Blood & blood transfusion in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a detailed answer. Let me compile everything.
Blood & Blood Transfusion - Comprehensive Guide
1. COMPOSITION OF BLOOD
Blood is a specialized connective tissue comprising approximately 8% of body weight. It consists of:
- Plasma (~55%): water, proteins (albumin, globulins, fibrinogen, clotting factors), electrolytes, hormones, nutrients, waste products
- Formed elements (~45%):
- Red blood cells (RBCs/erythrocytes): oxygen transport via hemoglobin
- White blood cells (leukocytes): immunity and defense
- Platelets (thrombocytes): hemostasis
2. BLOOD GROUPS
ABO System
The ABO system is the most important blood group system for transfusion compatibility. It is governed by two main antigens (A and B) encoded by two alleles, plus an inactive O allele. Four phenotypes result:
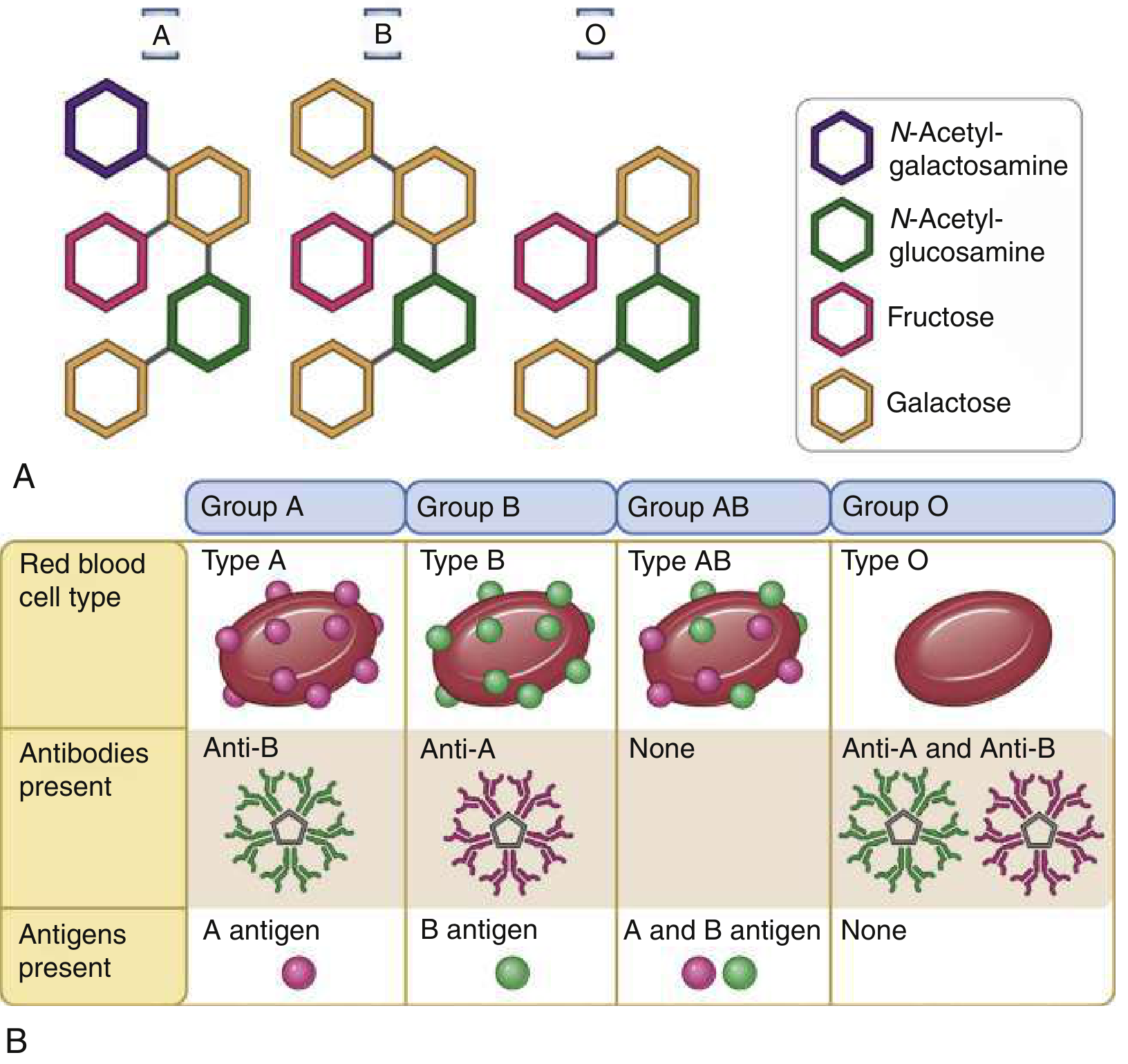
| Blood Group | RBC Antigen | Serum Antibody |
|---|---|---|
| A | A antigen | Anti-B |
| B | B antigen | Anti-A |
| AB | A and B antigens | None ("universal recipient") |
| O | None | Anti-A and Anti-B ("universal donor") |
ABO antigens are carbohydrate-based and are ubiquitously distributed on endothelial cells - making them genuine "tissue groups" relevant to organ transplantation as well. Natural (regular) ABO antibodies form without prior transfusion exposure, triggered by environmental bacteria sharing similar antigens. These IgM antibodies bind complement and can cause severe intravascular hemolysis, making ABO compatibility a strict requirement. - Harrison's Principles of Internal Medicine 22E, p. 1050-1052
