Give me mbbs level Knowledge on anxiety
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed. Here is the comprehensive MBBS-level knowledge on Anxiety:
Anxiety Disorders - MBBS Level
1. Definition and Normal vs. Pathological Anxiety
Fear is an expected emotional response to a real or perceived immediate threat. Anxiety is the anticipation of future danger - it is forward-looking and often without a clearly identifiable external stimulus.
Anxiety becomes a disorder when it is:
-
Excessive and out of proportion to the actual threat
-
Difficult or impossible to control
-
Persistent (lasting weeks to months)
-
Causes significant distress or impairment in social, occupational, or other functioning
-
Kaplan and Sadock's Synopsis of Psychiatry, p. 1249
2. Classification (DSM-5)
DSM-5 groups anxiety disorders separately from OCD and PTSD (which now have their own chapters). The main anxiety disorders are:
| Disorder | Core Feature |
|---|---|
| Separation Anxiety Disorder | Excessive fear of separation from attachment figures |
| Selective Mutism | Failure to speak in specific social situations |
| Specific Phobia | Fear/avoidance of a specific object or situation |
| Social Anxiety Disorder (Social Phobia) | Fear of embarrassment or scrutiny in social situations |
| Panic Disorder | Recurrent unexpected panic attacks + anticipatory anxiety |
| Agoraphobia | Fear/avoidance of situations where escape is difficult |
| Generalized Anxiety Disorder (GAD) | Excessive, uncontrollable worry about multiple domains for ≥6 months |
| Substance/Medication-Induced Anxiety Disorder | Due to intoxication or withdrawal |
| Anxiety Disorder Due to Another Medical Condition | Secondary cause |
Note: OCD, PTSD/Acute Stress Disorder, and adjustment disorders are no longer classified as anxiety disorders in DSM-5 - they have separate chapters.
3. Neurobiology of Anxiety
3a. The Amygdala - Center of Fear
The amygdala is an almond-shaped structure near the hippocampus that integrates sensory and cognitive information to determine whether a fear response is triggered.
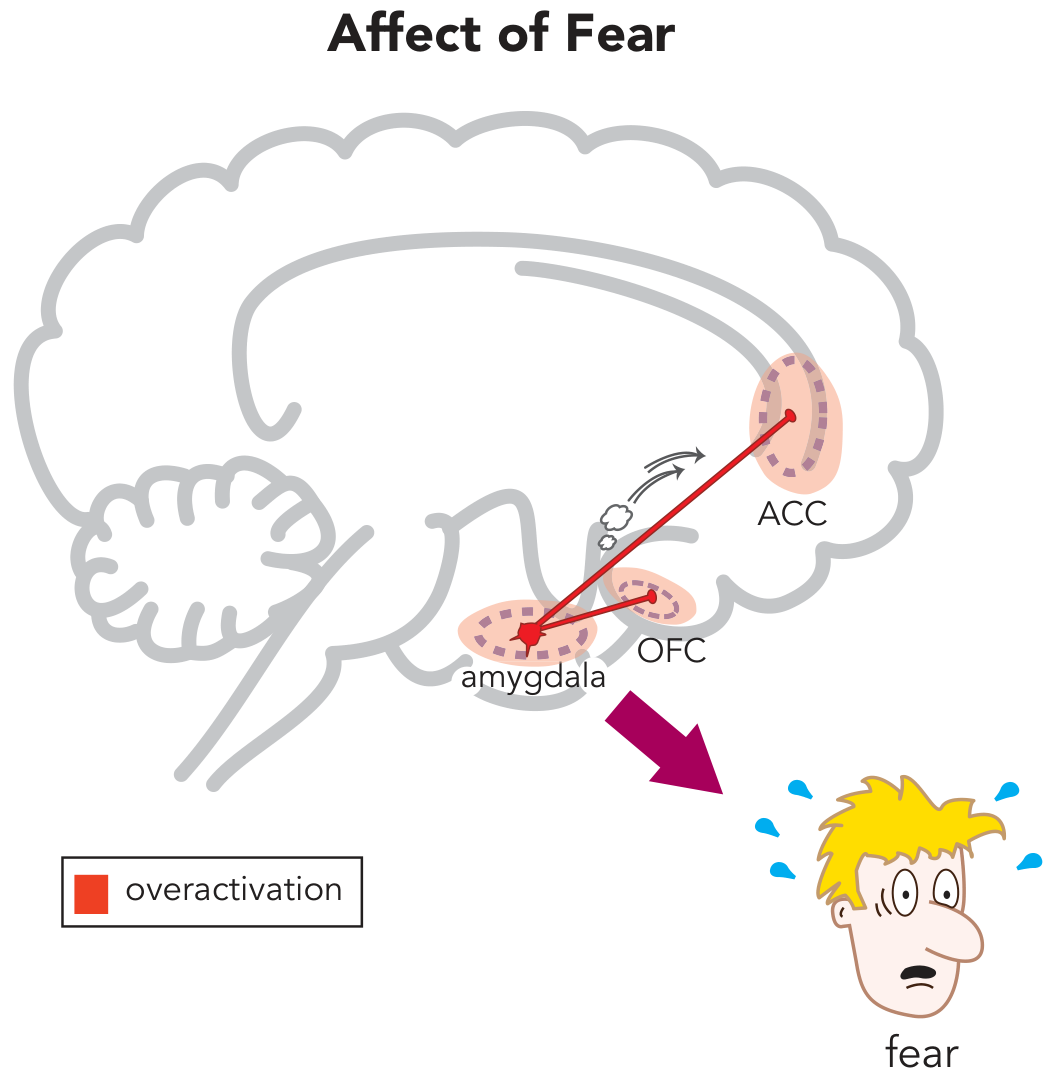
Key amygdala connections and outputs:
- Prefrontal cortex (OFC + ACC) - regulates the feeling of fear
- Periaqueductal gray (PAG) - mediates motor responses: fight, flight, or freeze
- Hypothalamus / HPA axis - triggers cortisol release; chronic activation leads to CAD, T2DM, stroke risk, and hippocampal atrophy
- Parabrachial nucleus - alters breathing (hyperventilation, dyspnea)
- Autonomic nervous system - tachycardia, sweating, palpitations, mydriasis
- Locus coeruleus - norepinephrine release
3b. CSTC Loops and Worry
