hypoglycorrhachia) |
| India ink | Encapsulated budding yeast with clear halo |
Low CSF cell count + high antigen titre = poor prognosis (immune system not reacting)
Other Diagnostic Points
- Lateral flow assay (LFA) — point-of-care CrAg test; rapid, cheap, field-deployable
- β-D-glucan: NOT useful for Cryptococcus (useful for other fungi)
- Screen all HIV patients with CD4 <100 with serum CrAg before ART initiation
Poor Prognostic Features
- Impaired consciousness at presentation
- Raised ICP / hydrocephalus
- CSF CrAg titre >1:1024
- Low CSF WBC (<20 cells/μL) — reflects poor host immune response
- Positive India ink on CSF
- High fungal burden
- Mortality: 10–25% in resource-rich settings; up to 43% in resource-poor settings
Treatment
Phase 1 — Induction (2 weeks)
| Drug | Dose | Route | Duration |
|---|---|---|---|
| Liposomal Amphotericin B | 3–4 mg/kg/day | IV | 2 weeks |
| + Flucytosine (5-FC) | 100 mg/kg/day ÷ q6h | Oral | 2 weeks |
Liposomal AmB preferred over AmB deoxycholate — less nephrotoxicity
- AmB deoxycholate 0.7–1 mg/kg/day IV + fluconazole 800 mg/day
- Daily renal function, electrolytes (K⁺, Mg²⁺) — amphotericin causes nephrotoxicity, hypokalemia, hypomagnesemia
- FBC (flucytosine → bone marrow suppression, especially in HIV)
- Flucytosine levels if available (target 40–60 μg/mL)
Phase 2 — Consolidation (8 weeks)
| Drug | Dose | Duration |
|---|---|---|
| Fluconazole | 400 mg/day orally | 8 weeks |
Phase 3 — Maintenance / Secondary Prophylaxis
| Drug | Dose | Duration |
|---|---|---|
| Fluconazole | 200 mg/day orally | Until CD4 >200 cells/μL sustained for ≥6 months on ART |
Without maintenance therapy → relapse in >50% of patients
Management of Raised ICP (Critical)
| Intervention | Detail |
|---|---|
| Measure opening pressure at every LP | Treat if >25 cm H₂O |
| Therapeutic LP (repeated) | Remove 20–30 mL CSF; repeat daily until pressure normalises; associated with improved survival (COAT trial) |
| Lumbar drain | If daily LPs are not sufficient |
| VP shunt | If LP contraindicated or severe refractory hydrocephalus |
| Acetazolamide | May help as adjunct |
| Optic nerve sheath fenestration | If visual loss from raised ICP |
| ❌ Corticosteroids | NOT routinely recommended — no benefit and possible harm in cryptococcal meningitis (unlike bacterial meningitis) |
| ❌ Mannitol | Not effective for chronic raised ICP in this setting |
ART Timing in HIV (Critical — COAT Trial)
Starting ART within 1–2 weeks of beginning antifungal therapy increased 26-week mortality to 45% vs. 30% if ART delayed to 5 weeks (HR 1.73; COAT trial 2014)
IRIS in Cryptococcal Meningitis
- Occurs weeks to months after ART initiation as CD4 count recovers
- Paradoxical worsening of symptoms (headache, fever, lymphadenopathy, neurological deterioration)
- Treat with corticosteroids (dexamethasone or prednisolone) + continued antifungals
- Do not stop ART
Diagnostic Sensitivity Summary
| Test | AIDS | Non-AIDS |
|---|---|---|
| CrAg (CSF/serum) | ~100% | 86–95% |
| India ink | 82% | 50% |
| Culture | 100% | 90% |
Crisp Summary
Cryptococcal Meningitis
│
├── Who: HIV (CD4 <100), transplant, steroids
├── Organism: C. neoformans (encapsulated yeast)
├── Classic: headache + raised ICP ± minimal meningism
├── Diagnose: CSF CrAg (>90%) + India ink + culture
│
├── TREAT:
│ Induction (2 wks): Liposomal AmB 3–4 mg/kg/day + Flucytosine 100 mg/kg/day
│ Consolidation (8 wks): Fluconazole 400 mg/day
│ Maintenance: Fluconazole 200 mg/day until CD4 >200 × 6 months
│
├── ICP: Daily therapeutic LPs → target normal pressure
├── ART: Delay ≥5 weeks (COAT trial)
└── Mortality: 10–43% despite treatment
Mri basal ganglia exudates images and Differential
MRI basal ganglia lesion T2 hyperintensity exudate
cryptococcal meningitis basal ganglia pseudocysts gelatinous MRI
basal ganglia ring enhancing lesion toxoplasmosis abscess MRI brain
basal ganglia signal change Wilson disease metabolic stroke MRI bilateral
MRI Basal Ganglia Lesions — Images & Differential Diagnosis
How to Approach Basal Ganglia Lesions on MRI
- Unilateral or bilateral?
