Principles of disaster management
Reading File
Searching the Web
principles of disaster management framework 2024
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have excellent material from multiple authoritative textbooks. Here is the comprehensive answer:
Principles of Disaster Management
Definition
The WHO defines a disaster as "a sudden ecologic phenomenon of sufficient magnitude to require external assistance" - essentially any event that overwhelms the resources of the region in which it occurs. The UNISDR defines disaster risk management as "the systematic process of using administrative decisions, organizations, operational skills and capacities to implement policies, strategies and coping capacities of the society and communities to lessen the impacts of natural hazards and related environmental and technological disasters."
- Park's Textbook of Preventive and Social Medicine
- Tintinalli's Emergency Medicine: A Comprehensive Study
The Disaster Cycle
The three fundamental aspects of disaster management correspond to different phases in the disaster cycle:
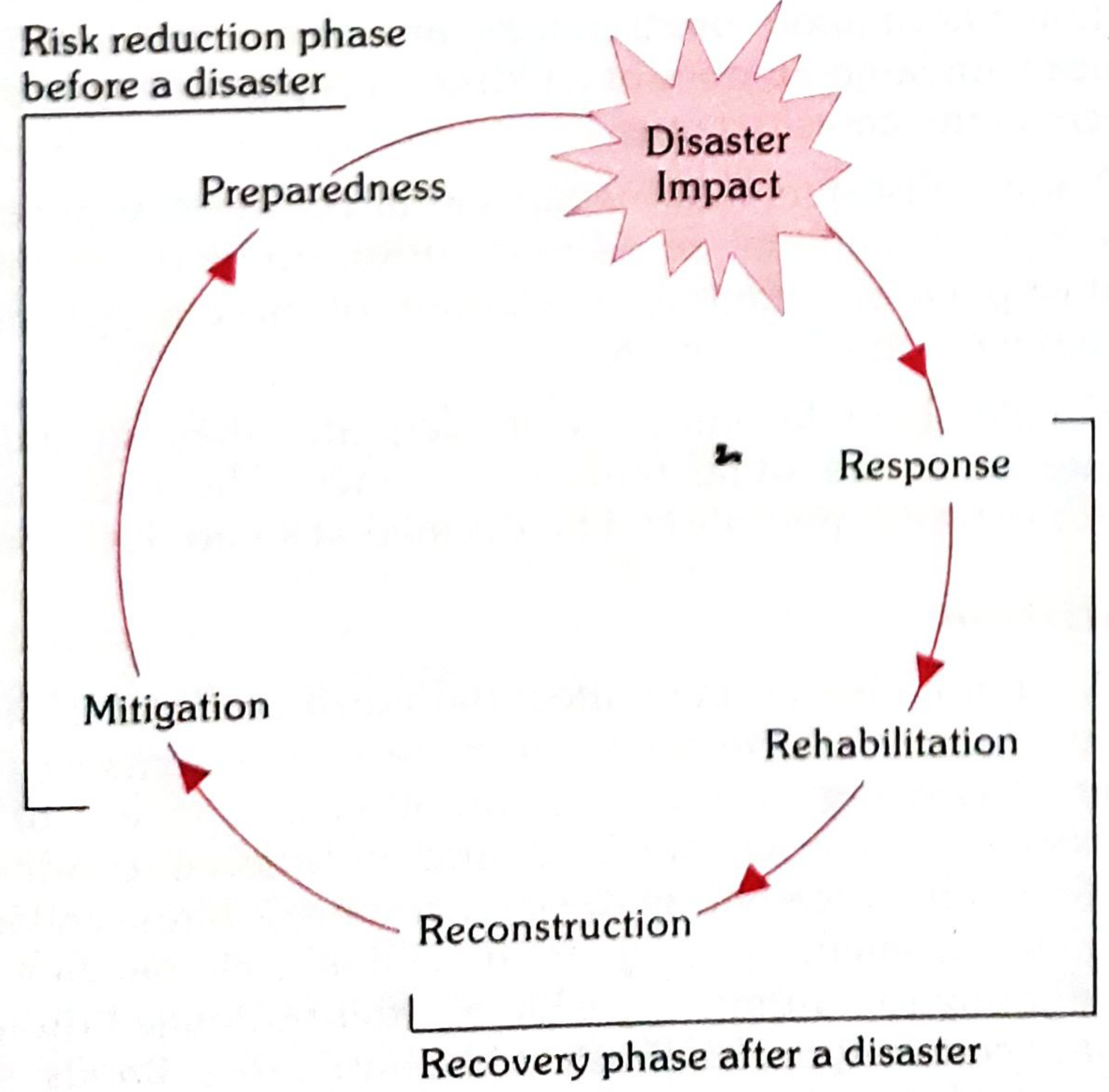
Fig. 1 - Management sequence of a sudden-onset disaster (Park's Textbook)
The cycle has two broad phases:
- Risk Reduction Phase (before a disaster): Preparedness → Mitigation
- Recovery Phase (after a disaster): Response → Rehabilitation → Reconstruction
1. Mitigation (Pre-Disaster - Risk Reduction)
Mitigation refers to all measures taken to reduce or eliminate the risk of a disaster or to lessen its consequences. It comprises:
- Structural measures: Earthquake-resistant construction, flood embankments, early warning systems, land-use regulation
- Non-structural measures: Legislation, public awareness, land zoning, insurance schemes, training programs
The goal is to reduce vulnerability so that hazards do not become disasters.
2. Preparedness (Pre-Disaster - Risk Reduction)
Preparedness is the state of readiness to deal effectively with a disaster when it strikes. Key elements include:
Hazard Vulnerability Analysis (HVA)
A planning group must assess which disasters are most likely to occur in the local geographic area (e.g., earthquake planning on the West Coast, hurricane planning on the Gulf Coast). This includes proximity to industrial sites, chemical depots, transportation hubs, and terrorist targets.
The Hospital Emergency Operations Plan
Disaster planning must include:
- A diverse hospital planning group meeting regularly to assess hazards
- Short- and long-term plans with exercises and drills