Rh System
The Rh system is the most clinically significant protein-based blood group system. Unlike ABO, Rh antibodies require prior allogeneic stimulation (transfusion or pregnancy) to develop, since these antigens are human-specific.
- ~45 RBC blood group systems are recognized; ~390 antigens described
- Five systems routinely investigated due to clinical significance of their antibodies: Rh, Kell, Duffy, Kidd, and MNS - testing all five achieves ~95% routine transfusion compatibility
- Warm autoantibodies (IgG, active at 37°C): most often directed against Rh antigens - cause warm autoimmune hemolytic anemia
- Cold autoantibodies (IgM, active at 4°C): directed against ABO, HI, I, P antigens
Alloimmunization
Transfusion may result in the production of alloantibodies including:
- Anti-RBC antibodies (risk of hemolysis)
- Anti-HLA antibodies (platelet refractoriness, TRALI)
- Anti-HPA (human platelet antigen) antibodies
- Anti-HNA (human neutrophil antigen) antibodies
3. BLOOD COMPONENTS AND COLLECTION
Collection and Manufacturing
Whole blood is collected by phlebotomy (300-500 mL) into specialized bags containing anticoagulants and preservatives. Anticoagulant options include:
| Solution | Key Features |
|---|---|
| ACD (Acid Citrate Dextrose) | Citrate-based; older formulation |
| CPD (Citrate Phosphate Dextrose) | Standard; 35-day shelf life |
| CPDA-1 | Adds adenine; extends shelf life to 35 days |
| Additive solutions (AS-1, AS-3, AS-5) | Extend RBC shelf life to 42 days |
Citrate chelates calcium and prevents coagulation. Dextrose and adenine support RBC ATP production.