The second core symptom - worry - is hypothetically linked to the Cortico-Striato-Thalamo-Cortical (CSTC) loop. This circuit underlies catastrophic thinking, apprehensive expectations, and obsessional worry seen in GAD.
3c. Key Neurochemical Systems
| System | Brain Regions | Role in Anxiety |
|---|---|---|
| Serotonin (5-HT) | Dorsal raphe, amygdala, hippocampus, PFC | Low 5-HT1A activity in PD and SAD - target of SSRIs/SNRIs |
| Norepinephrine | Locus coeruleus, amygdala, hypothalamus | Unrestrained activation drives autonomic symptoms |
| GABA | Substantia nigra, globus pallidus, amygdala | Reduced GABA-A activity disinhibits fear circuits |
| Glutamate | Amygdala, hippocampus, frontal cortex | Imbalance with GABA drives excessive amygdala output |
| HPA / Cortisol | Hippocampus, amygdala, hypothalamus | Dysregulated cortisol feedback |
| Dopamine | Amygdala, nucleus accumbens, PFC | Excessive mesocortical dopamine release |
- Kaplan and Sadock's Synopsis of Psychiatry, p. 1267-1269
- Stahl's Essential Psychopharmacology, p. 364-382
4. Specific Disorder Profiles
4a. Generalized Anxiety Disorder (GAD)
DSM-5 Criteria:
- Excessive anxiety and worry about multiple events/activities, most days, for ≥6 months
- Difficulty controlling the worry
- At least 3 of 6 somatic symptoms:
- Restlessness / feeling on edge
- Easy fatigability
- Difficulty concentrating / mind going blank
- Irritability
- Muscle tension
- Sleep disturbance
- Causes significant distress or impairment
- Not attributable to substances or another medical condition
(In children, only 1 somatic symptom required)
Key feature: Worries span multiple domains (job, finances, health, family), cannot be prioritized or set aside, and catastrophe feels imminent.
Scales used: GAD-7, Beck Anxiety Inventory (BAI), Hamilton Anxiety Rating Scale (HAM-A), State-Trait Anxiety Inventory (STAI)
4b. Panic Disorder
Panic attack = discrete episode of intense fear with ≥4 symptoms peaking within minutes:
- Palpitations/tachycardia
- Sweating
- Trembling/shaking
- Shortness of breath/smothering
- Choking sensation
- Chest pain
- Nausea/abdominal distress
- Dizziness/lightheadedness
- Derealization/depersonalization
- Fear of losing control or "going crazy"
- Fear of dying
- Paresthesias
- Chills or hot flushes
Panic Disorder DSM-5: Recurrent unexpected panic attacks + at least 1 month of:
- Persistent concern/worry about future attacks ("anticipatory anxiety"), OR
- Significant maladaptive change in behavior (avoidance)
Course: Onset typically late adolescence/early adulthood. Chronic but variable - ~30-40% become symptom-free long term; ~10-20% continue to have significant symptoms.
