dermatoglyphics AND physiotherapy fingerprint patterns AND neuromuscular disorder dermal ridge count AND cerebral palsy palmar crease AND motor development
dermatoglyphics neuromuscular disorder physiotherapy
dermal ridge count cerebral palsy
dermatoglyphics cerebral palsy
dermatoglyphics neurodevelopmental disorders fingerprint
dermatoglyphics physical rehabilitation motor function
PMID: 31708622
dermatoglyphics Down syndrome trisomy palmar crease
dermatoglyphics physiotherapy neuromuscular disorders clinical significance fingerprint patterns
dermatoglyphics genetic marker neurodevelopment prenatal
Dermatoglyphics: Clinical Relevance to Physiotherapy and Neuromuscular Disorders
1. What Are Dermatoglyphics?
"The epidermal ridges that produce typical patterns on the surface of the fingertips, palms of the hand, and soles of the feet are genetically determined... In children with chromosomal abnormalities, the epidermal pattern on the hand and fingers is sometimes used as a diagnostic tool." — Langman's Medical Embryology
| Pattern | Characteristics |
|---|---|
| Loop | Most common (~65%); ridge enters and exits from same side |
| Whorl | Concentric rings; second most common (~30%) |
| Arch | Simplest pattern; ridges enter one side and exit the other (~5%) |
- Total Ridge Count (TRC): Sum of ridges counted at all 10 fingers
- atd angle: The angle formed by triradii at the base of digits 2 and 4 and the hypothenar region; elevated in trisomy conditions
- a-b Ridge Count (ABRC): Count between the thenar and first interdigital triradii on the palm
- Pattern Intensity Index (PII): Based on loop/whorl/arch distribution
2. Dermatoglyphics & Chromosomal/Neurodevelopmental Conditions
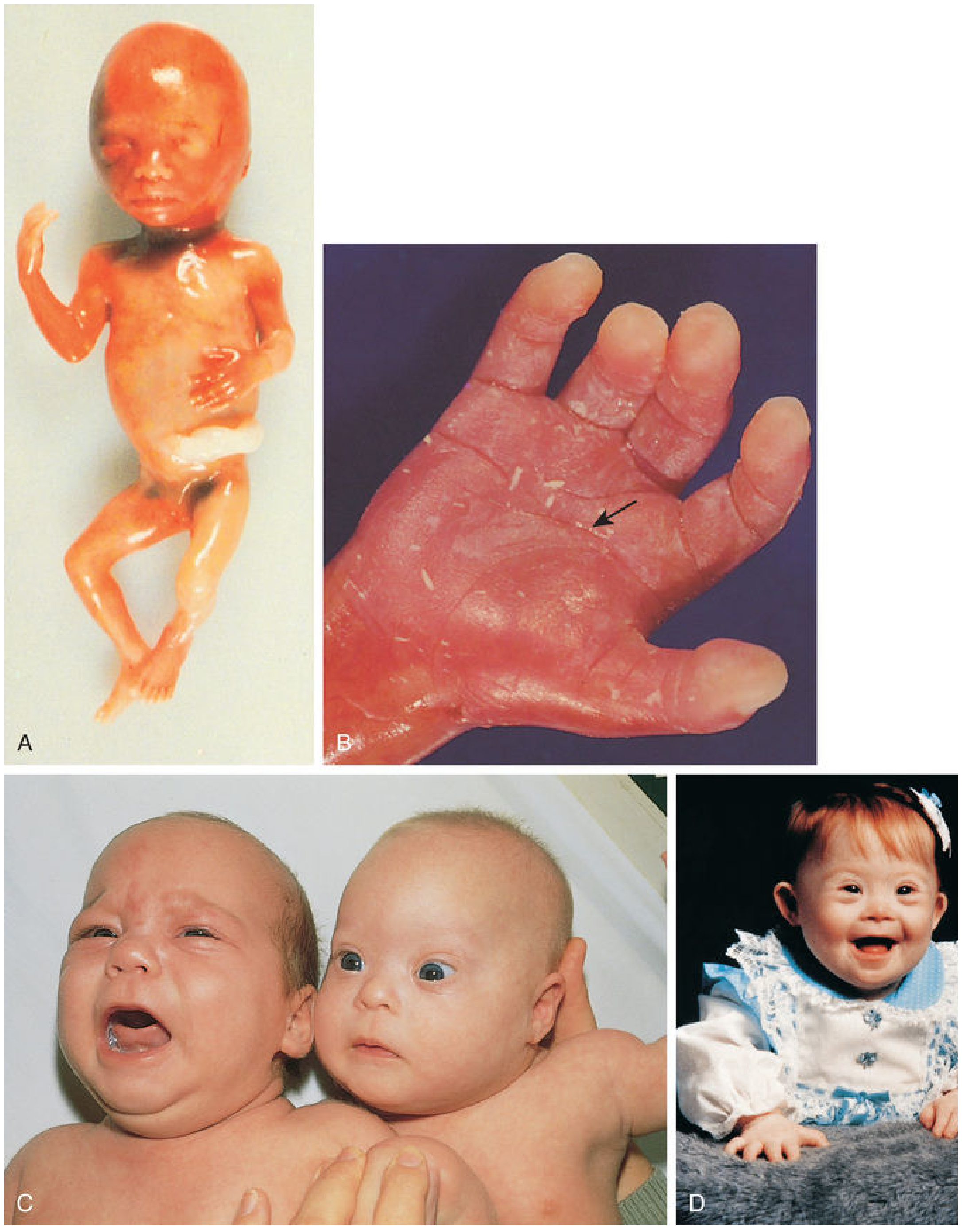
Down Syndrome (Trisomy 21)
"The hands are broad, with a single transverse (simian) palmar crease and other characteristic dermal markings." — Adams and Victor's Principles of Neurology, 12th Ed.