- Specific plans for radiation, explosions, mass casualties, and decontamination
Key Preparedness Components
| Component | Detail |
|---|---|
| Hospital-Community Coordination | Integration with local emergency agencies and national response assets |
| Incident Command System (ICS) | A standardized management structure ensuring clear command |
| Supplies stockpile | Hospitals should maintain at least 96 hours of independent supply |
| Staff training & exercises | Regular drills to test and update the disaster plan |
| Communications | Backup systems when normal infrastructure fails |
- Tintinalli's Emergency Medicine, Chapter 2 (Disaster Preparedness)
3. Response (During/Immediately After Disaster)
Disaster Characteristics That Drive Response
- The vast majority (~80%) of casualties self-transport to the nearest facility rather than via prehospital services
- Peak ED volumes occur 2-3 hours after an acute event
- Even in acute events, volumes remain elevated for days to weeks
- In nonacute events (e.g., pandemic), surge is slower but prolonged
Core Response Principles
a) Search, Rescue, and First Aid
Organized relief services can meet only a small fraction of the immediate demand after a major disaster. The most immediate help comes from uninjured survivors - the community is the first responder.
b) Triage
When casualties overwhelm facility capacity, the principle of "first come, first treated" is abandoned. Triage classifies the injured based on severity and likelihood of survival with prompt intervention:
- Highest priority: Patients whose prognosis can be dramatically improved by simple intervention
- Lowest priority: Moribund patients requiring extensive resources with uncertain benefit
- Goal: Maximum benefit to the greatest number
Standard triage uses color coding (red = immediate, yellow = delayed, green = minor, black = expectant/deceased).
c) Field Care and Hospital Response
- Maximize bed availability and surgical services
- Redirect health service resources to disaster priorities
- Establish a Family Information Center (to prevent families from interfering with care)
- Set up a Volunteer Coordination Center (to credential and deploy volunteers)
- Designate a single Media Center with a public information officer
- Pre-designate areas for decontamination, triage, major/minor casualties, psychiatric care, and the morgue
d) Decontamination
For chemical, biological, radiologic, or nuclear (CBRN) events, decontamination must occur external to the ED before patients enter the facility.