Blood Components
1. Packed Red Blood Cells (PRBCs)
- Hematocrit: 70-80%
- Shelf life: 35-42 days at 2-6°C
- 1 unit raises adult hemoglobin by ~1 g/dL or hematocrit by ~3%
- In children: 10 mL/kg raises Hb ~1 g/dL
- Transfusion time: 60-90 min per unit; must not exceed 4 hours (bacterial growth risk)
- Indication: Improve oxygen delivery to tissues
2. Fresh Frozen Plasma (FFP)
- Contains all coagulation factors (1 unit of activity per mL)
- Indications: Coagulopathy reversal, massive transfusion, liver disease
- Dosing: 10-30 mL/kg (variable clinical response)
- Note: PCC (prothrombin complex concentrate) preferred over FFP for vitamin K antagonist reversal in life-threatening hemorrhage
3. Platelets
- Stored at room temperature (22°C) with gentle agitation
- Shelf life: 5-7 days
- Transfusion triggers:
- Prophylactic: count <10,000/μL (stable adult)
- Central venous catheter placement: <20,000/μL
- Lumbar puncture / non-neuroaxial surgery: <50,000/μL
- Dose: 6 units (pooled "six-pack") or 1 apheresis unit → raises platelet count ~40,000-60,000/μL
- Apheresis platelets expose recipient to plasma proteins of only one donor (lower allergic reaction risk)
4. Cryoprecipitate
- Derived from plasma; rich in fibrinogen, Factor VIII, Factor XIII, vWF, fibronectin
- Indicated for significant hypofibrinogenemia (<100 mg/dL)
- Dose: ~10 bags raises fibrinogen by ~1 g/L (100 mg/dL)
5. Whole Blood
- Shelf life shorter than components but can be cost-effective
- Low-titer O whole blood (LTOWB) is safe and effective, especially in hemorrhagic resuscitation
- Advantages over component therapy: physiologic balance, higher hemostatic factors, more fibrinogen delivery, fewer donor exposures
- Risk: Rh isoimmunization in premenopausal women receiving LTOWB (consider Rh immunoglobulin)
6. Granulocyte Concentrates
- Used rarely in severe neutropenia with refractory infection; not leukoreduced
Leukoreduction (Leukocyte Reduction)
Most components are now prestorage leukocyte-reduced to <1-5 × 10^6 donor leukocytes. This reduces:
- Febrile non-hemolytic transfusion reactions (FNHTRs)
- CMV transmission risk
- Alloimmunization
- Immunomodulation
Additional Processing
| Processing Step | Indication |
|---|---|
| Irradiation | Prevent transfusion-associated GVHD in immunosuppressed patients |
| Pathogen reduction | Reduce risk of transfusion-transmitted infections |
| Washing | Severe allergic reactions to plasma proteins |
| CMV-negative units | Neonates, immunocompromised (if leukoreduced not available) |
Storage Lesion
Biochemical and structural changes during RBC storage include:
- Loss of RBC deformability
- Potassium leakage
- Irreversible membrane changes
- Impaired oxygen unloading in microcirculation
These worsen with storage duration. Clinical significance is debated - large randomized trials have found no statistically significant difference in outcomes based on blood age. - Rosen's Emergency Medicine, p. 2441
4. BLOOD TYPING AND COMPATIBILITY TESTING
Type and Screen:
- Blood type: identify ABO group and Rh factor
- Antibody screen: detect unexpected alloantibodies
Crossmatch:
- Confirms compatibility between donor RBCs and recipient serum
- Electronic crossmatch acceptable if no alloantibodies detected
Emergency Transfusion:
- Untyped blood: Group O Rh-negative PRBCs (universal donor for RBCs)
- Type-specific blood: Can be issued within minutes once type is known
5. TRANSFUSION INDICATIONS AND THRESHOLDS
Red Cell Transfusion (AABB 2016 Guidelines)
| Patient Category | Hemoglobin Threshold |
|---|---|
| Most stable hospitalized patients | < 7 g/dL |
| Orthopedic surgery, cardiac surgery, known cardiovascular disease | < 8 g/dL |
| Known/symptomatic coronary artery disease | < 9 g/dL |
| Acute exsanguinating hemorrhage | Immediate regardless of level |
The rationale: RBC transfusion is only indicated to increase oxygen delivery at the tissue level. Restrictive strategies are associated with lower mortality and rebleeding compared to liberal strategies in most patient populations. - Rosen's Emergency Medicine, p. 2530
6. MASSIVE TRANSFUSION PROTOCOL (MTP)
Definition: Traditionally >10 units PRBCs in 24 hours; practically: ≥3 units PRBCs/hour or ≥4 components in 30 minutes.