- What is the signal pattern? (T2 bright, T1 bright/dark, ring enhancing, non-enhancing)
- Is there restricted diffusion (DWI)?
- Clinical context? (Age, immunocompromise, toxic exposure, metabolic disease)
Image Gallery
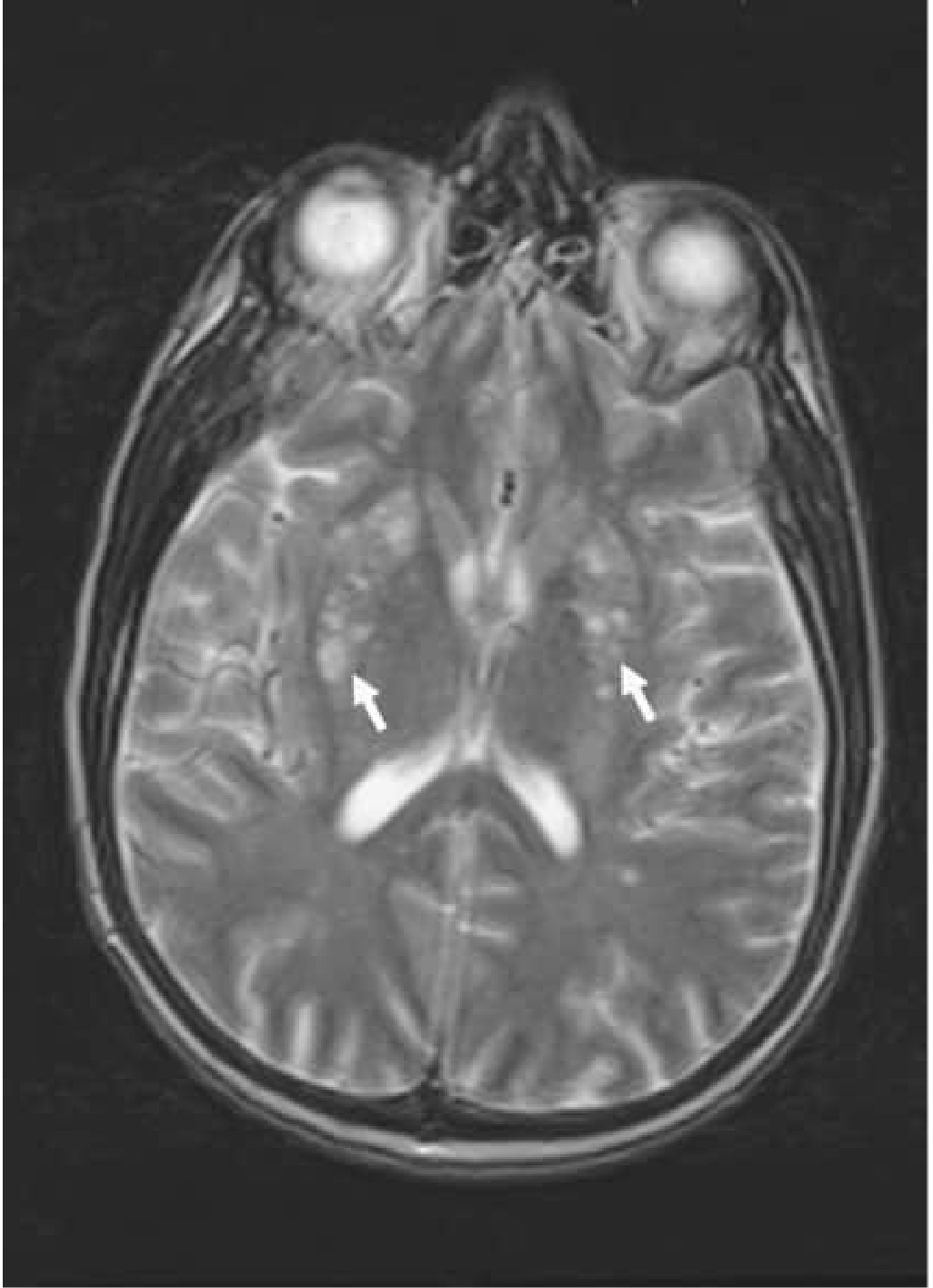
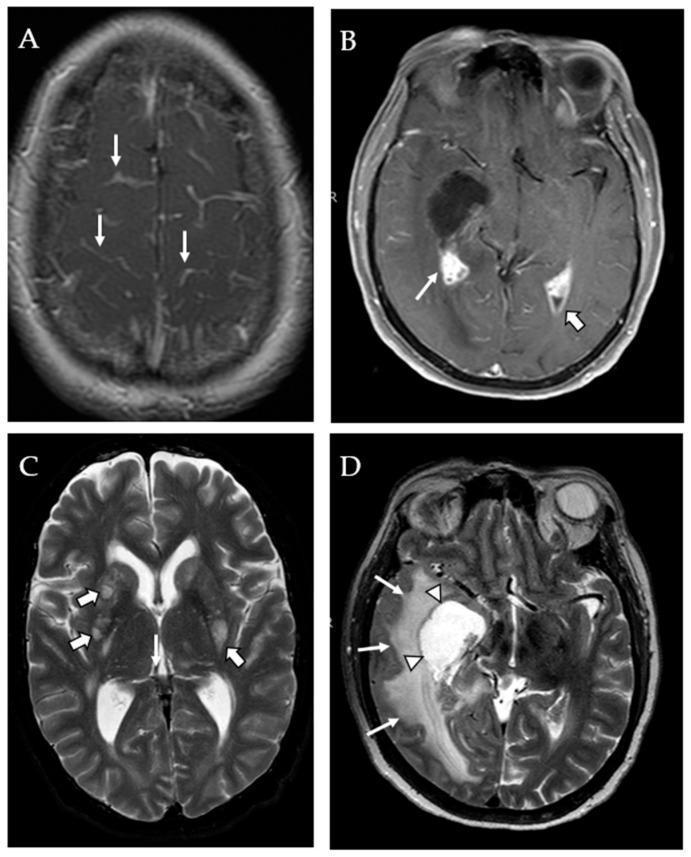
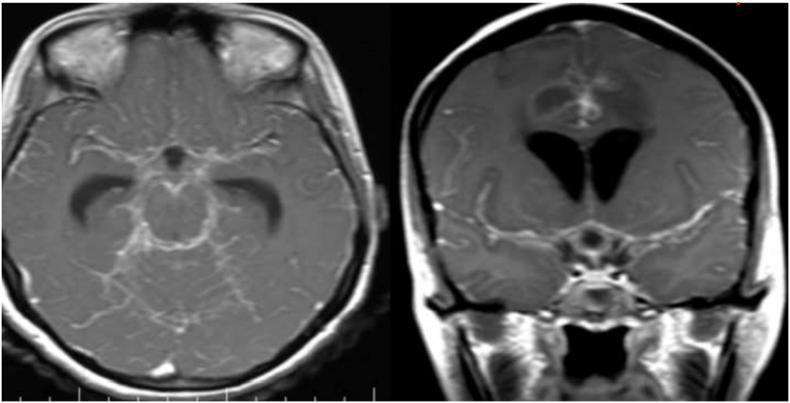
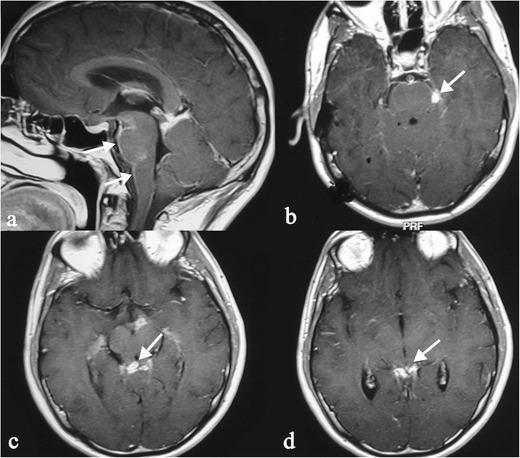
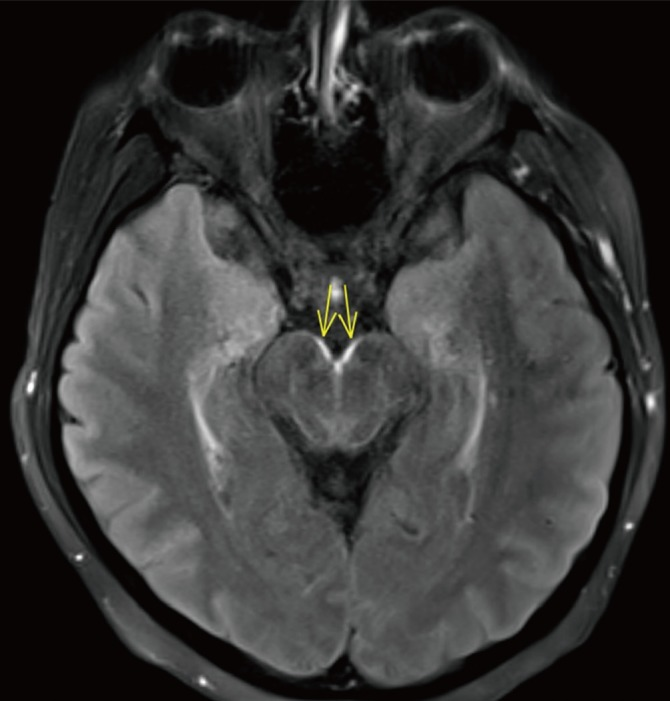
1. Cryptococcal Meningitis — Gelatinous Pseudocysts
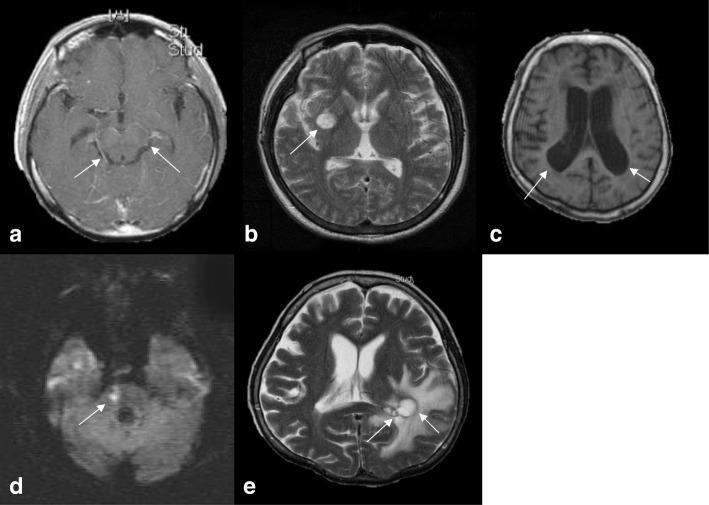
2. Cryptococcal Meningitis — Dilated Virchow-Robin Spaces (Perivascular Pseudocysts)
3. Cerebral Toxoplasmosis — Ring-Enhancing Lesions in Basal Ganglia
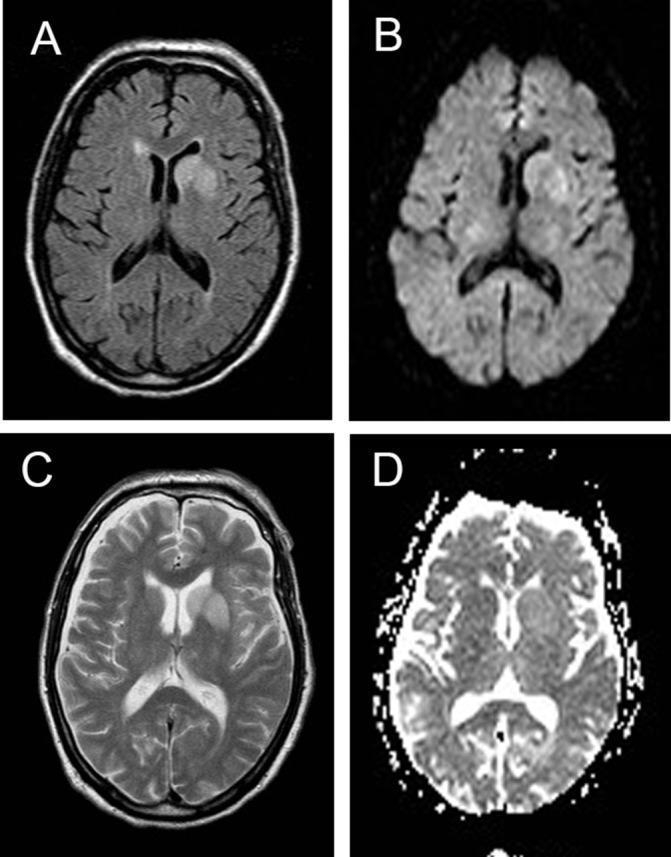
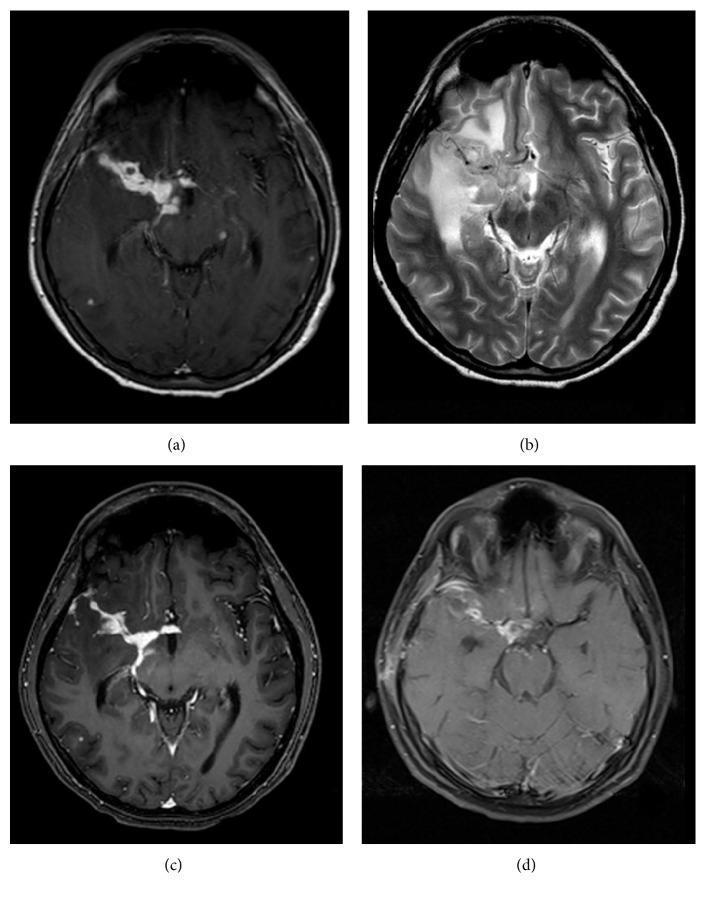
4. Autoimmune Encephalitis (LGI1) — T2 Shine-Through, No True Restricted Diffusion
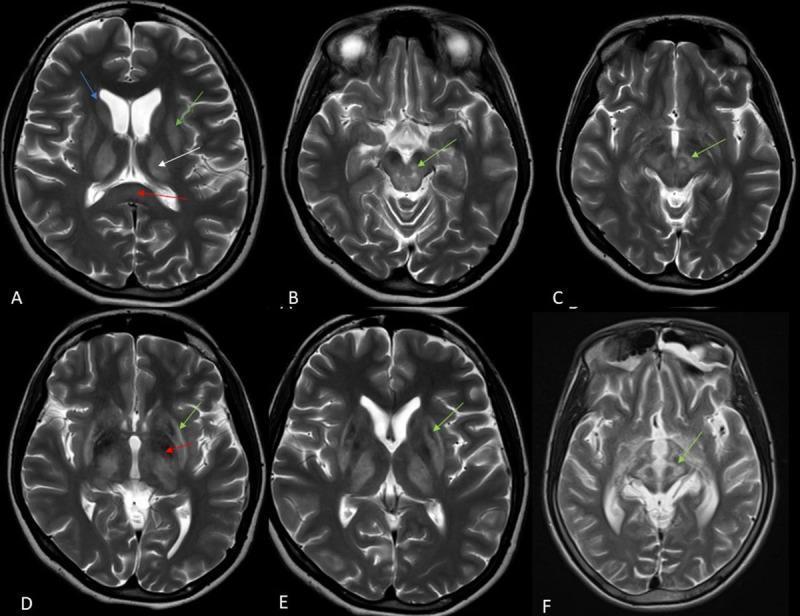
5. Wilson Disease — Bilateral Basal Ganglia T2 Signal Changes
Differential Diagnosis of Basal Ganglia Lesions on MRI
A. Bilateral Symmetric T2 Hyperintensity (Non-Enhancing)
| Diagnosis | Key Features | Clue |
|---|---|---|
| Wilson disease | Caudate, putamen, thalamus, midbrain; T1 hypo/hyper; "face of giant panda" | Young adult; liver disease; KF rings; ↓ceruloplasmin |
| Carbon monoxide poisoning | Globus pallidus (bilateral symmetric T2/DWI) | Exposure history; cherry-red skin |
| Cyanide / methanol poisoning | Putamen necrosis bilaterally | Toxic exposure |
| Leigh syndrome | Caudate, putamen, brainstem; T2 bright | Mitochondrial disorder; children; ↑lactate |
| Methylmalonic / propionic acidemia | Basal ganglia bilateral T2 hyperintensity | Metabolic crisis; organic acids in urine |