- Tintinalli's Emergency Medicine; Park's Textbook
4. Recovery (Post-Disaster)
Recovery involves restoring conditions to an acceptable level and comprises:
Rehabilitation
Short-term restoration of critical services - water, power, sanitation, temporary shelter, and basic healthcare. This also includes psychosocial support and disaster stress management for both victims and responders.
Reconstruction
Longer-term rebuilding of infrastructure, livelihoods, and governance systems, ideally with built-in risk reduction so the reconstructed community is less vulnerable than before.
Types of Disasters
| Type | Definition | Examples |
|---|---|---|
| Natural | Caused by naturally occurring events | Earthquakes, tsunamis, hurricanes, volcanic eruptions, pandemic influenza |
| Man-made (unintentional) | Non-natural events not purposefully produced | Vehicle crashes, industrial accidents, building fires |
| Man-made (intentional) | Deliberately caused | Terrorism, bioterrorism, chemical attacks |
| Internal (hospital) | Occurs within the hospital | Power failure, bomb scare, lab accident |
| External | Occurs outside the hospital | Mass casualty transport accident |
Core Overarching Principles
| Principle | Meaning |
|---|---|
| All-Hazards Approach | Plan generically so the same framework can cover any type of disaster |
| Command and Control | Clear chain of command through ICS to prevent chaos |
| Community Participation | Communities are the first responders; build local capacity |
| Inter-agency Coordination | Local, state, federal, and international bodies must work together |
| Sustainability | Plans must be financially and operationally sustainable |
| Equity | Vulnerable populations (elderly, disabled, poor) need targeted plans |
| Lessons Learned | Every event should be evaluated and the plan updated accordingly |
| Mental Health Integration | Address psychological needs of survivors and responders |
| Build Back Better | Reconstruction should reduce, not reproduce, vulnerability |
Key Global Frameworks
- Sendai Framework for Disaster Risk Reduction (2015-2030): The international blueprint, shifting focus from disaster management to disaster risk management, with four priorities: understanding risk, strengthening governance, investing in risk reduction, and enhancing preparedness for effective response.
- Hyogo Framework (2005-2015): The predecessor framework that established the concept of building resilience.
- UNISDR (now UNDRR): The UN body coordinating global disaster risk reduction.
Sources: Park's Textbook of Preventive and Social Medicine | Tintinalli's Emergency Medicine: A Comprehensive Study | Rosen's Emergency Medicine: Concepts and Clinical Practice | Goldman-Cecil Medicine
Rule of halves in hypertension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"rule of halves" hypertension
Finding Sources
Reading Article
PMID: 36149103
Finding Sources
Finding Sources
Searching PubMed
hypertension awareness treatment control cascade global
Finding Sources
Searching PubMed
hypertension care cascade awareness treatment control
Reading Article
PMID: 37901590
Reading Article
PMID: 41495934
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, multi-source material. Here is the complete answer:
Rule of Halves in Hypertension
Origin and Definition
The Rule of Halves is a classical epidemiological concept first described by Hart JT (1970) in the UK, later reinforced by Shaper et al. It describes the enormous gap between the true burden of hypertension in a population and effective clinical management through a cascade of "halves."
The rule states:
Of all hypertensive individuals in a population:
- Only 1/2 are aware of their condition (diagnosed)
- Of those diagnosed, only 1/2 are on treatment
- Of those on treatment, only 1/2 have their blood pressure controlled
The Cascade in Numbers
Starting with 100 hypertensive individuals in a population:
| Step | Number | Fraction of Total |
|---|---|---|
| Total hypertensives in population | 100 | 100% |
| Known/diagnosed (aware) | 50 | 50% |
| Receiving treatment | 25 | 25% |
| Adequately controlled on treatment | 12-13 | ~12.5% |
This means that only about 1 in 8 hypertensives in the community actually has their blood pressure under adequate control - a striking illustration of the treatment gap.
