Ankle joint examination
Reading File
Finding Sources
Searching the Web
ankle joint clinical examination orthopaedics inspection palpation movements tests
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete ankle joint examination guide.
Ankle Joint Examination
Sources: S Das Manual of Clinical Surgery 13th Ed, Bailey & Love's Short Practice of Surgery 28th Ed, Tintinalli's Emergency Medicine, Miller's Review of Orthopaedics 9th Ed, Campbell's Operative Orthopaedics 15th Ed 2026
Anatomy Recap
The ankle joint (talocrural joint) is a hinge joint formed by the tibia, fibula, and talus. The foot is divided into three regions:
- Hindfoot: talus and calcaneus
- Midfoot: navicular, cuboid, cuneiforms
- Forefoot: metatarsals and phalanges
The lateral malleolus is less prominent, descends ~1 cm lower and lies slightly posterior to the medial malleolus. - S Das Manual on Clinical Surgery, p. 261
1. HISTORY
Key points to elicit:
- Mechanism of injury: foot commonly anchored while the body drives forward - eversion, external rotation, or internal rotation injuries
- Three injury types: (i) external rotation, (ii) internal rotation, (iii) vertical compression
- In arthritis: gradual onset pain, swelling, stiffness - S Das Manual on Clinical Surgery, p. 214
2. GAIT
Observe the patient walking before formal examination:
- Antalgic gait: painful ankle/foot joint
- High-stepping gait: foot drop (common peroneal nerve injury)
- Short propulsive phase: suggests forefoot pain
- Examine footwear for abnormal wear patterns (normally posterolateral heel wear + ball of big toe) - Bailey & Love's Short Practice of Surgery 28th Ed, p. 518
3. INSPECTION (Look)
Standing Patient
From the front:
- Overall alignment, foot shape, and any deformity
- Assess pelvic obliquity, leg length discrepancy, valgus/varus at the knee
From the side:
- Medial longitudinal arch (normal vs. pes planus or pes cavus)
From behind:
- Heel alignment - normal heel valgus is 5-7°
- "Too many toes" sign = increased forefoot abduction (pes planus / splayed forefoot)
Attitude
- In arthritis of the ankle, the limb assumes a position of plantar flexion
Swelling
- Joint effusion: fullness on either side of the tendo Achilles + a bulge across the front of the joint
- Tendon sheath effusion: swelling extends along the long axis of the leg/foot far beyond joint level
- In fractures: look for deformity (lateral, medial, forward, or backward displacement); excessive broadening of the ankle suggests inferior tibiofibular diastasis (talus wedged between tibia and fibula)
Skin
- Ecchymosis, abrasions, blistering, skin color changes
- Bunion, gouty tophi, corns, nail changes
- Corns = callosities where toes rub shoes
Muscles
- Wasting obvious in tuberculous ankle arthritis
- Muscle wasting on the dorsum of the foot suggests neurological pathology - full neuro exam required
Foot Deformities
| Deformity | MTP Joint | PIP Joint | DIP Joint |
|---|---|---|---|
| Claw toe | Hyperextension | Flexion | Flexion |
| Hammer toe | Normal | Flexion | Flexion |
| Mallet toe | Normal | Normal | Flexion |
| Hallux valgus/varus | Valgus/Varus | Normal | - |
- Bailey & Love's Short Practice of Surgery 28th Ed
4. PALPATION (Feel)
Skin
- Temperature: increased local warmth in arthritis/infection
- Sensation: test light touch on dorsum (first web space) and lateral foot; inability to sense a Semmes-Weinstein 5.07 monofilament (10g) = neuropathy
- Glove-and-stocking reduced sensation suggests diabetes
Vascular
- Palpate posterior tibial pulse (behind medial malleolus)
- Palpate dorsalis pedis pulse (dorsum of foot, first web space)

Soft Tissues
- Tendo Achilles: palpate for gaps, tenderness, swelling along its full length; palpate attachment to os calcis
- Peroneal tendons: lateral side (peroneus brevis is dorsal to longus at the peroneal tubercle)
- Tibialis posterior tendon: medial side
- Tibialis anterior tendon and long extensors: dorsum of foot
- Sinus tarsi: soft-tissue depression anterior to the lateral malleolus - tenderness here with subjective hindfoot instability = sinus tarsi syndrome
- Retrocalcaneal bursa and Haglund's posterolateral prominence of the calcaneus
Bones - Palpation Landmarks
- Medial malleolus and lateral malleolus - palpate for bony tenderness, irregularity, crepitus
- Dome of talus: palpate with deep pressure anteriorly just below the ankle
- Calcaneum: posterior aspect; commonest cause of plantar heel pain = plantar fasciitis (most tender at plantar calcaneal origin)
- Sustentaculum tali: one fingerbreadth below the medial malleolus - attachment for spring ligament
- Syndesmosis (anterior ankle): tenderness suggests tibiofibular ligament injury
- Palpate all tarsal bones, metatarsals, and phalanges along their lengths
Fluctuation Test for Effusion
- With joint effusion, squeezing the swelling on either side of the tendo Achilles transmits a fluid impulse palpable in front of the joint - S Das Manual on Clinical Surgery
5. MOVEMENTS (Move)
The ankle is a hinge joint - primary movements are in one plane only.