- Single transverse (simian) palmar crease — due to hypotonia during fetal development
- Clinodactyly of the 5th digit
- Increased ulnar loops on fingertips
- Elevated atd angle (>57°)
- Decreased TRC relative to controls
- Profound hypotonia is the primary motor challenge; early physiotherapy (neurodevelopmental therapy, aquatic therapy) addresses delayed motor milestones — most children with Down syndrome do not walk until 3–4 years of age
- The simian crease itself is a passive clinical marker; its presence should prompt the physiotherapist to screen for associated hypermobility, atlantoaxial instability, and cardiac defects before designing an exercise programme
3. Dermal Ridge Count & Cerebral Palsy
Somani R et al. (2019) studied 150 children (6–12 years) in three groups: CP caries-active, healthy caries-active, and healthy caries-free. Using the Cummins and Midlo method for fingerprint analysis, they found:
- CP children showed predominance of whorl patterns
- Healthy caries-free children showed more arch patterns
- The association between dermatoglyphic pattern and disease group was statistically significant
- Conclusion: Dermatoglyphics can serve as a noninvasive, economical preliminary tool for identifying genetic predisposition in CP
- CP arises from a non-progressive injury to the developing brain, typically between 24–34 weeks gestation — the same window when ridge formation is being completed
- Hypoxic-ischemic events, periventricular leukomalacia, or intrauterine infections during this period could theoretically disturb the signalling gradients (Wnt, BMP, EDA pathways) that simultaneously pattern both ridges and cortical cytoarchitecture
- This explains why atypical ridge patterns (fewer arches, altered TRC, abnormal atd angles) are observed in some children with spastic diplegia
4. Fingerprint Patterns & Neuromuscular Disorders — Broader Evidence
Neurodevelopmental Disorders (Systematic Evidence)
- Dermatoglyphic asymmetry, reduced TRC, altered pattern distribution, and abnormal palmar crease patterns reflect disrupted neurodevelopment during the second trimester
- These findings appear across schizophrenia, bipolar disorder, and attention-deficit disorders, consistent with a shared ectodermal disruption hypothesis
Conditions With Absent/Hypoplastic Dermatoglyphics
5. Palmar Crease & Motor Development — Clinical Synthesis
| Finding | Association | Physiotherapy Implication |
|---|---|---|
| STPC + hypotonia | Down syndrome, trisomy 18 | Screen for atlantoaxial instability; gentle proprioceptive input; hydrotherapy |
| STPC + spasticity | Some CP cases | Botulinum toxin + task-oriented therapy; hand splinting to prevent contracture |
| STPC + joint laxity | Connective tissue disorders | Stability exercises, orthotics, proprioceptive training |
| STPC + isolated finding | ~4% normals | No physiotherapy action required alone |
| Bilateral STPC | Stronger genetic association | Warrants chromosomal workup before intensive exercise |
6. The Dermatoglyphics–Physiotherapy Interface: Practical Framework
Dermatoglyphic Anomaly Detected
│
▼
Is it isolated?──Yes──► Low risk; routine developmental surveillance
│
No
│
▼
Associated features?