Why It Matters
Hypertension is the commonest cardiovascular disorder and "the major risk factor for cardiovascular mortality, accounting for 20-50% of all deaths." It is the leading risk factor for premature death and disability globally. Yet despite effective, affordable treatment being available, the cascade of undiagnosis, undertreatment, and poor control remains enormous.
- Park's Textbook of Preventive and Social Medicine
The rule is not merely historical trivia - it frames public health priorities by pinpointing where the care system fails: screening, linkage to care, or adherence and effectiveness of treatment.
The Three Gaps Explained
Gap 1 - Unawareness (Undiagnosed)
- Hypertension is largely asymptomatic ("silent killer") until complications arise
- Many people never present for blood pressure measurement
- Barriers: lack of screening programs, low health literacy, limited access to healthcare, absence of routine check-ups
Gap 2 - Untreated (Diagnosed but Not on Medication)
- Patients may be told they have hypertension but not started on pharmacotherapy
- Reasons: "white coat" hesitancy, patient refusal, physician inertia, cost of medications, lifestyle modification preferred without follow-up
- In India (NFHS-4 data): 72% of known hypertensives were not availing treatment - far worse than the "half" the rule predicts, suggesting the rule underestimates the treatment gap in low-income settings (Maroof et al., 2022 [PMID: 36149103])
Gap 3 - Uncontrolled (Treated but Not at Target)
- Poor adherence to medication
- Inadequate dosing or drug selection
- White-coat effect vs. true blood pressure at home
- Comorbidities and drug interactions
- Lack of follow-up and monitoring
Is the Rule Still Valid Today?
The rule is a useful mnemonic model but its exact fractions have shifted with improved health systems in high-income countries. Contemporary data paints a more nuanced picture:
-
A 2023 systematic review and meta-analysis across low-income settings (95 studies, Lamloum et al., PMID: 37901590) found:
- Mean hypertension prevalence: 33%
- Awareness: 48% (close to the "half")
- Treatment: 35% (worse than expected)
- Control: 16% (worse than the rule predicts)
- In LICs and Sub-Saharan Africa, all figures were even worse
-
A 2026 global review (O'Connell et al., PMID: 41495934) notes that despite availability of effective therapy, "hypertension awareness, treatment, and control remain inadequate globally."
-
In high-income countries, the treatment and control gaps have improved substantially, but unawareness remains a persistent problem.
So the rule of halves has evolved into the concept of the "hypertension care cascade" - a more nuanced, step-by-step framework to quantify gaps at each stage.
Prevention Strategies Targeting Each Gap
As described in Park's Textbook, the WHO recommends two complementary prevention approaches:
Closing Gap 1 (Unawareness) - Screening
- Population strategy: Universal BP screening at all healthcare contacts, community health camps
- High-risk strategy: Targeted screening of those with family history, obesity, diabetes, smokers
- Health education campaigns
- Self-monitoring devices and patient self-care programs
Closing Gap 2 (Undertreatment) - Linkage to Care
- Improving healthcare access and affordability
- Physician training to overcome clinical inertia
- Fixed-dose combination (FDC) therapies to simplify regimens
- Community health worker programs for follow-up
Closing Gap 3 (Poor Control) - Adherence and Optimization
- Team-based care models (nurses, pharmacists, allied health)
- Regular BP monitoring and feedback
- Lifestyle modifications: salt restriction (<5 g/day), weight reduction, exercise, smoking cessation, stress management
- Universal healthcare facility-based screening
- Patient education and self-care (log books, home BP monitoring)
Extended / Modern "Rule of Halves"
In some modern adaptations, the cascade is extended to include a fourth step:
| Step | Population |
|---|---|
| All hypertensives | 100% |
| Aware/diagnosed | ~50% |
| Treated | ~25% |
| Controlled | ~12.5% |
| Controlled AND free of end-organ damage | ~6% |
This "rule of eighths" or extended cascade emphasizes that even controlled hypertension does not guarantee absence of cardiovascular target organ damage.