| Hypoxic-ischaemic encephalopathy | Putamen, thalamus; globus pallidus; DWI bright | Cardiac arrest, near-drowning; raised lactate |
| Hepatic encephalopathy | Globus pallidus T1 hyperintensity (manganese deposition) | Cirrhosis; ↑ammonia |
| Kernicterus (neonatal) | Globus pallidus T1 bright | Neonatal hyperbilirubinaemia |
| Osmotic demyelination (CPM) | Pontine + extrapontine (BG); T2 bright | Rapid Na correction |
| CJD | Caudate, putamen; DWI bright with ADC dark — TRUE restricted diffusion; "ribboning" cortex | Rapid dementia; 14-3-3 in CSF |
| NBIA (Neurodegeneration with Brain Iron Accumulation) | Globus pallidus "eye of the tiger" sign — central T2 bright, surrounded by hypointense rim | Pantothenate kinase deficiency; young |
B. Unilateral / Focal T2 Hyperintensity ± Enhancement
| Diagnosis | Signal | Enhancement | Clue |
|---|---|---|---|
| Basal ganglia infarct (lenticulostriate artery) | T2 bright; DWI bright + ADC dark | No enhancement (acute) | Vascular risk factors; sudden onset hemiplegia |
| Hypertensive putaminal hemorrhage | T2 hypointense (haemosiderin); heterogeneous | Ring or no enhancement | Hypertension; sudden onset |
| Brain abscess | T2 bright cavity; DWI bright core | Thick uniform ring | Fever; source of infection |
| Toxoplasmosis | T2 bright; necrotic core | Ring-enhancing often in BG; multiple | HIV CD4 <100; multiple lesions |
| Primary CNS lymphoma | Iso-to-hypointense on T2; homogeneous | Solid / homogeneous enhancement in HIV | HIV; periventricular; EBV |
| Metastasis | T2 bright; vasogenic edema | Ring or solid enhancement | Known primary cancer |