Rationale: Acute massive hemorrhage involves loss of all blood components, not just red cells. Replacement should mirror this.
Standard Ratio: 1:1:1 (PRBCs : FFP : Platelets) - most protocols now advocate this ratio.
MTP Flowchart (Denver Health Model):
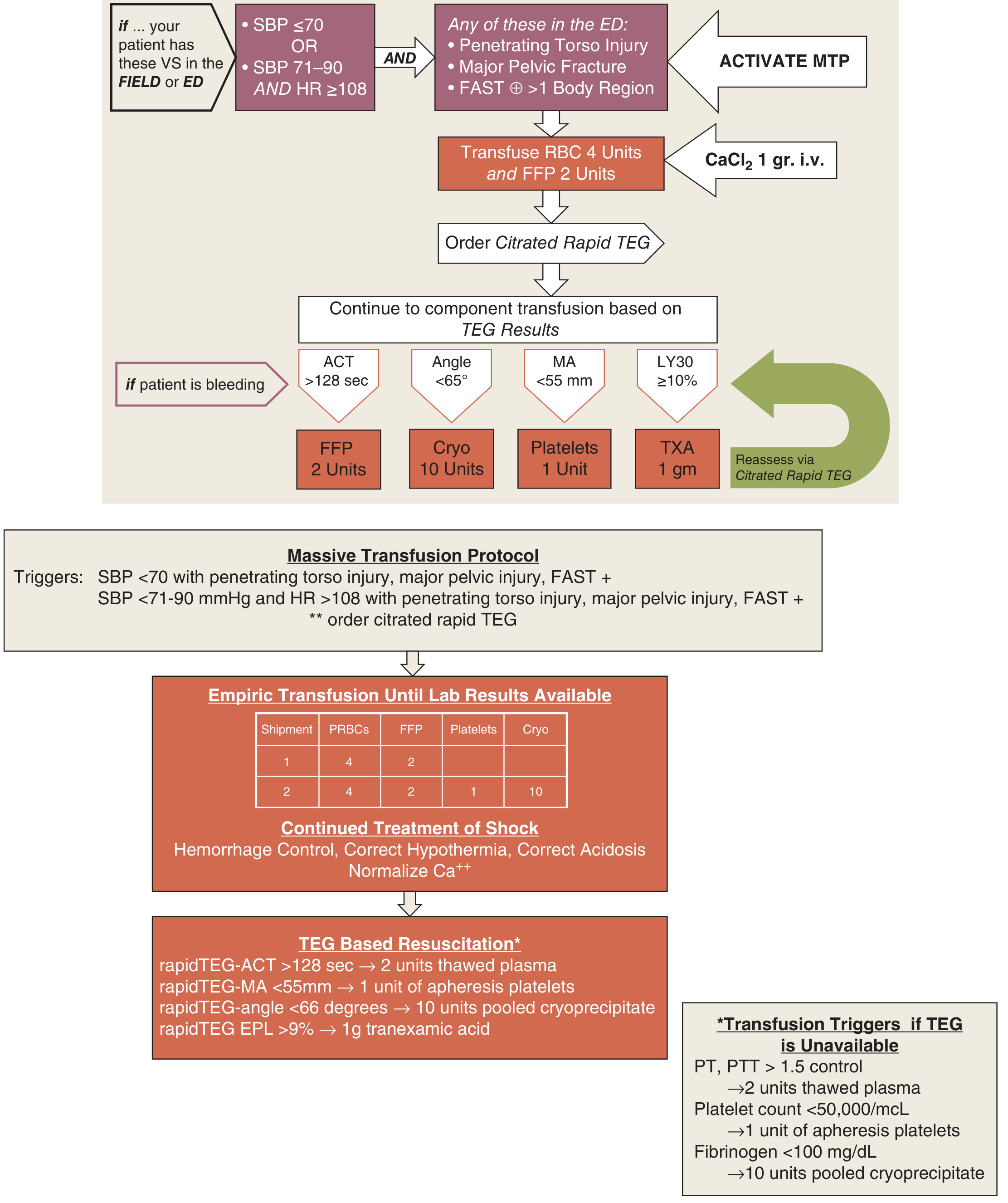
Complications of Massive Transfusion ("Lethal Triad")
| Complication | Mechanism | Management |
|---|---|---|
| Hypothermia | Infusion of cold blood, impaired metabolism | Blood warmers, warming blankets |
| Coagulopathy | Dilution, factor consumption, citrate | Replace FFP/platelets/cryo per ratio; TEG/ROTEM guided |
| Metabolic acidosis | Hypoperfusion, citrate load | Optimize O₂ delivery; NaHCO₃ not routinely recommended |
| Hypocalcemia | Citrate chelates Ca²⁺ | Calcium supplementation |
| Hyperkalemia | Potassium leaks from stored RBCs | Monitor electrolytes |
| Metabolic alkalosis | Citrate metabolized → bicarbonate | Monitor pH |
7. TRANSFUSION REACTIONS
Acute Reactions
1. Febrile Non-Hemolytic Transfusion Reaction (FNHTR)
- Most common reaction: ~1 in 100-200 transfusions
- Mechanism: Cytokines from donor leukocytes
- Presentation: Temperature rise ≥1°C (2°F), no hemolysis
- Treatment: Antipyretics; leukoreduced products reduce incidence
2. Allergic Reactions
- Second most common: ~1 in 300 transfusions
- Range: urticaria/pruritus → anaphylaxis
- Mechanism: IgE-mediated reaction to donor plasma proteins; IgA-deficient recipients may have anti-IgA antibodies
- IgA deficiency: affects 1 in 700, but severe reactions in minority
- Treatment:
- Mild (localized): antihistamines; transfusion may be restarted
- Severe/recurrent: steroids 2-3 hours pre-transfusion
- Anaphylaxis: epinephrine; give IgA-deficient units or washed units
3. Acute Hemolytic Transfusion Reaction (AHTR)
- Incidence: 1 in 6,000-30,000 transfusions; fatal: 1 in 100,000-600,000
- Mechanism: Usually ABO incompatibility (most from clerical error); complement activation → intravascular hemolysis
- Presentation: Abrupt fever, chills, back/flank pain, hypotension, DIC, hemoglobinuria, renal failure, sense of "impending doom," burning at infusion site
- Lab: Positive DAT, pink serum, hemoglobinuria, elevated bilirubin, schistocytes, coagulopathy
- Treatment: STOP transfusion immediately → IV fluids, monitor renal function, treat DIC
- Fatal reactions must be reported to the FDA within 7 days
4. TRALI (Transfusion-Related Acute Lung Injury)
- Leading cause of transfusion-related mortality
- Incidence: 1 in 5,000-190,000 transfusions
- Mechanism: Donor anti-HLA or anti-HNA antibodies react with recipient neutrophils → massive pulmonary neutrophil activation → non-cardiogenic pulmonary edema
