classify immunity, describe briefly T cell immunityand B-cell T cell coactivation,add a note on AIDS
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed for a thorough, well-illustrated answer. Here it is:
Classification of Immunity
Immunity is broadly divided into two arms that work sequentially:
1. Innate Immunity (Natural / Native Immunity)
- Present before any infection occurs; provides defense within hours of exposure
- Does not adapt or improve with re-exposure (limited memory)
- Recognizes broad molecular patterns shared by groups of microbes (PAMPs) via germline-encoded receptors
- Components:
- Physical/chemical barriers: skin, mucosal epithelia, antimicrobial peptides
- Cellular: phagocytes (macrophages, neutrophils), dendritic cells, NK cells, mast cells, innate lymphoid cells (ILCs)
- Soluble: complement, lectins, acute-phase proteins
- Key features: low specificity, low diversity, rapid response
2. Adaptive Immunity (Specific / Acquired Immunity)
- Develops over days in response to infection; increases in magnitude and quality with each successive exposure
- Recognizes a vast array of antigens through somatically recombined receptors
- Has immunological memory
- Subdivided into:
| Sub-type | Mediator | Main function |
|---|---|---|
| Humoral immunity | B lymphocytes → plasma cells → antibodies | Neutralization, opsonization, complement activation; effective against extracellular pathogens |
| Cell-mediated immunity | T lymphocytes (CD4+ helper, CD8+ cytotoxic) | Kill infected/tumor cells; coordinate immune response; effective against intracellular pathogens |
- Key features: high specificity, high diversity (somatic recombination), memory, self-tolerance
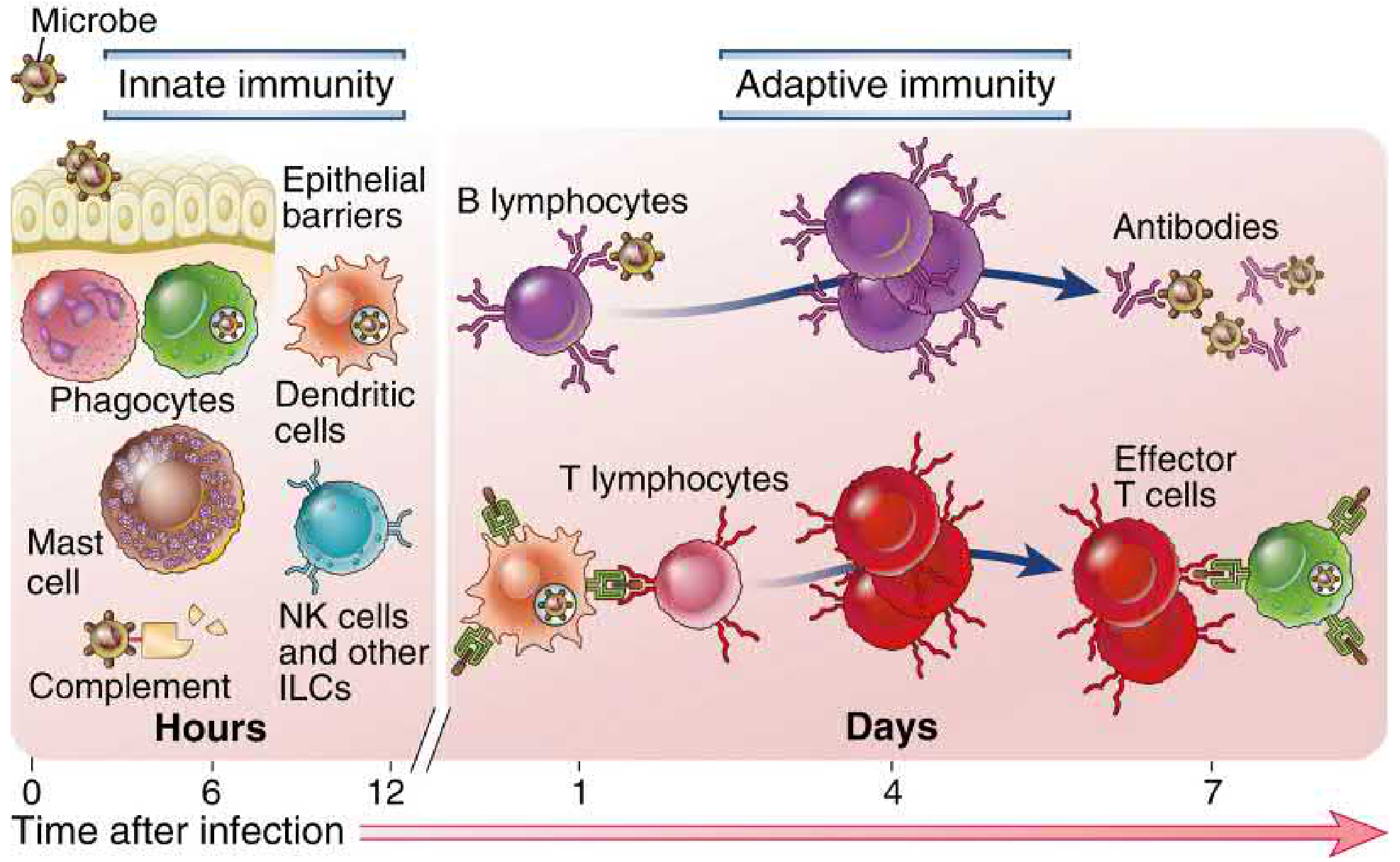
Innate and adaptive immunity. The innate response acts within hours; the adaptive response (B and T lymphocytes) develops over days. - Cellular and Molecular Immunology, Fig. 1.1
T-Cell Immunity
