Corrigan pulse
Reading File
Finding Sources
Searching the Web
Corrigan pulse water hammer pulse aortic regurgitation clinical features mechanism
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I have everything needed for a thorough answer.
Corrigan's Pulse (Water-Hammer Pulse)
Definition and Eponym
Corrigan's pulse is the characteristic collapsing pulse of aortic regurgitation (AR). It is named after Sir Dominic John Corrigan, who described visible arterial pulsations in AR in his landmark 1832 publication "On permanent patency of the mouth of the aorta, or inadequacy of the aortic valves."
The term "water-hammer pulse" was coined by Sir Thomas Watson (1837/1842), referencing a Victorian toy - a sealed tube half-filled with water that produced a sharp thud when inverted, mimicking the abrupt pulse feel.
Technically, Corrigan's pulse = visible arterial pulsations; water-hammer pulse = the palpable collapsing character. In clinical practice, both terms are used interchangeably for the same sign.
Mechanism / Pathophysiology
In aortic regurgitation, blood leaks back from the aorta into the LV during diastole. This produces two key hemodynamic derangements:
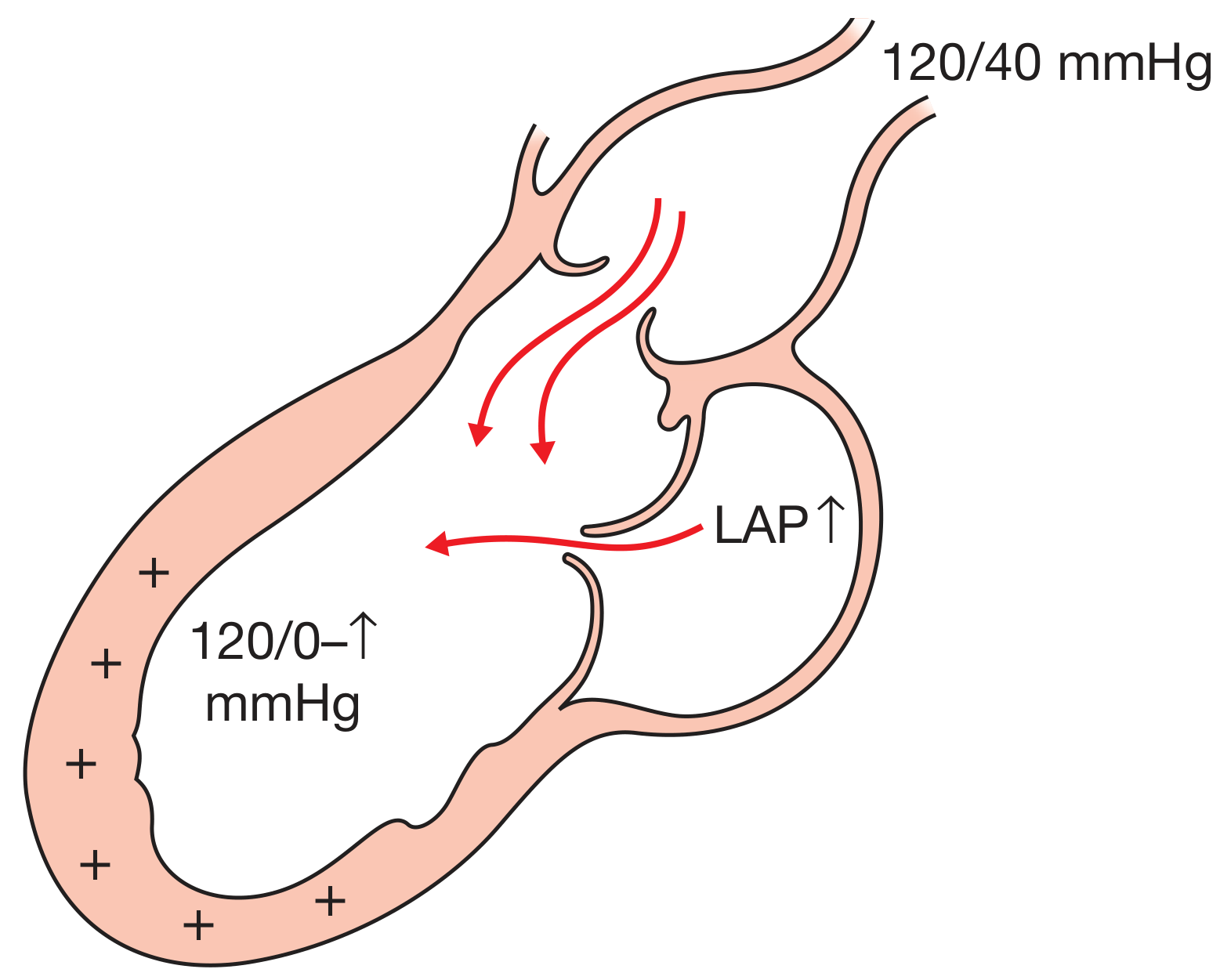
Haemodynamics of aortic regurgitation - Bailey & Love's Short Practice of Surgery, 28th Ed.