- Presentation: Acute respiratory distress within 6 hours of transfusion; bilateral pulmonary infiltrates; NO evidence of fluid overload
- Treatment: Stop transfusion; supportive respiratory care (NIPPV or intubation/mechanical ventilation)
5. TACO (Transfusion-Associated Circulatory Overload)
- Presentation: Dyspnea, elevated BNP, hypertension, bilateral pulmonary infiltrates
- Distinguish from TRALI: TACO shows elevated filling pressures
Delayed Reactions
6. Delayed Hemolytic Transfusion Reaction (DHTR)
- Incidence: ~1 in 1,500 transfusions
- Timing: 5-14 days after transfusion (anamnestic antibody response)
- Most commonly implicated antigens: Kidd (most severe - intravascular hemolysis), E, c, Kell, Duffy
- Findings: Positive DAT (mixed field), hyperbilirubinemia, microspherocytes
- Treatment: Identify responsible antibody; avoid further exposure; usually no acute treatment needed
7. Transfusion-Associated GVHD (TA-GVHD)
- Donor T-lymphocytes attack immunocompromised recipient
- Prevention: Irradiation of cellular blood products in at-risk patients
Infectious Risks (Current Estimated Rates)
| Pathogen | Risk per Unit |
|---|---|
| HIV | 1 in 3 million |
| HCV | 1 in 1.5 million |
| HBV | 1 in 300,000 |
| HTLV-I/II | 1 in 2.9 million |
| Bacterial contamination (platelets) | 1 in 75,000-100,000 |
| Bacterial contamination (RBCs) | 1 in 500,000 |
All US blood donors are tested for: HIV-1/2, HTLV-I/II, HBV, HCV, syphilis, West Nile virus, Zika virus, and Trypanosoma cruzi. Endemic regions also test for Babesia microti.
Bacterial Septic Transfusion Reactions:
- Most common transfusion-transmitted infection; mortality 25% (platelets), 70% (RBCs)
- Platelet-related: Staphylococcal species (stored at room temperature)
- RBC-related: Psychrophilic Gram-negative bacilli - Yersinia enterocolitica (most common), Serratia, Citrobacter, Pseudomonas
- Treatment: Stop transfusion, Gram stain the unit, broad-spectrum antibiotics, hemodynamic support
8. SPECIAL TOPICS
Autologous Blood Transfusion
- Patient donates own blood before elective surgery
- Now used rarely due to little advantage over allogeneic (with modern blood safety)
- Still useful for patients with rare blood group phenotypes
Autotransfusion (Intraoperative Cell Salvage)
- Blood collected from uncontaminated bleeding sites (e.g., thoracic trauma) and returned to patient
- Advantages: immediate availability, perfect compatibility, no disease transmission risk, acceptable to Jehovah's Witnesses
Irradiation
- Prevents TA-GVHD in: immunocompromised patients, neonates, intrauterine transfusion recipients, HLA-matched/directed donations, post-stem cell transplant patients