T cells mature in the thymus and circulate through blood and lymphoid tissue. They respond to antigens only when these are presented as peptide fragments bound to MHC proteins on antigen-presenting cells (APCs) - macrophages, B cells, and dendritic cells (the most potent APCs).
Antigen Presentation & T-Cell Activation
- MHC class I proteins present antigens to cytotoxic (CD8+) T cells
- MHC class II proteins present antigens to helper (CD4+) T cells and regulatory T cells
- T-cell receptors (TCRs) on the T-cell surface bind the peptide-MHC complex; each T cell has up to 100,000 receptor sites
- Cell adhesion proteins are required to hold the T cell to the APC long enough for activation to occur
Types of T Cells
There are three major functional groups:
1. T-Helper Cells (CD4+) - >75% of all T cells
The master regulators of the immune system. Once activated by antigen presented on MHC-II, naïve CD4+ T cells differentiate into subsets secreting lymphokines (cytokines) that orchestrate all other immune functions.
| Subset | Induced by | Cytokines produced | Main effect |
|---|---|---|---|
| T | IFN-γ, IL-12 | IFN-γ, IL-2, TNF-α, GM-CSF | Macrophage activation, IgG production |
| T | IL-4 | IL-4, IL-5, IL-6, IL-10, IL-13 | IgE production, mast cell/eosinophil activation |
| T | TGF-β, IL-1, IL-6, IL-23 | IL-17, IL-22 | Neutrophil/monocyte recruitment |
| T | Multiple | IL-21 | B-cell help in germinal centers |
2. Cytotoxic T Cells (CD8+)
- Recognize antigen on MHC class I (expressed on all nucleated cells)
- Directly kill virus-infected cells, tumor cells, and transplanted foreign cells
- Kill via perforins and granzymes or Fas-FasL interaction
3. Regulatory T Cells (Tregs / Suppressor T Cells)
- Suppress excessive immune activation
- Maintain self-tolerance; prevent autoimmunity
T-Cell Effector Release and Memory
After activation, large numbers of antigen-specific T cells are released from lymphoid tissue into the circulation, recirculating through blood and tissues for months to years. Memory T cells are also generated; on second exposure to the same antigen, the response is dramatically faster and stronger.