Clinical and Public Health Significance
- Iceberg phenomenon: Hypertension, like many chronic diseases, has a massive "submerged" undiagnosed component
- Drives screening policy: Supports argument for population-wide, opportunistic BP measurement at every healthcare contact
- Program evaluation tool: Used to monitor progress of national hypertension control programs (e.g., India's NPCDCS program)
- Applicable to other conditions: The "rule of halves" concept has been extended to diabetes mellitus, dyslipidemia, and other chronic NCDs
Sources: Park's Textbook of Preventive and Social Medicine | Maroof et al., Indian J Public Health 2022 [PMID: 36149103] | Lamloum et al., Int J Public Health 2023 [PMID: 37901590] | O'Connell et al., Curr Opin Nephrol Hypertens 2026 [PMID: 41495934]
Growth chart and its uses
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here it is:
Growth Chart and Its Uses
Definition
The growth chart, also called the "Road-to-Health Chart", was first designed by David Morley and later modified by the WHO. It is a visible display of a child's physical growth and development, designed primarily for the longitudinal follow-up (growth monitoring) of a child so that changes over time can be interpreted.
Weight is used as the primary measure because it is the most sensitive indicator of growth - any deviation from normal is easily detected by comparison with reference curves. A child can lose weight, but not height.
- Park's Textbook of Preventive and Social Medicine
WHO Child Growth Standards (2006)
In 1993, the WHO undertook a comprehensive review of anthropometric references and concluded that the older NCHS (National Centre for Health Statistics) growth references (used since the late 1970s) did not adequately represent early childhood growth.
A Multicentre Growth Reference Study (MGRS) was conducted between 1997 and 2003 across:
- Brazil, Ghana, India, Norway, Oman, and USA
- 9,440 healthy breastfed infants and young children (0-60 months, both sexes)
- Mothers who breastfed their children and did not smoke during/after pregnancy
- Widely diverse ethnic backgrounds and cultural settings
New standards generated for boys and girls aged 0-60 months:
- Length/height-for-age
- Weight-for-age
- Weight-for-length
- Weight-for-height
- BMI-for-age (new addition compared to NCHS set)
The new WHO standards depict normal early childhood growth under optimal environmental conditions and can be used to assess children everywhere, regardless of ethnicity, socioeconomic status, or type of feeding - making them a prescriptive standard (what should be), not merely a descriptive reference (what is).
WHO vs. NCHS: Key Differences
| Feature | NCHS Reference (old) | WHO Standards (2006) |
|---|---|---|
| Basis | Descriptive (observed growth) | Prescriptive (optimal growth) |
| Population | US-based, formula-fed | Multi-ethnic, breastfed |