TEG/ROTEM in Massive Transfusion
- Viscoelastic point-of-care tests guide goal-directed transfusion
- Alters transfusion patterns; preliminary data suggest TEG-guided therapy may reduce mortality vs. conventional coagulation parameters, but further study is needed
Sources
- Harrison's Principles of Internal Medicine 22E (2025) - Blood components, blood group antigens
- Rosen's Emergency Medicine - Blood products, transfusion thresholds, massive transfusion, transfusion reactions
- Quick Compendium of Clinical Pathology 5th ed. - Transfusion complications and risk table
- Tietz Textbook of Laboratory Medicine 7th ed. - Blood banking and collection
- Schwartz's Principles of Surgery 11th ed. - Massive transfusion protocol
Each colour tube reagent it contains
Reading File
Finding Sources
Finding Sources
Searching the Web
blood collection tube colors additives contents chart complete guide
Reading File
Reading File
Reading File
I now have a complete, authoritative table from Henry's Clinical Diagnosis & Management by Laboratory Methods + Quick Compendium of Clinical Pathology. Here is the full guide:
Blood Collection Tubes - Color, Additive, Mechanism & Use
Complete Reference Table
| Cap Color | Additive | Mechanism of Action | Specimen Type | Tests / Uses |
|---|---|---|---|---|
| Red (glass) | None | Blood clots naturally; serum separated by centrifugation | Serum | Chemistry, serology, immunology, blood bank |
| Red (plastic / Hemogard) | Clot activator (silica particles) | Silica accelerates clot formation | Serum | Chemistry, serology, drug levels |
| Gold / Red-Gray (SST) | Clot activator + separation gel | Gel forms a barrier between serum and cells after centrifugation | Serum | Chemistry, immunochemistry, therapeutic drug monitoring (TDM) |
| Yellow/Orange (rapid serum) | Thrombin (clot activator) | Very fast clot activation (~5 min) | Serum | Stat chemistry tests |
| Light Blue | Sodium citrate 3.2% (0.109 M) | Chelates calcium → prevents clotting; preserves labile coagulation factors | Plasma | PT/INR, aPTT, fibrinogen, D-dimer, coagulation screen - must be filled exactly to the line (1:9 anticoagulant:blood ratio) |
| Light Blue (special) | Thrombin + soybean trypsin inhibitor | Activates clotting + inhibits fibrinolysis | Plasma | Fibrin degradation products (FDP) |
| Black | Sodium citrate (1:4 ratio) | Chelates calcium | Plasma | ESR (erythrocyte sedimentation rate) - uses a higher citrate concentration than the light blue coag tube |
| Green | Sodium heparin or Lithium heparin | Inhibits thrombin and thromboplastin formation | Plasma | Plasma chemistry, stat chemistries, ammonia, blood gases |