| Phase | Event | Effect on Pulse |
|---|---|---|
| Systole | Increased stroke volume (LV ejects both its normal output + the regurgitated volume) | Rapid, forceful upstroke - high systolic pressure |
| Diastole | Blood regurgitates back through incompetent aortic valve; aortic run-off into LV | Rapid, complete collapse - very low diastolic pressure |
The result is a wide pulse pressure (e.g., 120/40 or even 120/0 mmHg). The combination of high systolic + very low diastolic pressure creates the hallmark rapid rise-and-fall.
- Ganong's Review of Medical Physiology, 26th Ed.: "When the aortic valve is incompetent (aortic regurgitation), the pulse is particularly strong, and the force of systolic ejection may be sufficient to make the head nod with each heartbeat. The pulse in aortic regurgitation is called a Corrigan or water-hammer pulse."
- Fuster and Hurst's The Heart, 15th Ed.: "The combination of increased stroke volume and regurgitation gives rise to an arterial pulse that is increased in amplitude - 'bounding' - that also collapses very quickly. This is so-called water hammer pulse, typical of severe isolated aortic regurgitation."
How to Elicit
- Grasp the patient's wrist with your whole hand
- Raise the forearm above the level of the heart
- Feel the pulse - the sudden slapping impact followed by immediate collapse is accentuated by elevation (gravity empties the vessel rapidly)
Best felt at: radial artery (elevated), carotid, brachial, femoral arteries.
Causes
Any condition producing a wide pulse pressure or large stroke volume with low diastolic runoff:
| Cause | Mechanism |
|---|---|
| Aortic regurgitation (classic) | Regurgitant flow - low diastolic pressure |
| Patent ductus arteriosus (PDA) | Aortic diastolic runoff into pulmonary artery |
| Arteriovenous fistula/malformation | Diastolic runoff into venous system |
| Severe anaemia | High cardiac output, low peripheral resistance |
| Thyrotoxicosis | Hyperdynamic circulation |
| Pregnancy | Increased CO, decreased SVR |
| Fever | Vasodilation, increased CO |
| Complete heart block | Long diastole - very low diastolic pressure |
| Paget's disease of bone | Arteriovenous shunting in bone |
- S. Das Manual on Clinical Surgery, 13th Ed.: "Water-hammer pulse of aortic regurgitation or thyrotoxicosis..."
Associated Peripheral Signs of Aortic Regurgitation
All caused by the same wide pulse pressure; these accompany Corrigan's pulse in severe chronic AR:
| Sign | Description |
|---|---|
| de Musset's sign | Pulsatile head bobbing with each heartbeat |
| Quincke's sign | Capillary pulsations visible at the proximal nail bed (alternate flushing/blanching) - seen with gentle pressure or transillumination of fingertip |
| Duroziez's sign | Systolic murmur when femoral artery compressed proximally + diastolic murmur when compressed distally ("to-and-fro" femoral bruit) |
| Traube's sign | "Pistol shot" booming systolic and diastolic sounds heard over the femoral artery |
| Müller's sign | Systolic pulsations of the uvula |
| Hill's sign | Popliteal BP exceeds brachial BP by >20 mmHg (in severe AR); indicates severity |
| Corrigan's sign | Visible pulsations in the neck (carotid arteries) |
| Bisferiens pulse | Two systolic peaks palpable when AR is the predominant lesion in mixed aortic valve disease |
- Braunwald's Heart Disease, 10th Ed.: "The Traube sign...refers to booming systolic and diastolic sounds heard over the femoral artery; the Müller sign consists of systolic pulsations of the uvula; and the Duroziez sign consists of a systolic murmur heard over the femoral artery when it is compressed proximally and a diastolic murmur when it is compressed distally."