| Age range | 0-18 years | 0-5 years (MGRS); 5-19 years (WHO reference) |
| Stunting rates | Lower | Higher (especially infancy) |
| Wasting rates | Lower | Substantially higher in infancy |
| Overweight rates | Lower | Greater prevalence |
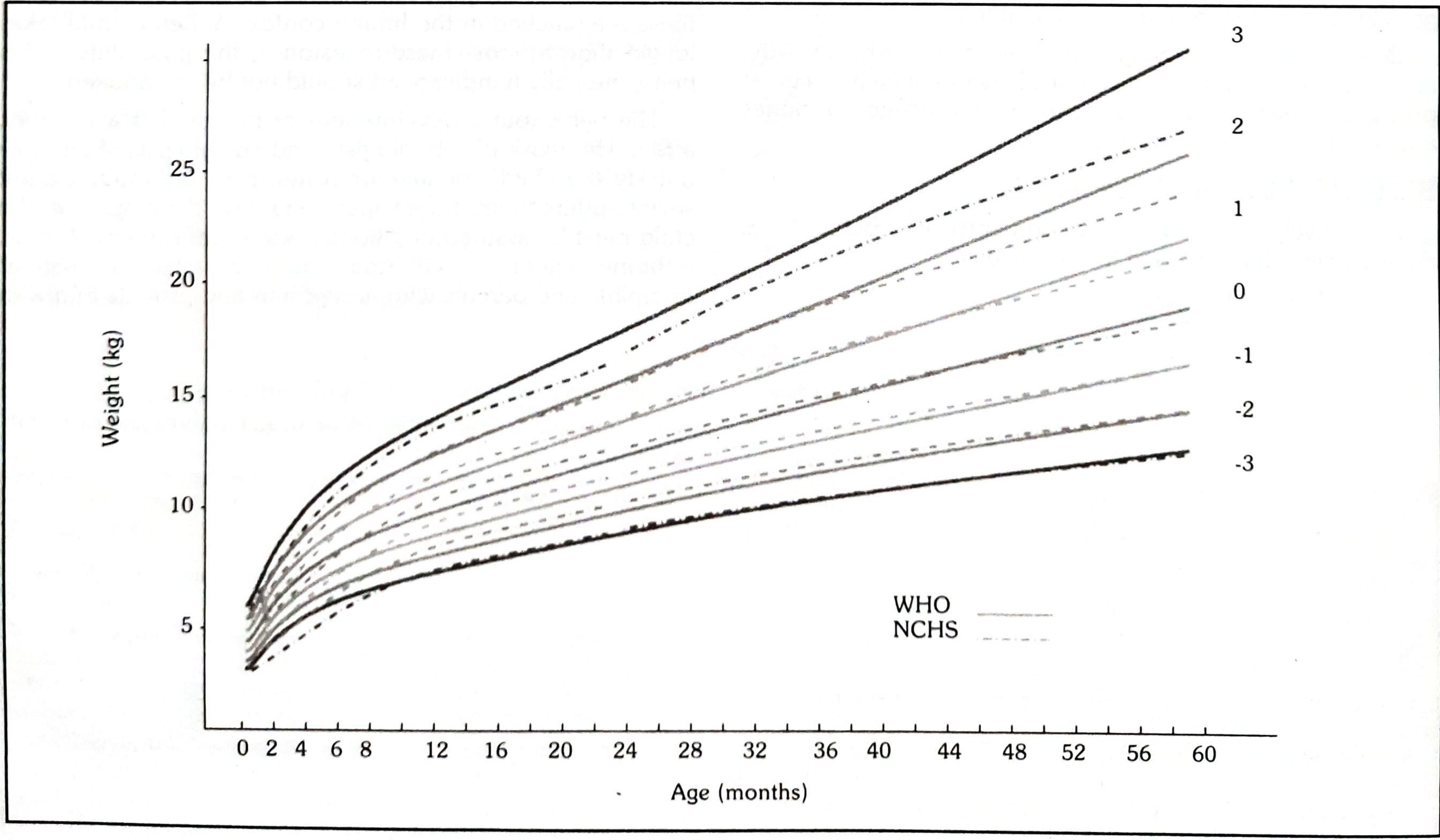
Comparison of WHO vs NCHS Weight-for-Age Z-scores for Boys (0-60 months):
Comparison of WHO vs NCHS Weight-for-Age Z-scores for Girls (0-60 months):
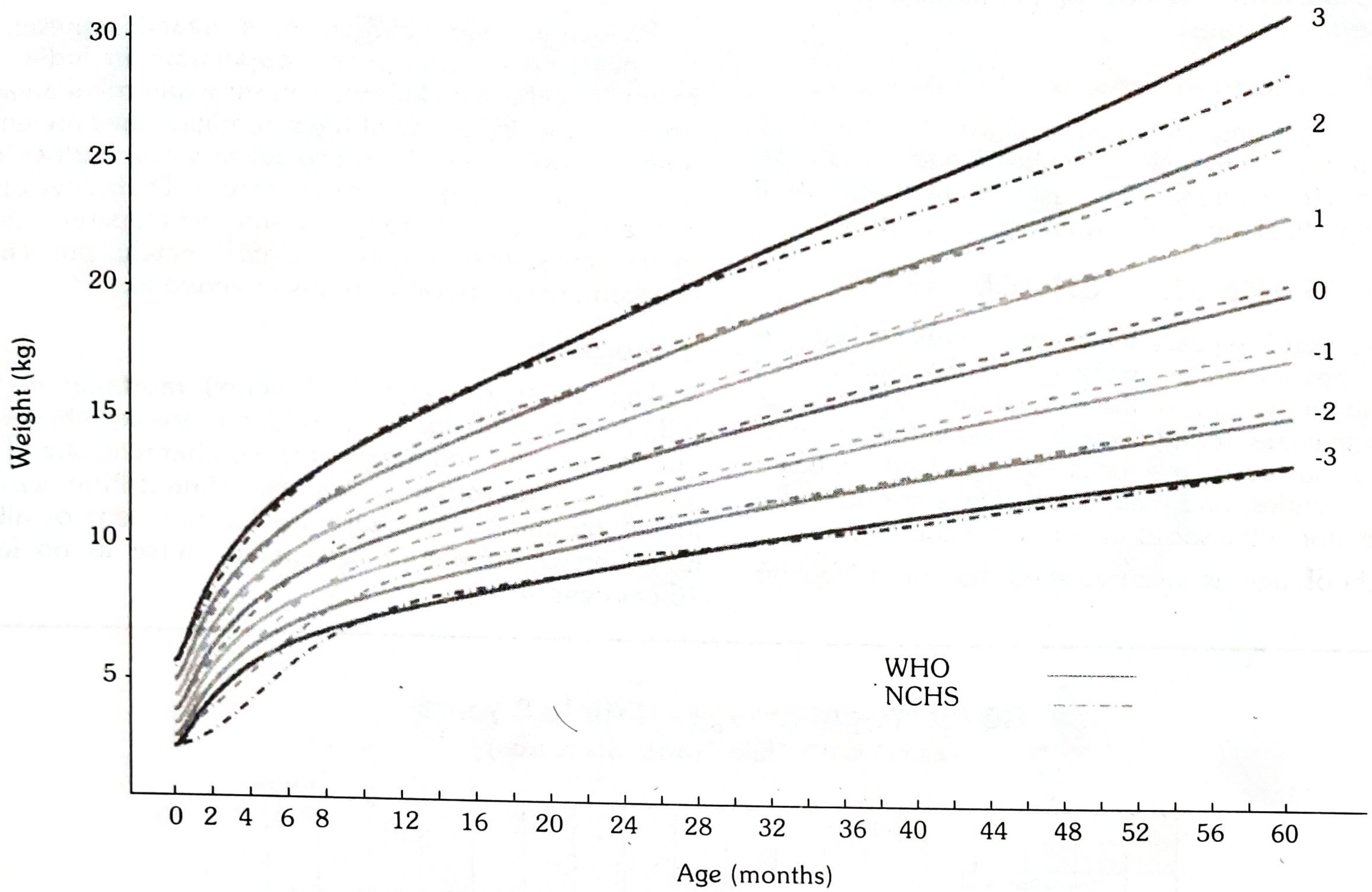
Source: Park's Textbook of Preventive and Social Medicine, Figs. 5 & 6
The curves show Z-score lines labeled +3, +2, +1, 0, -1, -2, -3 plotted against age (months) and weight (kg), from birth to 60 months.
Growth Chart Used in India
India adopted the WHO Child Growth Standards (2006) in February 2009 for monitoring young child growth within the National Rural Health Mission (NRHM) and the ICDS (Integrated Child Development Services).
Mother and Child Protection (MCP) Card
A joint MCP Card was developed which provides space for:
- Family identification and registration
- Birth record and pregnancy record
- Care during pregnancy
- Registration under Janani Suraksha Yojana
- Immunization details
- Breastfeeding and supplementary food introduction timeline
- Developmental milestones
- Birth spacing information
The card is kept by the mother and brought to the health centre at each visit. It is easily understood by both health workers and the mother.