| Tuberculoma | T2 hypointense (central) | Ring or target enhancement | TB exposure; meningeal enhancement too |
| Neurocysticercosis | Cyst with scolex; T2 bright | Ring enhancement around cyst; calcification (old) | Endemic region; seizures |
C. Non-Enhancing Punctate T2/FLAIR Bright Lesions in Basal Ganglia
| Diagnosis | Feature |
|---|---|
| Cryptococcal pseudocysts | Bilateral; follow CSF signal; NO enhancement; dilated perivascular spaces |
| Dilated perivascular spaces (normal variant) | Tiny, symmetrical; follow CSF on all sequences; no DWI restriction |
| Lacunar infarcts | Small; FLAIR bright rim; old = hypointense center; vascular risk factors |
| MS plaques | Less common in BG; other typical demyelinating lesions elsewhere |
D. Autoimmune / Inflammatory
| Diagnosis | Key Feature |
|---|---|
| LGI1 autoimmune encephalitis | Unilateral/bilateral BG T2 bright; faciobrachial dystonic seizures; no true DWI restriction (T2 shine-through) |
| NMDAR encephalitis | BG/limbic involvement; cortical FLAIR changes; psychiatric onset |
| Rasmussen encephalitis | Unilateral progressive atrophy + signal; children |
| Susac syndrome | Corpus callosum "snowballs" + BG lesions + sensorineural deafness |
| ADEM | Bilateral BG T2 lesions; post-infectious; demyelinating pattern |
| Behçet disease | Brainstem + BG involvement; parenchymal neuro-Behçet |
Key Discriminating Points
| Pattern | Top Diagnoses |
|---|---|
| Bilateral BG T2 bright + metabolic context | Wilson, CO, Leigh, HIE, hepatic encephalopathy |
| Bilateral BG DWI bright + ADC dark | CJD, HIE |
| Bilateral BG T2 bright + T2 shine-through (ADC normal) | Autoimmune encephalitis (LGI1) |