- Bailey and Love's Short Practice of Surgery, 28th Ed.: full list confirmed.
Key Murmur of AR (for context)
- Early diastolic, decrescendo, high-pitched, blowing
- Heard best: left sternal border, 3rd-4th intercostal space, patient sitting up and leaning forward, breath held in expiration
- An Austin Flint murmur (mid-diastolic rumble at the apex) may also be present - caused by the regurgitant jet vibrating the anterior mitral leaflet
- Severity correlates better with duration than intensity of the murmur
Clinical Pearl
In acute AR (e.g., aortic dissection, endocarditis), Corrigan's pulse and the wide pulse pressure may be absent or minimal - the LV has not had time to dilate and adapt, so there is little increase in stroke volume. The murmur may also be very short or inaudible. This makes acute AR a diagnostic trap.
- Tintinalli's Emergency Medicine: "In acute disease, the murmur may be inaudible due to tachycardia, tachypnea, and rales."
Sources: Braunwald's Heart Disease (10th Ed.) | Fuster & Hurst's The Heart (15th Ed.) | Ganong's Review of Medical Physiology (26th Ed.) | Bailey & Love's Short Practice of Surgery (28th Ed.) | Tintinalli's Emergency Medicine (9th Ed.) | S. Das Manual on Clinical Surgery (13th Ed.)
Hoffman sign
Finding Sources
Searching the Web
Hoffmann sign neurological upper motor neuron clinical significance elicitation
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I have comprehensive data from multiple authoritative sources. Here is the full answer:
Hoffmann's Sign
Definition
Hoffmann's sign is a pathological upper limb reflex indicating corticospinal tract (upper motor neuron / UMN) dysfunction. It is the upper extremity analogue of the Babinski sign in the lower limb.
Named after Johann Hoffmann (German neurologist, 1857-1919), though the sign was likely first described by his student van Norden.
How to Elicit
Position: Patient relaxed, hand pronated, fingers slightly flexed (not tense). The examiner supports the patient's middle finger.
Technique:
- Hold the patient's middle finger (digit III) loosely between your index finger and thumb
- With your other thumb, sharply flick the distal phalanx of the middle finger downward (snap the nail downward - this is the classic Hoffmann method)
- Observe the thumb and index finger
Positive response: Involuntary flexion + adduction of the thumb AND flexion of the index finger (a pincer-like twitch)
- Bailey & Love's Short Practice of Surgery, 28th Ed.: "Forced flexion of the distal phalanx of the middle finger results in flexion of the thumb and index finger"
- Firestein & Kelley's Textbook of Rheumatology: "Holding the middle finger extended and suddenly extending the distal interphalangeal joint, resulting in flexion of the index finger and thumb"
- Sabiston Textbook of Surgery: "Elicited by flipping the fingernail of the middle finger, resulting in an involuntary flexion of the interphalangeal joint of the index finger and thumb"
Mechanism
The sign reflects hyperreflexia of the flexor digitorum superficialis/profundus and flexor pollicis longus due to release from normal corticospinal inhibition. When the middle finger's flexor tendons are suddenly stretched by the flick, the disinhibited spinal stretch reflex causes overflow contraction in the thumb and index finger flexors.
In normal subjects, the corticospinal tract modulates and suppresses this overflow. When the tract is damaged or its inhibitory influence is reduced, the reflex spreads - producing the positive sign.
- Adams & Victor's Principles of Neurology, 12th Ed.: "Other manifestations of the hyperreflexic state are the Hoffmann sign and the crossed adductor reflex of the thigh muscles."