| Light Green / Green-Black (PST) | Lithium heparin + separation gel | Heparin anticoagulates; gel separates plasma from cells | Plasma | Chemistry, immunochemistry |
| Lavender / Purple | K₂EDTA (spray-dried) or K₃EDTA (liquid) | Chelates calcium → prevents clotting | Whole blood | CBC, WBC differential, blood film/morphology, HbA1c, reticulocyte count |
| Pink | Spray-dried K₂EDTA | Chelates calcium | Whole blood | Blood bank: ABO grouping, Rh typing, antibody screen, crossmatch - FDA-approved for blood bank; has special AABB cross-match label |
| White | EDTA + gel | Chelates calcium; gel separates plasma | Plasma | Molecular diagnostics: PCR, bDNA amplification |
| Gray | Sodium fluoride + potassium oxalate OR sodium fluoride/Na₂EDTA | Fluoride inhibits enolase → blocks glycolysis; oxalate/EDTA anticoagulates | Plasma | Glucose, lactate, blood alcohol - preserves glucose up to 5 days |
| Royal Blue | Sodium heparin OR K₂EDTA (no trace elements in stopper) | Heparin or EDTA; special low-trace-element stopper formulation | Plasma or serum | Trace element testing (zinc, copper, lead, mercury), toxicology, nutritional chemistry |
| Tan (glass) | Sodium heparin | Inhibits thrombin formation | Plasma | Lead testing |
| Tan (plastic) | K₂EDTA | Chelates calcium | Plasma | Lead testing |
| Dark Blue / Navy | EDTA (no contaminating metals) | Chelates calcium; metal-free tube | Plasma | Trace metals, heavy metal screening |
| Yellow (SPS) | Sodium polyanetholsulfonate (SPS) | Inhibits complement, phagocytosis, and some antibiotics → aids bacterial recovery | Whole blood/serum | Blood cultures (microbiology) |
| Yellow (ACD) | Acid Citrate Dextrose (ACD-A or ACD-B) | Citrate chelates calcium; dextrose preserves WBCs | Whole blood | Blood bank, HLA phenotyping, paternity testing, WBC preservation |
Key Additive Details
EDTA (Ethylenediaminetetraacetic Acid)
- Mechanism: Chelates (binds) calcium ions - calcium is essential for the clotting cascade
- Forms: K₂EDTA (spray-dried, no sample dilution - preferred) vs K₃EDTA (liquid, dilutes sample ~1-2%)
- Used in: Lavender, Pink, White, Royal Blue, Tan tubes
- Do NOT use for: coagulation tests, chemistry panels requiring ionized calcium, blood cultures
Sodium Citrate
- Mechanism: Chelates calcium (reversible - calcium can be added back)
- Concentration matters: 3.2% for coagulation (light blue), higher ratio for ESR (black)
- Critical note: The light blue tube must be filled to the fill line. Under-filling causes excess citrate relative to plasma volume → falsely prolonged PT/aPTT. In polycythemia (Hct >60%), the same problem occurs because plasma volume is reduced - the citrate volume must be adjusted.