| Globus pallidus T1 bright | Hepatic encephalopathy (Mn), CO (subacute), NF1 |
| Globus pallidus "eye of the tiger" | PKAN (NBIA) |
| Punctate BG + follow CSF + no enhancement | Cryptococcal pseudocysts |
| Ring-enhancing BG in HIV | Toxoplasmosis (multiple) vs. PCNSL (single, solid) |
| Basal ganglia + meningeal enhancement + hydrocephalus | Cryptococcal, TB, bacterial meningitis |
Mri of basal exudates with image and Differential
MRI basal cistern exudates meningitis T1 enhancement tuberculosis
basal meningitis MRI cryptococcal fungal leptomeningeal enhancement cistern
sarcoidosis neurosarcoidosis leptomeningeal enhancement MRI basal cistern
leptomeningeal carcinomatosis MRI enhancement basal cistern sulci
MRI Basal Cistern Exudates — Images & Differential Diagnosis
Normal vs. Abnormal Basal Cisterns
| Normal | Abnormal (Exudate) | |
|---|---|---|
| T1 + contrast | No enhancement; CSF dark | Bright enhancement filling cisterns |
| FLAIR | CSF completely suppressed (black) | Hyperintense — CSF suppression fails |
| Cistern morphology | Patent, open | Obliterated, filled with material |
Image Gallery
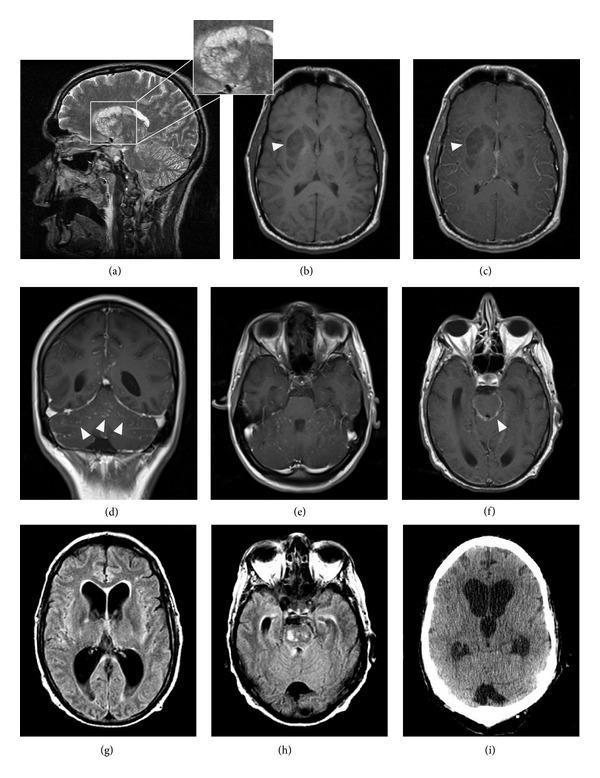
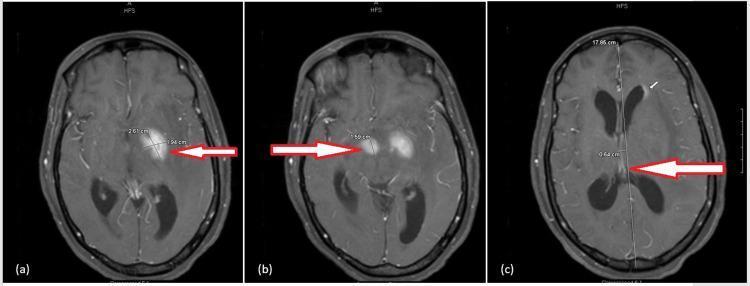
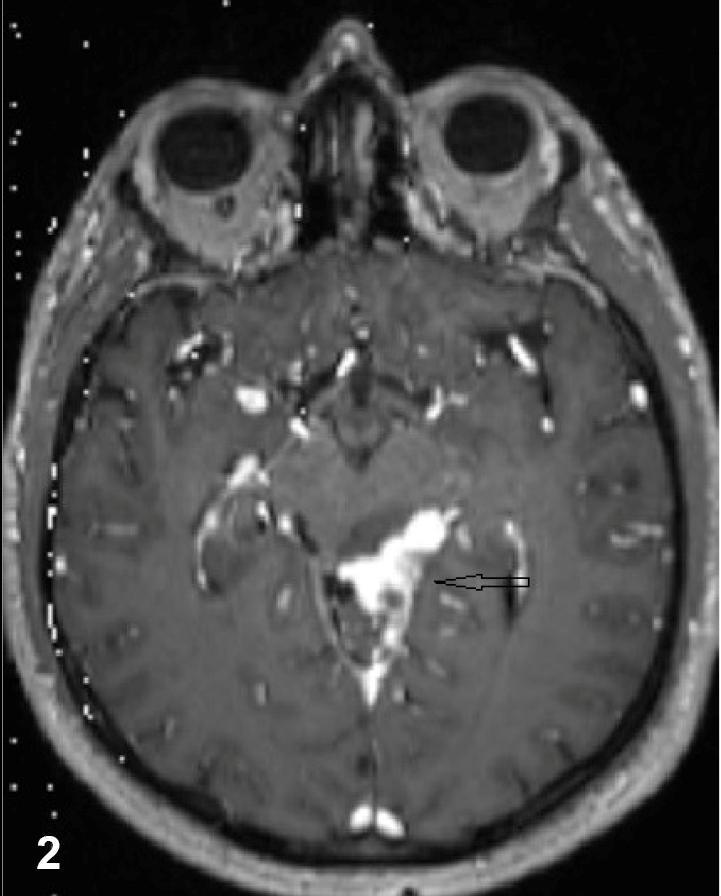
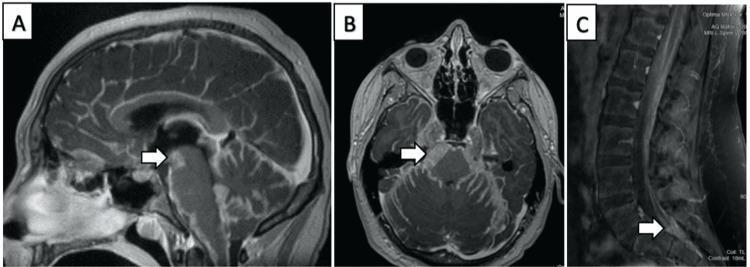
1. Tuberculous Meningitis — Thick Basal Cistern Enhancement (Classic)
2. TBM — Axial T1+Gad — Interpeduncular Cistern Obliteration
3. TB Meningitis — Radiological Triad (Hydrocephalus + Basal Enhancement + Pachymeningitis)

4. TBM — Active Basal Exudates Then Steroid Response (Sequential)
5. Neurosarcoidosis — Nodular Leptomeningeal Enhancement at Basal Cisterns
