Abnormal uterine bleeding
Reading File
Finding Sources
Searching PubMed
"abnormal uterine bleeding" management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Abnormal Uterine Bleeding (AUB)
Definition
AUB describes any irregularity in the menstrual cycle involving frequency, cyclicity, duration, or volume of flow outside of pregnancy. The term has replaced the older, imprecise labels "dysfunctional uterine bleeding," "menorrhagia," and "menometrorrhagia" - those terms are now obsolete.
Normal menstrual parameters:
- Cycle length: 21-35 days
- Duration of flow: 4-8 days
- Blood loss: up to 80 mL per cycle (>80 mL = abnormal)
- Intermenstrual bleeding = always abnormal
Up to one-third of women between menarche and menopause experience AUB at some point, making it one of the most common gynecological complaints.
Normal Menstrual Cycle - Key Physiology
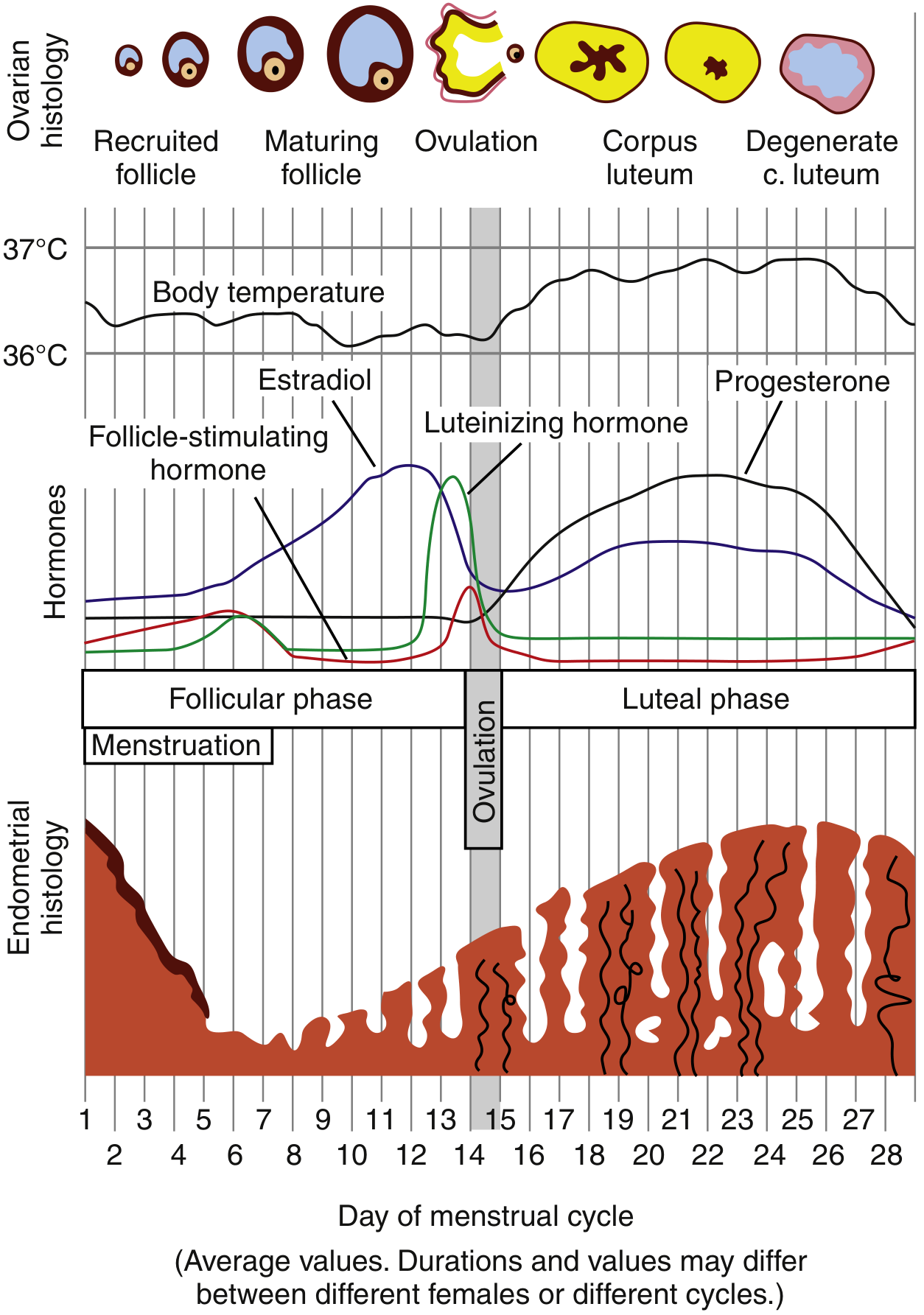
The cycle depends on the coordinated interplay of the hypothalamic-pituitary-ovarian axis. Estrogen drives follicular-phase endometrial proliferation; post-ovulation progesterone from the corpus luteum matures the lining. When the corpus luteum degenerates (no implantation), the sharp drop in progesterone and estrogen triggers predictable menstruation. Disruption at any point along this axis causes AUB.