(hypotonia, delay, dysmorphism, spasticity)
│
▼
┌─────────────────────────────────────────────┐
│ Refer: genetics + physiotherapy assessment │
│ • Gross motor: GMFCS / GMFM scoring │
│ • Fine motor: Peabody / PDMS-2 │
│ • Tone assessment: Ashworth / Tardieu │
└─────────────────────────────────────────────┘
│
▼
Tailor PT Programme:
- Hypotonic CP/DS → NDT, aquatic therapy, orthotics
- Spastic CP → stretching, serial casting, FES
- Dyskinetic CP → rhythmic auditory stimulation, CIMT
Key Takeaways
- Dermatoglyphics are permanent fetal records — formed during the same embryological window as the brain's key organizational phases (weeks 10–24)
- The simian crease is the most clinically visible palmar dermatoglyphic anomaly, strongly associated with Down syndrome, trisomy 18, and some cases of CP; it arises from hypotonia-driven fetal fisting
- Total Ridge Count and pattern distribution (increased whorls, decreased arches) have been documented in CP and other neurodevelopmental conditions, supporting their use as noninvasive biomarkers
- For physiotherapists, dermatoglyphic anomalies are not therapeutic targets but serve as clinical flags — their presence should prompt comprehensive developmental screening, GMFCS classification, and early referral for structured intervention
- Absent dermatoglyphics in genodermatoses (NFI, Kindler EB) require adapted physiotherapy approaches due to skin fragility and thermal regulation impairment
- The evidence base is growing but largely observational; no RCTs yet link dermatoglyphic profiling to physiotherapy outcome prediction
- Langman's Medical Embryology — Fingerprints section
- The Developing Human: Clinically Oriented Embryology — Trisomy 21 and palmar crease
- Adams and Victor's Principles of Neurology, 12th Ed. — Down Syndrome
- Swanson's Family Medicine Review — Clinical case on simian crease
- The Harriet Lane Handbook, 23rd Ed. — Cerebral palsy motor development
- Somani R et al. Dermatoglyphics as a Noninvasive Tool for Predicting Dental Caries in Cerebral Palsy. Int J Clin Pediatr Dent 2019 [PMID: 31708622]
- Berecz H et al. Minor physical anomalies and dermatoglyphic signs in affective disorders: A systematic review. Psychiatr Hung 2017 [PMID: 28424384]
- Kyselicová K et al. Fingerprint patterns in altered neurodevelopment in autism spectrum disorder. Dev Psychobiol 2023 [PMID: 38010306]
What new research can be done in physiotherapy in relevance to this
dermatoglyphics motor outcome prediction rehabilitation
dermatoglyphics cerebral palsy spasticity gross motor
fingerprint biomarker neurodevelopmental early intervention
dermatoglyphics congenital disorders screening
dermatoglyphics sport physical performance athletic
dermatoglyphics Down syndrome autism motor skills
PMID: 32126478
PMID: 32196525
dermatoglyphics spastic diplegia GMFCS functional assessment
Research Proposals: Dermatoglyphics × Physiotherapy
THEME 1 — Dermatoglyphics as a Triage/Screening Tool in Paediatric PT
Study Idea 1.1
- Enrol neonates (0–1 month) referred to NICU or neonatology
- Collect dermatoglyphic data at birth (inkless wipe method or optical scanning)
- Classify anomalies: STPC, elevated atd angle (>57°), reduced TRC, increased whorl density
- Follow-up at 3, 6, 9, 12, 18, 24 months with GMFM-88, Bayley Scales, and GMFCS classification
- Primary outcome: Does the number or type of dermatoglyphic anomalies at birth independently predict GMFCS level at 24 months?
Study Idea 1.2
- Cross-sectional study; 100 children (ages 2–12) referred to a paediatric PT clinic
- Measure FAABRC (fluctuating asymmetry of a-b ridge count) and bilateral atd angle asymmetry
- Correlate with: GMFCS level, Peabody Developmental Motor Scales (PDMS-2), Bruininks-Oseretsky Test of Motor Proficiency (BOT-2)
- Sub-group analysis: CP vs. non-CP vs. neuromuscular disease vs. orthopaedic conditions
THEME 2 — Dermatoglyphics as a Prognostic Stratifier in Cerebral Palsy PT
Study Idea 2.1
- 80 children with spastic CP (4–12 years, GMFCS I–III)
- Pre-treatment: classify fingerprint pattern (whorl-dominant vs. loop-dominant), measure TRC, ABRC, atd angle
- All children receive standardised 12-week intensive physiotherapy (NDT + task-oriented training)
- Outcome measures at 0, 6, 12 weeks: GMFM-66, Modified Ashworth Scale, 10-metre walk test, Box and Block Test (for fine motor)
- Analysis: Does dermatoglyphic subgroup (whorl-dominant vs. loop-dominant) predict rate of improvement on GMFM-66?
Study Idea 2.2
- Assess bilateral palmar crease morphology in 60 children with hemiplegic CP
- Categorise: unilateral STPC (affected side), bilateral STPC, normal bilateral crease
- All children undergo 60-hour HABIT protocol
- Outcome: Melbourne Assessment 2, Assisting Hand Assessment (AHA), grip strength dynamometry
- Test whether STPC on the hemiplegic side correlates with severity of fine motor impairment and response to HABIT
THEME 3 — Dermatoglyphics in Stroke & Acquired Neurology
Study Idea 3.1
- Enrol 100 first-ever ischaemic stroke patients within 72 hours
- Record TRC, fingerprint pattern, atd angle at baseline
- Standardised upper limb PT (45 min/day × 6 weeks)
- Outcomes at 4 and 12 weeks: Fugl-Meyer Assessment (UL), Action Research Arm Test, grip dynamometry
- Covariates: stroke volume, lesion location, age, NIHSS
- Test: Does TRC independently predict Fugl-Meyer gain score at 12 weeks?