6. FLAIR Hyperintensity in Basal Cisterns (Non-specific but Sensitive)
7. Leptomeningeal Carcinomatosis — "Sugar-Coating" (Zuckerguss) Appearance
Differential Diagnosis of Basal Cistern Exudates/Enhancement
1. Infectious Causes (Most Common)
| Cause | Pattern of Enhancement | Key Clinical Features |
|---|---|---|
| Tuberculous meningitis ⭐ | Thick, nodular, basal predominant — interpeduncular, suprasellar, ambient cisterns + Sylvian fissures; tuberculomas; hydrocephalus; infarcts | Subacute onset; fever; meningism; cranial nerve palsies (II, III, VI, VII); lymphocytic CSF, low glucose, high protein; AFB stain/culture; ADA↑ |
| Bacterial meningitis | Diffuse leptomeningeal enhancement; may be basal or convexity | Acute onset; high fever; neck stiffness; neutrophilic CSF; Gram stain positive |
| Cryptococcal meningitis | Minimal or no enhancement often; dilated VR spaces in basal ganglia; leptomeningeal enhancement when present is subtle | HIV (CD4<100); headache; minimal meningism; India ink; CrAg >90% |
| Fungal meningitis (non-crypto) — Candida, Aspergillus, Coccidioides | Enhancement in basal cisterns; often nodular/exudative | Immunocompromised; transplant; antifungals |
| Neurocysticercosis (basal/cisternal type) | Cysts in basal cisterns; no scolex in extraparenchymal form; enhancement of cyst wall; racemose NCC = grape-like cluster in cisterns | Endemic; seizures; hydrocephalus from cyst obstructing cisterns |
| Pyogenic ventriculitis/ependymitis | Periventricular enhancement; extension to basal cisterns | Post-neurosurgery; shunt infection; neonates |