Agoraphobia often co-develops - avoidance of situations where escape is difficult (crowds, public transport, open spaces). It is now a separate diagnosis in DSM-5.
- Kaplan and Sadock's Synopsis of Psychiatry, p. 1255
4c. Social Anxiety Disorder (Social Phobia)
- Fear of social situations where one may be scrutinized or embarrassed
- The fear is of embarrassment in the situation, not the situation itself (distinguishes it from specific phobia)
- Marked avoidance or endurance with intense distress
- Duration ≥6 months
- Example: fear of public speaking, meeting new people, eating in public
4d. Specific Phobia
- Persistent, intense, irrational fear of a specific object/situation
- Specifiers: Animal, Natural environment, Blood-Injection-Injury (BII), Situational, Other
- Exposure causes immediate fear/anxiety
- Duration ≥6 months
- BII subtype is notable: can cause vasovagal syncope (bradycardia, hypotension) rather than the typical sympathetic arousal
4e. Separation Anxiety Disorder
-
Developmentally inappropriate, excessive anxiety about separation from attachment figures
-
Requires ≥3 symptoms (refusal to go to school, nightmares about separation, somatic complaints on separation, persistent worry about harm coming to attachment figure)
-
Duration: ≥4 weeks in children, ≥6 months in adults (DSM-5 now applies to adults too)
-
Behaviorally inhibited children (high resting HR, elevated morning cortisol, low HRV) are at highest risk
-
Kaplan and Sadock's Synopsis of Psychiatry, p. 624-625
5. Epidemiology
- Anxiety disorders are among the most common psychiatric conditions worldwide
- Affect 10-20% of children and adolescents
- Women are more commonly affected than men (approximately 2:1)
- High comorbidity: among separation anxiety, GAD, and social anxiety disorder in youth, a child has a 60% chance of having at least one of the others; 30% have all three
- High comorbidity with major depressive disorder (GAD and depression often co-occur; GAD may represent a prodromal or residual phase of depression)
- Substance use disorder commonly co-occurs and worsens prognosis
- Increased risk of suicide - must always be monitored
6. Differential Diagnosis
Medical causes to rule out:
- Hyperthyroidism (anxiety, palpitations, tremor)
- Pheochromocytoma (episodic hypertension, sweating, tachycardia)
- Hypoglycemia
- Cardiac arrhythmias
- Seizure disorders (especially complex partial seizures)
- Pulmonary embolism, asthma (dyspnea mimicking panic)
- Cushing's disease (HPA dysregulation)
- Drug withdrawal (alcohol, benzodiazepines, opioids)
Psychiatric differentiation:
- Panic disorder vs. specific phobia: panic attacks in phobia are cued/expected (situational); in panic disorder they are unexpected
- GAD vs. normal worry: GAD worry is excessive, uncontrollable, pervasive, and functionally impairing
- Social anxiety vs. panic: social anxiety fear is of embarrassment/scrutiny; panic disorder fear is of the attack itself
- OCD: obsessions cause anxiety but are ego-dystonic, intrusive, unwanted thoughts (separate category in DSM-5)
7. Treatment
7a. Pharmacotherapy
First-line for most anxiety disorders (GAD, Panic Disorder, Social Anxiety Disorder):
- SSRIs - safest, best-tolerated, broadest efficacy (e.g., sertraline, escitalopram, paroxetine, fluoxetine)
- SNRIs - venlafaxine, duloxetine; especially useful for GAD
Important note on SSRIs in panic disorder: May initially worsen panic attacks before improving them - start at low dose, warn the patient, and titrate slowly.