Normal Ranges
| Joint | Movement | Normal Range |
|---|---|---|
| Ankle (talocrural) | Dorsiflexion | 25° |
| Ankle (talocrural) | Plantarflexion | 35° |
| Subtalar | Inversion | ~20° |
| Subtalar | Eversion | ~20° |
| Midtarsal | Abduction | 10° |
| Midtarsal | Adduction | 20° |
| MTP (hallux) | Extension | 70-90° |
| MTP (hallux) | Flexion | 45° |
Normal toe-off requires 35-40° of MTP dorsiflexion. - Bailey & Love's
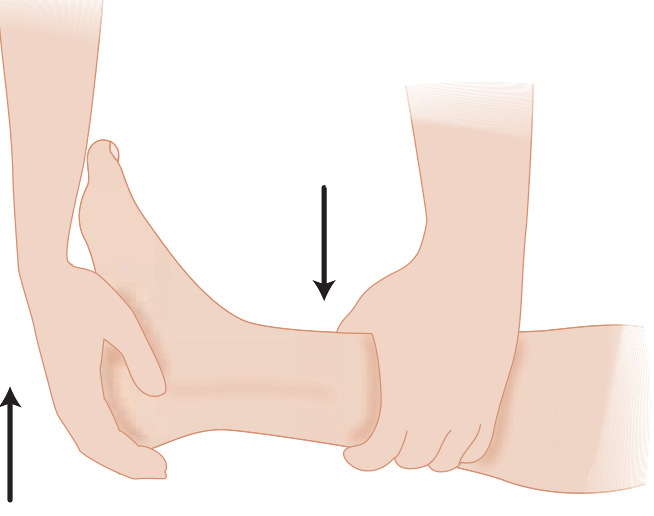
Testing Ankle (Talocrural) Movement
To test passive ankle movements: hold the leg with one hand and grasp the foot with the other hand including the head of the talus in the grip. This excludes movement at the subtalar and midtarsal joints, preventing a false impression of ankle motion in cases of ankle ankylosis.
- Dorsiflexion: test with knee both flexed and extended
- Restriction greater with knee extended → contracture primarily in gastrocnemius
- Restriction equal in both positions → contracture primarily in soleus
- Plantarflexion: weakness suggests Achilles tendon injury or S1 nerve root pathology
Subtalar Joint
Hold the talar neck (not the tibia - this isolates subtalar from ankle motion). Ask patient to move the heel side to side, or apply passive varus/valgus stress.
- Inversion: foot moves inwards
- Eversion: foot moves outwards
- Normal: ~5° in each direction
Midtarsal Joint
Hold the heel; move the forefoot medially (adduction = 20°) and laterally (abduction = 10°).
6. SPECIAL TESTS
A. Thompson Test (Simmonds Squeeze Test) - Achilles Tendon Integrity
Indication: Suspected Achilles tendon rupture
Technique: Lie the patient prone with the foot free over the edge of the couch. Squeeze the calf belly and observe the ankle.