Zones on the Growth Chart
| Zone | Z-score | Status |
|---|---|---|
| Normal zone | Above -2 SD | Healthy |
| Undernutrition | Below -2 SD | Underweight |
| Severely underweight | Below -3 SD | Severe undernutrition |
"It is the direction of growth that is more important than the position of dots on the line." Flattening or falling of the weight curve signals growth failure - the earliest sign of protein-energy malnutrition (PEM), which may precede clinical signs by weeks to months.
7 Uses of the Growth Chart
(as enumerated in Park's Textbook)
1. Growth Monitoring
The primary use - longitudinal tracking of a child's weight gain over time to detect changes at the earliest opportunity, well before clinical signs appear.
2. Diagnostic Tool
Identifies "high-risk" children - malnutrition can be detected long before signs and symptoms become apparent. A child whose curve flattens or falls is flagged for intervention immediately.
3. Planning and Policy Making
By grading malnutrition, the chart provides an objective basis for:
- Planning child nutrition programs at local and national levels
- Allocating resources (supplementary feeding programs, ICDS)
- Setting targets for program evaluation
4. Educational Tool
Because of its visual, easy-to-understand character:
- Mothers can be educated about their own child's health and nutrition
- Encourages active participation in growth monitoring
- Demystifies the concept of healthy growth for non-literate caregivers
5. Tool for Action
Guides the health worker on:
- What type of intervention is needed (dietary counselling, deworming, referral)
- Makes referrals to higher centres easier and more objective
- Triggers supplementary nutrition under ICDS programs
6. Evaluation
Provides a good method to evaluate:
- Effectiveness of corrective measures taken
- Impact of a program or special intervention for improving child growth and development
- Monitors response to therapeutic feeding
7. Tool for Teaching
Used as a teaching aid to illustrate:
- The importance of adequate feeding at each age
- The deleterious effects of diarrhoeal diseases on growth
- The relationship between infections and nutritional status
"The growth chart has been described as a passport to child health care. It has won international recognition and is now a standard method of monitoring children's health and nutritional status."
- Park's Textbook of Preventive and Social Medicine
Alternative Methods of Growth Monitoring
Growth charting (weight-for-age) is one method, but others exist - especially useful when age is not known:
| Indicator | What it Measures | Special Feature |
|---|---|---|
| Height-for-age | Stunting (chronic malnutrition) | Reflects past/chronic undernutrition |
| Weight-for-height | Wasting (acute malnutrition) | Age-independent |
| Mid-Upper Arm Circumference (MUAC) | Current nutritional status | Age-independent; quick field tool |
| BMI-for-age | Overweight and obesity | Useful in school-age children |
| Head circumference-for-age | Brain/neurological growth | Used in infants 0-2 years |
Interpretation of Z-scores and Percentiles
| Z-score | Percentile (approx.) | Interpretation |
|---|---|---|
| > +3 | > 99.9th | Obese/overweight |
| > +2 | > 97.7th | Overweight |
| 0 | 50th | Median (average) |
| < -1 | < 15.9th | Mild growth concern |
| < -2 | < 2.3rd | Underweight / Stunted / Wasted |
| < -3 | < 0.1st | Severely underweight / Severely stunted |
Summary Table
| Feature | Detail |
|---|---|
| Designed by | David Morley; modified by WHO |
| Also called | Road-to-Health Chart |
| Primary parameter | Weight (most sensitive growth indicator) |
| Standard used globally | WHO Child Growth Standards 2006 |
| Standard used in India | WHO 2006 (adopted Feb 2009) |
| Program linkage | ICDS, NRHM, MCP Card |
| Key principle | Direction of curve > absolute position |
| Critical sign | Flattening/falling curve = growth failure |
| Age range covered | 0-5 years (WHO MGRS); 5-19 years (WHO reference) |
Source: Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.