Heparin
- Mechanism: Activates antithrombin III → inhibits thrombin and Factor Xa
- Forms: Sodium heparin, lithium heparin (lithium heparin preferred for most chemistry to avoid sodium or lithium interference)
- Do NOT use for: CBC (causes WBC clumping), coagulation tests, blood bank testing
Sodium Fluoride
- Mechanism: Inhibits enolase enzyme → blocks glycolysis → prevents glucose from being consumed by RBCs
- Preserves glucose for up to 5 days at room temperature
- May cause slight hemolysis if tube is under-filled
Clot Activator (Silica)
- Mechanism: Silica microparticles provide a surface for platelet activation and accelerate the intrinsic clotting pathway
- After collection, tube should be gently inverted 5-10 times, then allowed to clot for 30 minutes before centrifugation
Order of Draw (CLSI Standard)
The order of draw prevents additive carryover contaminating subsequent tubes:
| Priority | Tube Type | Cap Color |
|---|---|---|
| 1 | Blood culture bottles | Yellow (SPS) |
| 2 | Coagulation tube | Light blue |
| 3 | Serum tubes (no additive / clot activator ± gel) | Red, Gold, Orange |
| 4 | Heparin tubes (with or without gel) | Green, Light green |
| 5 | EDTA tubes (with or without gel) | Lavender, Pink, White |
| 6 | Glycolytic inhibitor | Gray |
Why this order? Tissue thromboplastin released during venipuncture can contaminate early tubes. Citrate (blue) must come before additive tubes to prevent EDTA or heparin carryover, which would falsely prolong coagulation times. EDTA drawn before heparin tubes prevents EDTA from chelating calcium and falsely affecting chemistry panels.
Common Mnemonics
"Boy Scout, Boys Rarely Go Leaping. Grab Gold."
- Blood cultures → Sodium citrate (Blue) → Red → Green → Lavender → Grey → Gold
Color = Purpose memory trick:
- 🔵 Blue = "Blood clotting tests" (coagulation)
- 🟣 Lavender/Purple = "Lab hematology" (CBC)
- 🟢 Green = "Go chemistry" (plasma chemistry, stat)
- ⬜ Grey = "Glucose guard" (glycolysis inhibitor)
- 🟡 Gold = "General chemistry" (SST serum)
- 🩷 Pink = "Patient blood bank" (type & cross)
Special Notes
| Clinical Situation | Implication |
|---|---|
| Polycythemia (Hct >60%) | Citrate (blue tube) must be adjusted - too much anticoagulant relative to plasma volume falsely prolongs coagulation times |
| IgA deficiency | Plasma-containing tubes relevant - IgA in donor plasma can cause transfusion reactions |
| Molecular/PCR testing | White tube (EDTA + gel) or pink tube preferred for DNA/RNA isolation from plasma |
| Trace element testing | Only royal blue or dark blue (special metal-free stopper) - regular tubes leach metals and contaminate samples |
| Blood alcohol / legal specimens | Gray tube with fluoride (inhibits in vitro ethanol production by yeast/bacteria) |
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods - Table 3.4 (Tube Color and Anticoagulant/Additive), p. 2012-2013
- Quick Compendium of Clinical Pathology 5th ed. - Selected blood collection tubes table, p. 192
- BD Vacutainer Tube Guide - manufacturer specifications
- CLSI GP41 Order of Draw Standard
This is a shared conversation. Sign in to Orris to start your own chat.