Positive test: Absence of plantar flexion = Achilles tendon rupture
Important: Do not be misled if the patient can stand on tiptoes - this can be achieved by long toe flexors even with a complete rupture.
Diagnosis of Achilles rupture requires 2 or more of:
- Positive Thompson test
- Decreased ankle plantarflexion strength
- Palpable gap in the tendon
- Increased passive dorsiflexion with gentle manipulation
- Campbell's Operative Orthopaedics 15th Ed 2026
B. Anterior Drawer Test - ATFL (Anterior Talofibular Ligament)
Indication: Lateral ankle instability, suspected ATFL tear
Technique: Patient seated with the ankle in 10-15° of plantar flexion (places ATFL under tension). Cup the heel in one hand; apply counter-traction to the tibia with the other hand while drawing the heel forward.
Positive test: Increased anterior subluxation of ≥2 mm compared to the uninjured side, or visible dimpling of the anterior skin = significant ATFL injury (Grade III sprain)
- Tintinalli's Emergency Medicine; Bailey & Love's
C. Talar Tilt Test (Inversion Stress Test) - CFL (Calcaneofibular Ligament)
Indication: CFL instability
Technique: Invert the ankle in dorsiflexion to stress the CFL. Inversion in plantar flexion may also assess the ATFL.
Positive test: Excessive and asymmetric talar tilt = CFL rupture/instability
D. Squeeze Test - Syndesmosis Injury
Technique: Squeeze the tibia and fibula together above the ankle joint (midcalf level)
Positive test: Pain at the ankle/syndesmosis = interosseous membrane or syndesmosis injury
Also: Springing the fibula - squeeze the upper ends of tibia and fibula; pain at the lower fibula suggests a fibular fracture (Maisonneuve pattern). - S Das Manual on Clinical Surgery
E. Crossed-Leg Test - Syndesmosis
Technique: Patient crosses the affected leg over the contralateral knee (fibula resting on the other knee); pressure is applied medially at the knee level.
Positive test: Pain in the syndesmosis = syndesmosis injury
F. Coleman Block Test - Subtalar Joint Flexibility (Pes Cavus)
Technique: Patient stands on a 2 cm block, great toe resting on the floor over the medial edge. Observe the hindfoot from behind.
- Hindfoot varus corrects to valgus = subtalar joint is mobile (forefoot-driven deformity)
- Hindfoot varus remains = subtalar joint is fixed
G. Windlass / Jack's Test - Flat Foot Flexibility
Technique: Ask patient to stand on tiptoes and observe the medial arch.
- Arch forms as patient rises on tiptoes = flexible flat foot
- Arch fails to form = fixed flat foot

7. NEUROLOGICAL EXAMINATION
- Test sensation in the first web space (deep peroneal nerve) and lateral border of the foot (sural nerve)
- Deep peroneal nerve can be compressed at the anterior tarsal tunnel (anterior ankle / inferior extensor retinaculum)
- Superficial peroneal, tibial, and sural nerves should be assessed in appropriate clinical context
- Full upper and lower limb neurological exam if muscle wasting is present
8. MEASUREMENTS
When comparing to the contralateral side:
- Distance from medial malleolus to head of 1st metatarsal and to heel
- Distance from lateral malleolus to head of 5th metatarsal and to heel
- In calcaneal fractures: these measurements are altered compared to the sound side
Summary - Ankle Examination Checklist
| Step | Key Points |
|---|---|
| Gait | Antalgic, foot drop, propulsive phase |
| Inspect | Deformity, swelling, skin, alignment (front/side/behind) |
| Palpate | Temperature, pulses, malleoli, tendons, ligaments, effusion |
| Move | Dorsiflexion (25°), plantarflexion (35°), subtalar, midtarsal |
| Special Tests | Thompson, Anterior Drawer, Talar Tilt, Squeeze, Coleman Block |
| Neuro | Sensation, power, reflexes |
| Measure | Malleolus-to-metatarsal distances vs contralateral side |
This is a shared conversation. Sign in to Orris to start your own chat.