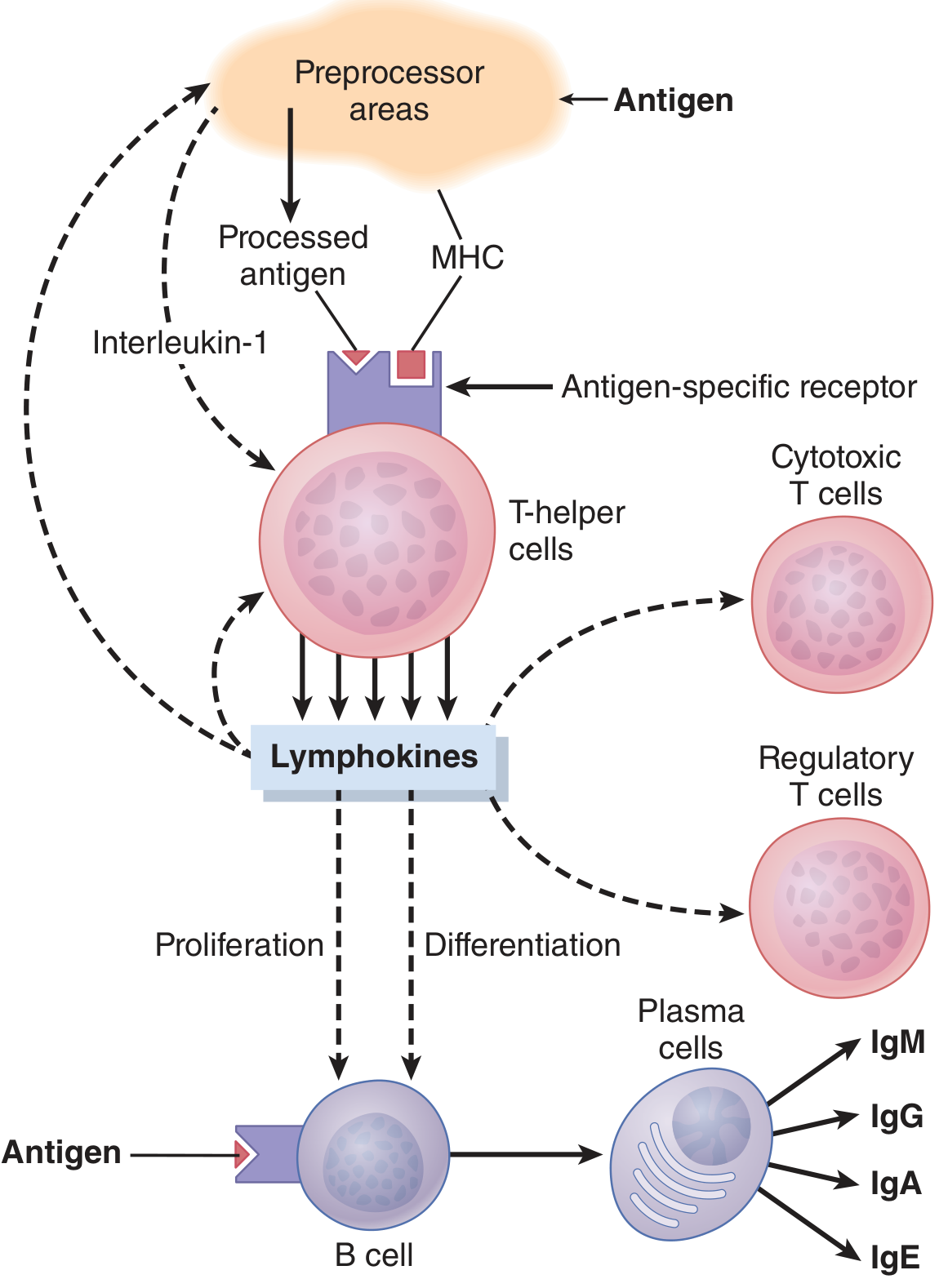
T-helper cells are the central regulators of immunity, directing B cells, cytotoxic T cells, and regulatory T cells via lymphokines. - Guyton and Hall, Fig. 35.8
B-Cell and T-Cell Coactivation
Most antibody responses to protein antigens require cooperation between B cells and T-helper cells. This interaction is called thymus-dependent (TD) antigen response.
Step-by-Step Mechanism
-
BCR signal (Signal 1): The B-cell antigen receptor (BCR/surface Ig) binds antigen. This initiates intracellular signaling and also internalizes the antigen. The antigen is processed and its peptide fragments are returned to the cell surface bound to MHC class II molecules.