| Viral meningitis/encephalitis | Usually mild/no enhancement; or subtle basal | HSV, CMV, enteroviruses |
2. Granulomatous / Inflammatory (Non-Infectious)
| Cause | Pattern | Key Features |
|---|---|---|
| Neurosarcoidosis | Nodular, linear leptomeningeal enhancement; basal cisterns + cranial nerves + hypothalamus + pituitary stalk | Young adults; bilateral hilar adenopathy; ACE↑; non-caseating granuloma |
| Wegener's granulomatosis (GPA) | Pachymeningeal or leptomeningeal enhancement | Sinus + lung + kidney; p-ANCA |
| Behçet disease | Brainstem involvement; meningeal enhancement | Orogenital ulcers, uveitis |
| IgG4-related disease | Pachymeningeal (dural) thickening + enhancement | Hypophysitis; raised IgG4 |
| Vogt-Koyanagi-Harada | Leptomeningeal + uveal | Uveitis, vitiligo, poliosis, hearing loss |
3. Neoplastic
| Cause | Pattern | Key Features |
|---|---|---|
| Leptomeningeal carcinomatosis | Diffuse "sugar-coating" — sulci + cisterns + cranial nerves; drop metastases in spine | Known primary (breast, lung, GI, melanoma, lymphoma); multiple cranial neuropathies; positive CSF cytology |
| Primary CNS lymphoma | Periventricular + leptomeningeal; basal cisterns | Immunocompromised; EBV; homogeneous enhancement |
| Medulloblastoma / PNET | Posterior fossa + cisterns + drop mets spine | Children; CSF cytology |
| Gliomatosis / glioma with CSF spread | Leptomeningeal seeding | Aggressive high-grade glioma |
4. Vascular / Other
| Cause | Pattern | Key Features |
|---|---|---|
| Subarachnoid hemorrhage | FLAIR cistern hyperintensity (blood → CSF suppression fails); no post-Gad enhancement | Sudden severe headache; xanthochromia in CSF |