PALM-COEIN Classification (FIGO 2011)
Established by the FIGO Working Group on Menstrual Disorders and endorsed by ACOG, this system divides causes into structural and nonstructural:
PALM - Structural Causes
(diagnosed by imaging or histology)
| Abbreviation | Condition | Key Features |
|---|---|---|
| AUB-P | Polyp | Endometrial glands/stroma overgrowth; benign in ~95%; associated with tamoxifen, obesity, PCOS |
| AUB-A | Adenomyosis | Endometrial glands within myometrium; causes heavy, painful periods |
| AUB-L | Leiomyoma (Fibroids) | Most common benign gynecologic tumor; up to 70% of women by age 50; 2-3x higher incidence in Black women; submucosal type (projects into cavity) causes the worst bleeding |
| AUB-M | Malignancy & Hyperplasia | Endometrial cancer in 90% of cases presents with AUB; must be excluded in high-risk patients |
COEIN - Nonstructural Causes
(medical/hormonal diagnoses)
| Abbreviation | Condition | Key Features |
|---|---|---|
| AUB-C | Coagulopathy | Up to 20% of heavy menstrual bleeding; von Willebrand disease most common (up to 13% of AUB cases), often first presenting with heavy bleeding at menarche |
| AUB-O | Ovulatory Dysfunction | ~50% of AUB cases; most commonly PCOS; also hyperprolactinemia, hypothyroidism, hypothalamic dysfunction (anorexia), perimenopause |
| AUB-E | Endometrial | Primary disorders of endometrial hemostasis; regular cycle but heavy bleeding |
| AUB-I | Iatrogenic | Oral contraceptives, anticoagulants, hormone therapy, tamoxifen, prior cesarean scar |
| AUB-N | Not yet classified | No identifiable etiology |
Pathophysiology of Anovulatory Bleeding
This is the most frequent mechanism (~75% of functional AUB). Without ovulation, there is no corpus luteum and no progesterone. Estrogen stimulates the endometrium unopposed - it proliferates, becomes thick and fragile, then sheds irregularly and unpredictably. This pattern tends to produce infrequent but heavy, unpredictable bleeding, in contrast to organic structural lesions, which often cause more frequent bleeding.