Variants: Hoffmann vs. Trömner
| Sign | Stimulus | Response |
|---|---|---|
| Hoffmann's | Downward flick of middle finger distal phalanx (nail flick) | Thumb + index flex |
| Trömner's | Upward tap/flick of the palmar aspect of middle finger distal phalanx | Same: thumb + index flex |
Both test the same reflex arc; Trömner is considered slightly more sensitive by some authors. They are often grouped together.
Clinical Significance
1. Upper Motor Neuron (UMN) Lesion
A positive Hoffmann's sign = corticospinal pathway dysfunction. It is listed alongside the Babinski sign as a cardinal pathological reflex:
- Bradley & Daroff's Neurology in Clinical Practice: Box of UMN signs includes: "Pathological reflexes (Babinski, Hoffmann sign, loss of abdominal reflexes)"
- Neuroanatomy through Clinical Cases, 3rd Ed.: "Increased tone, spastic gait, and hyperreflexia including Babinski's sign, Hoffmann's sign, and jaw jerk reflex are upper motor neuron signs."
2. Cervical Myelopathy (Most Common Clinical Context)
Hoffmann's sign is a key screening test for cervical spondylotic myelopathy (CSM) - compression of the cervical spinal cord:
- Miller's Review of Orthopaedics, 9th Ed.: UMN findings in myelopathy include "Hyperreflexia, Hoffmann sign, clonus, or Babinski sign" alongside the finger escape sign, myelopathy hand, and inverted radial reflex
- Firestein & Kelley's Rheumatology: "Provocative tests helpful in diagnosing myelopathy include the presence of Hoffmann's sign, the finger escape sign, the abnormal grip-release test, and Lhermitte's sign"
3. Common Causes of a Positive Sign
| Category | Examples |
|---|---|
| Cervical cord compression | Cervical spondylotic myelopathy, disc herniation, ossification of posterior longitudinal ligament (OPLL) |
| Demyelinating disease | Multiple sclerosis |
| Motor neuron disease | ALS (corticospinal involvement) |
| Spinal cord tumors | Intramedullary/extramedullary |
| Cervical spine instability | e.g., rheumatoid atlantoaxial subluxation |
| Syringomyelia | |
| Trauma | Cervical cord injury |
Diagnostic Performance and Caveats
| Parameter | Value |
|---|---|
| Sensitivity | ~8-59% (variable, often low) |
| Specificity | ~49-85% |
| Population prevalence of false-positive | ~2-3% |
Important caveats:
- Can be bilaterally positive in normal anxious or hyper-reflexic individuals - a unilateral positive sign is far more significant than bilateral
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry: "An upper extremity sign of pyramidal dysfunction though sometimes present bilaterally in normal subjects"
- Asymmetry is the most clinically meaningful finding
- A positive sign in isolation, without other UMN features, should be interpreted cautiously
- Sensitivity is low - a negative sign does not rule out myelopathy; must be interpreted alongside Babinski, clonus, hyperreflexia, and clinical history
Associated UMN Signs to Test Alongside
| Sign | Test | Positive Response |
|---|---|---|
| Babinski | Stroke lateral sole | Upgoing great toe |
| Clonus | Dorsiflexion of ankle | Rhythmic oscillations |
| Finger escape sign | Hold fingers adducted/extended | Ulnar 2 fingers drift into flexion/abduction |
| Grip-release test | Rapid fist open-close | Cannot perform >20/10 sec (myelopathy) |
| Lhermitte's sign | Neck flexion | Electric shocks down spine/limbs |
| Inverted radial reflex | Tap brachioradialis | Finger flexion instead of elbow flexion (C5/C6 myelopathy) |
Sources: Adams & Victor's Principles of Neurology (12th Ed.) | Bradley & Daroff's Neurology in Clinical Practice | Firestein & Kelley's Textbook of Rheumatology | Miller's Review of Orthopaedics (9th Ed.) | Bailey & Love's (28th Ed.) | Neuroanatomy through Clinical Cases (3rd Ed.) | Kaplan & Sadock's Comprehensive Textbook of Psychiatry
This is a shared conversation. Sign in to Orris to start your own chat.