| Chemical meningitis | Post-LP, post-surgery, drug-induced | History |
| Superficial siderosis | T2 hypointense rim on brainstem surface (hemosiderin) | Chronic; hearing loss; cerebellar ataxia |
Key Discriminating Features
| Pattern | Top Diagnosis |
|---|---|
| Thick nodular basal enhancement + hydrocephalus + cranial nerve palsies | Tuberculous meningitis |
| Basal cistern obliteration + infarcts (lenticulostriate territory) | TB meningitis (vasculitis) |
| Nodular deposits + brainstem + cranial nerve enhancement | Neurosarcoidosis |
| Racemose cysts in cisterns | Cisternal neurocysticercosis |
| FLAIR bright cisterns without post-Gad enhancement | Subarachnoid haemorrhage; early bacterial meningitis |
| Diffuse "sugar-coating" of sulci + cisterns + spinal drop mets | Leptomeningeal carcinomatosis |
| Minimal enhancement but VR space dilation in BG | Cryptococcal meningitis |
| Thick dural/pachymeningeal > leptomeningeal | IgG4, meningioma en plaque, sarcoid |
Pathology of TBM Basal Exudates (Adams & Victor)
"A thick, gelatinous exudate accumulates at the base of the cerebral hemispheres, obliterating the pontine and interpeduncular cisterns and extending to the meninges around the medulla, the floor of the third ventricle, the optic chiasm, and the undersurfaces of the temporal lobes... Cranial nerves are often involved far more often than with typical bacterial meningitis. Arteries may become inflamed and occluded, with infarction of brain."
- Dense basal cistern enhancement
- Communicating hydrocephalus (cistern blockage)
- Cerebral infarcts (endarteritis of perforators)
Rapidly progressive dementia with 1 Yr and myoclonus 4 month Differential