-
T-cell recognition: An antigen-specific CD4+ T
FH(follicular helper T) cell that has already been activated by the same pathogen recognizes the peptide-MHC II complex on the B-cell surface. -
Co-stimulatory signal (Signal 2 - CD40-CD40L interaction): The T cell expresses CD40 ligand (CD40L / CD154) which binds CD40 on the B cell. This activates:
- The canonical NF-κB signaling pathway (via IKK)
- The non-canonical NF-κB pathway (via NIK/NF-κB-inducing kinase)
- Expression of anti-apoptotic proteins (e.g., Mcl-1), promoting B-cell survival
-
Cytokine signals: The T cell secretes IL-21 (activates STAT3, enhancing B-cell proliferation and plasma cell differentiation), plus IL-4, IL-6, IL-2, TGF-β, and IFN-γ - these regulate isotype switching (IgM → IgG, IgA, IgE).
-
Outcome: Activated B cells proliferate, enter germinal centers, undergo somatic hypermutation (affinity maturation), and differentiate into:
- Plasma cells - long-lived antibody-secreting factories
- Memory B cells - rapid responders upon re-exposure
Thymus-Independent (TI) Antigens
Some microbial antigens (highly repetitive structures like bacterial polysaccharides, LPS) can activate B cells without T-cell help by cross-linking BCRs and signaling through TLRs. These responses produce mainly IgM and lack affinity maturation; they provide early but lower-quality protection.
Sources: Janeway's Immunobiology 10e, Figs. 10.2, 10.3; Guyton and Hall, Chapter 35
Note on AIDS (Acquired Immunodeficiency Syndrome)
AIDS directly exploits the T-helper cell axis described above, which is why it produces such profound immunosuppression.
The Virus
HIV (Human Immunodeficiency Virus) is an RNA retrovirus containing the enzyme reverse transcriptase. The incubation period before clinical AIDS develops can be up to 11 years.
Mechanism of CD4+ T-Cell Infection
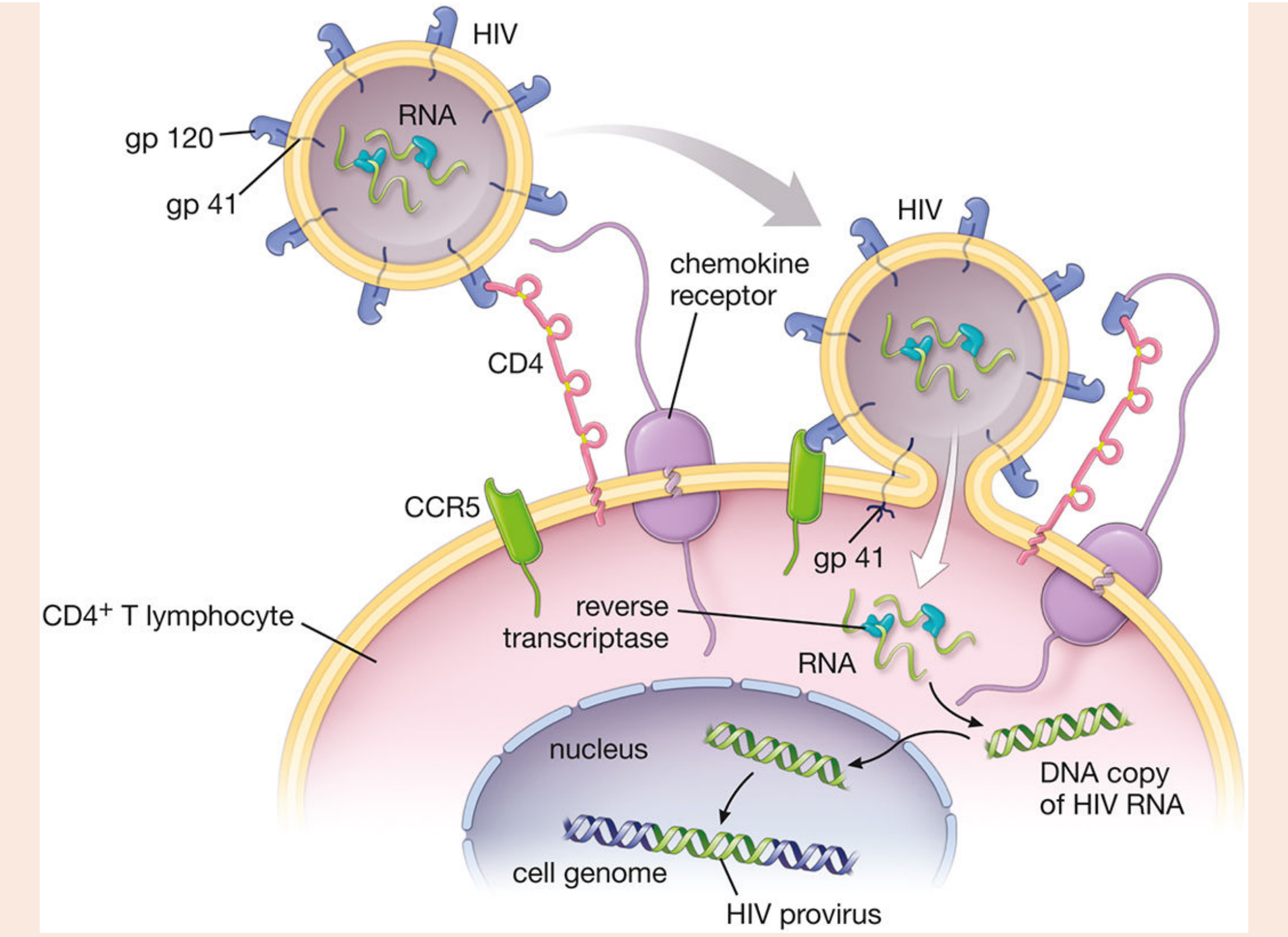
HIV gp120 binds CD4 and CCR5 co-receptor on helper T cells; gp41 mediates membrane fusion; viral RNA is reverse-transcribed into proviral DNA that integrates into the host genome. - Histology: A Text and Atlas, Fig. F14.3.1