| Drug Class | GAD | Panic Disorder | Social Anxiety |
|---|---|---|---|
| SSRIs | First line | First line | First line |
| SNRIs | First line | First line | First line |
| TCAs | Second line | Second line | Not recommended |
| MAOIs | Insufficient evidence | Second line | Second line |
| Benzodiazepines | Second line | Second line | Second line |
| Buspirone | Second line (GAD specific) | Second line | Second line |
| Pregabalin | Second line | Insufficient evidence | Second line |
| Quetiapine (atypical AP) | Second line | Insufficient | Not recommended |
| Beta-blockers (propranolol) | Only for performance anxiety | - | Performance anxiety only |
- Kaplan and Sadock's Synopsis of Psychiatry, p. 1258
Benzodiazepines (e.g., alprazolam, clonazepam, diazepam):
- Mechanism: positive allosteric modulation of GABA-A receptors in the amygdala → reduces amygdala overactivation
- Advantage: rapid onset (unlike SSRIs which take 2-4 weeks)
- Disadvantages: dependence, withdrawal, cognitive dulling, abuse potential
- Guidelines: mostly limit to short-term use or as adjunct to SSRIs during initiation phase
- High-potency BZDs (alprazolam, clonazepam) preferred for panic disorder
Buspirone:
- 5-HT1A partial agonist
- Effective for GAD specifically, requires chronic use (like SSRIs)
- No dependence/withdrawal, no sedation, no abuse potential
- Does not work for panic disorder or social anxiety
Pregabalin/Gabapentin (alpha-2-delta ligands):
-
Block presynaptic voltage-sensitive calcium channels → reduce glutamate release in the amygdala
-
Reduce both fear (amygdala) and worry (CSTC loops)
-
Stahl's Essential Psychopharmacology, p. 366-382
7b. Psychotherapy
Cognitive-Behavioral Therapy (CBT):
- Most evidence-based psychotherapy for all anxiety disorders
- Substantial effect for GAD, panic disorder, and social anxiety disorder
- Components: psychoeducation, cognitive restructuring, behavioral exposure
- For panic disorder: corrects false belief that mild bodily sensations signal impending doom/death
- For social anxiety: individual or group CBT; considered first-line by some guidelines
Exposure Therapy:
- In vivo exposure = treatment of choice for specific phobia
- Systematic desensitization for phobias
- Improves agoraphobia alongside panic treatment
Behavioral Therapy for agoraphobia: Rapid and complete reduction of avoidance behaviors.
Interpersonal Therapy (IPT): Also supported for anxiety disorders.
Combined treatment (pharmacotherapy + CBT): Generally superior to either alone, though some guidelines treat them as equivalent for first-line use.
- Kaplan and Sadock's Synopsis of Psychiatry, p. 1259
8. Course and Prognosis
- Anxiety disorders are generally chronic, with multiple relapses
- GAD: multiple relapses; some relapses occur long after initial episode (giving false sense of recovery)
- Panic disorder: ~30-40% symptom-free long term; ~50% mildly symptomatic; ~10-20% severely symptomatic
- Good prognostic factors: good premorbid functioning, brief duration of illness, absence of comorbid substance use
- Poor prognostic factors: comorbid depression, substance use disorder, personality disorder
- All anxiety disorders carry an increased suicide risk - regular monitoring is mandatory
9. Key Rating Scales (Clinical Tools)
| Scale | Use |
|---|---|
| GAD-7 | Screening and severity of GAD |
| Hamilton Anxiety Rating Scale (HAM-A) | Clinician-rated anxiety severity |
| Beck Anxiety Inventory (BAI) | Patient-rated anxiety severity |
| Hospital Anxiety and Depression Scale (HADS) | Screens both anxiety and depression |
| State-Trait Anxiety Inventory (STAI) | Distinguishes situational vs. trait anxiety |
| Panic Disorder Severity Scale (PDSS) | Monitors panic disorder treatment response |
10. Quick Memory Aid - "WATCHME" for Anxiety Exam Points
| Letter | Point |
|---|---|
| W | Worry (GAD = ≥6 months, multiple domains, ≥3/6 symptoms) |
| A | Amygdala (center of fear neurobiology) |
| T | Treatment first-line = SSRIs/SNRIs + CBT |
| C | Chronic course - monitor for relapse and suicide |
| H | HPA axis dysregulation - link to medical comorbidities |
| M | Medical causes must be ruled out first |
| E | Exposure therapy = first-line for specific phobia |
Sources:
- Kaplan and Sadock's Synopsis of Psychiatry (Anxiety disorders chapter, pp. 624-625, 1249-1269)
- Stahl's Essential Psychopharmacology: Neuroscientific Basis (Chapter 8: Anxiety, Trauma, and Treatment, pp. 359-382)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry (Neurobiology chapter)
CN you make a slide presentation on this topic
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/anxiety-pptx && ls /home/daytona/workspace/anxi…
This is a shared conversation. Sign in to Orris to start your own chat.