Study Idea 3.2
- 70 patients with PD (Hoehn and Yahr I–III)
- Measure FAABRC and pattern asymmetry
- 8-week structured physiotherapy (balance, treadmill, resistance training)
- Outcomes: Berg Balance Scale, Timed Up and Go, MDS-UPDRS III, Parkinson's Disease Questionnaire-39 (PDQ-39)
- Correlate FA with outcome improvement
THEME 4 — Dermatoglyphics × Sports Physiotherapy & Talent Identification
Study Idea 4.1
- 150 elite athletes (3 sports: sprinting, swimming, team sport)
- Fingerprint classification + TRC + atd angle
- Neuromuscular performance battery: isokinetic dynamometry, reactive strength index, star excursion balance test, Y-balance test
- Follow longitudinally for 12 months to record musculoskeletal injury incidence and return-to-play duration
- Test: Do specific dermatoglyphic profiles predict injury risk or differential recovery trajectory?
Study Idea 4.2
- Cross-sectional study at 6-month post-ACL reconstruction
- Fingerprint profiling + bilateral isokinetic quad/hamstring ratio
- Outcome: limb symmetry index, re-injury rate at 12 months
- Hypothesis: Dermatoglyphic FA predicts greater neuromuscular asymmetry post-ACLR
THEME 5 — Fetal Alcohol Spectrum Disorder (FASD) and Physiotherapy
Study Idea 5.1
- Screen all children aged 4–10 referred to PT for coordination disorder or unexplained motor delay (DCD criteria)
- Apply rapid dermatoglyphic screening (inkless optical scan): TABRC, FAABRC, atd angle
- Children flagged by dermatoglyphic algorithm referred for formal FASD assessment (paediatrician + neuropsychology)
- Validate the screening algorithm's sensitivity/specificity for FASD
- Compare PT outcomes (MABC-2, DCDQ) in FASD-confirmed vs. non-FASD groups
THEME 6 — Methodological Research
Study Idea 6.1
Summary: Research Priority Matrix
| Study | Condition | Design | Feasibility | Novelty | Impact |
|---|---|---|---|---|---|
| 1.1 Neonatal predictor study | General motor delay | Prospective cohort | Medium | ★★★★★ | High |
| 1.2 FA in PT-referred children | Mixed | Cross-sectional | High | ★★★★ | High |
| 2.1 CP fingerprint × PT response | Cerebral palsy | Longitudinal | Medium | ★★★★★ | Very High |
| 2.2 STPC × HABIT outcomes | Hemiplegic CP | RCT sub-study | High | ★★★★ | High |
| 3.1 Stroke TRC × motor recovery | Stroke | Prospective observational | Medium | ★★★★★ | Very High |
| 3.2 PD + FA + rehab | Parkinson's | Observational | Medium | ★★★★ | Medium |
| 4.1 Athletes + injury | Sports | Longitudinal | High | ★★★ | Medium |
| 5.1 FASD screening via PT | FASD/DCD | Diagnostic accuracy | High | ★★★★★ | Very High |
| 6.1 Digital scanning validity | All | Methodological | Very High | ★★★ | Enabling |
The Single Most Original & Impactful Study
- CP physiotherapy is intensive and expensive; knowing in advance who will respond well has enormous resource implications
- The dermatoglyphic-CP link already has a biological basis (shared second-trimester developmental window)
- The methodology is fully developed (validated PT outcome tools + established dermatoglyphic measurement techniques)
- It is entirely unstudied, meaning any positive finding would be a landmark publication
- Andreu-Fernández V et al. Dermatoglyphic FA and TABRC as biomarkers of FASD. Early Hum Dev. 2020 [PMID: 32126478]
- Neiswanger K et al. Fingerprint asymmetry in orofacial clefts. PLoS One. 2020 [PMID: 32196525]
- Somani R et al. Dermatoglyphics in cerebral palsy children. Int J Clin Pediatr Dent. 2019 [PMID: 31708622]
- Berecz H et al. Dermatoglyphic signs in neurodevelopmental disorders. Psychiatr Hung. 2017 [PMID: 28424384]
- Kyselicová K et al. Fingerprints in autism spectrum disorder. Dev Psychobiol. 2023 [PMID: 38010306]
Dermatoglyphics as a Prognostic Stratifier in Cerebral Palsy PT