- Entry: HIV envelope glycoprotein gp120 binds CD4 molecules on helper T cells, forming a CD4-gp120 complex. This exposes gp41, which anchors the virus into the T-cell membrane. CCR5 (C-C chemokine receptor type 5) acts as a major co-receptor for gp120 binding.
- Fusion & injection: The viral envelope fuses with the T-cell membrane, injecting viral RNA + reverse transcriptase into the cytoplasm.
- Reverse transcription: Viral RNA is reverse-transcribed into double-stranded proviral DNA.
- Integration: Viral integrase incorporates proviral DNA into the host genome permanently.
- Replication: New viral particles are produced and bud off to infect more helper T cells.
Immune Consequences
- The immune system initially responds by generating CD8+ cytotoxic T cells and antibodies against HIV
- But CD8+ T cells kill the HIV-infected CD4+ T cells, progressively reducing their numbers
- The CD4+ T-cell count is used clinically as a marker of disease progression (AIDS defined as CD4 <200 cells/μL)
- As CD4+ T cells are depleted, the entire immune system collapses - B cells lose T-cell help, cytotoxic T cells lose T-helper support, macrophage activation fails
- Patients die of opportunistic infections (PCP, CMV, Toxoplasma, cryptococcal meningitis, MAC) and AIDS-defining cancers (Kaposi sarcoma, NHL)
Treatment
- Antiretroviral therapy (ART): Combination of multiple drug classes to suppress viral replication:
- NRTIs (nucleoside reverse transcriptase inhibitors, e.g., AZT/zidovudine - the first drug used)
- NNRTIs (non-nucleoside reverse transcriptase inhibitors)
- Protease inhibitors (block viral protease)
- Integrase strand transfer inhibitors (prevent proviral DNA integration)
- ART advantages over monotherapy: synergistic effects, reduced side effects, and reduced drug resistance
- ART does not cure HIV but can suppress viral load to undetectable levels, allowing near-normal CD4 counts and life expectancy
Sources: Histology A Text and Atlas (Histology), Guyton and Hall Textbook of Medical Physiology, Cellular and Molecular Immunology, Janeway's Immunobiology 10e
This is a shared conversation. Sign in to Orris to start your own chat.