Epidemiology by Age Group
| Age Group | Common Causes |
|---|---|
| Adolescents (~20% of AUB) | Immaturity of hypothalamic-pituitary-ovarian axis; undiagnosed coagulopathy (vWD); PCOS; infection |
| Reproductive age | PCOS, fibroids, polyps, endometrial hyperplasia, iatrogenic |
| Perimenopause (~50% of AUB) | Incipient ovarian failure, anovulation, fibroids, hyperplasia |
| Postmenopause | Atrophy (most common); polyps; fibroids; hormone therapy; endometrial cancer (90% of endometrial cancers present with AUB) |
Associated Systemic Conditions
AUB may be a presenting manifestation of:
- Endocrine: hypothyroidism/hyperthyroidism, PCOS, hyperprolactinemia, diabetes mellitus, Cushing syndrome, Addison disease
- Hematologic: vWD, ITP, leukemia
- Hepatic/Renal disease (impaired factor clearance/production)
- Medications: anticoagulants, antipsychotics (raise prolactin), tamoxifen
Diagnosis
History
- Pattern of bleeding: frequency, duration, volume (number of pads/tampons, clots)
- Relationship to menstrual cycle
- Age at menarche; reproductive history
- Family history of bleeding disorders
- Medications; prior uterine surgery (cesarean)
- Symptoms of PCOS, thyroid disease, systemic illness
- Post-coital bleeding (suggests cervical pathology)
Physical Examination
- Hemodynamic status (BP, HR - assess for acute blood loss)
- Signs of PCOS: obesity, acne, hirsutism, acanthosis nigricans
- Thyroid palpation
- Skin: petechiae, ecchymoses (coagulopathy)
- Speculum exam: cervical/vaginal lesions
- Bimanual exam: uterine size, fibroid uterus, adnexal mass
Laboratory Workup
| Test | Indication |
|---|---|
| Urine/serum pregnancy test | All reproductive-age women - always first |
| CBC + platelets | All patients; assess anemia severity |
| TSH | Routine screen for thyroid dysfunction |
| Coagulation studies (PT, PTT, vWF screen) | Heavy bleeding since menarche; family history; bruising/epistaxis |
| Prolactin, FSH | Suspected ovulatory dysfunction |
| Fasting glucose / lipids | Suspected PCOS / metabolic syndrome |
| STI screen (Chlamydia) | At-risk patients |
Imaging
- Transvaginal ultrasound (TVUS) - first-line imaging; identifies fibroids, polyps (with Doppler), endometrial thickening
- Postmenopause: endometrial thickness ≤4 mm reliably excludes cancer (though this cutoff may under-diagnose endometrial cancer in Black patients - recent data highlight this disparity)
- Thickness >4 mm in postmenopausal women requires biopsy
Endometrial Biopsy Indications
- All women ≥45 years with AUB (including intermenstrual bleeding)
- Women <45 years with: prolonged unopposed estrogen exposure, obesity, persistent/refractory AUB, or elevated familial cancer risk
- Any postmenopausal bleeding with endometrial thickness >4 mm or focal lesion on imaging
Hysteroscopy
Diagnostic hysteroscopy is indicated for unexplained AUB (premenopausal or postmenopausal), abnormal TVUS findings, and selected infertility evaluations - it allows direct visualization and concurrent treatment (polypectomy, resection of submucosal fibroids).
Management
Acute / Emergent Bleeding (Hemodynamically Unstable)
- IV resuscitation (fluids + blood products)
- Conjugated equine estrogen IV: 25 mg every 4-6 hours (up to 3 doses) until bleeding stops
- Intrauterine tamponade (26-Fr Foley with 30 mL saline) as temporizing measure
- Surgical options: urgent dilation & curettage (D&C), uterine artery embolization, endometrial ablation, or hysterectomy
Medical Treatment (Non-Emergent)
| Agent | Use Case | Mechanism |
|---|---|---|
| Combined oral contraceptives (COCs) | Anovulatory bleeding, ovulatory heavy bleeding | Restores estrogen/progesterone balance; regulates cycle |
| Progestins (medroxyprogesterone 5-10 mg x 10 days; norethindrone 5 mg daily) | Anovulatory bleeding; when estrogen is contraindicated | Opposes estrogen-driven proliferation |
| Levonorgestrel IUD (LNG-IUD) | Ovulatory heavy bleeding, fibroids, adenomyosis | Local progestin - most effective long-term option for reducing heavy menstrual bleeding |
| Tranexamic acid | Ovulatory heavy bleeding | Antifibrinolytic; shown more effective than NSAIDs, less effective than LNG-IUD |
| NSAIDs | Ovulatory heavy bleeding, dysmenorrhea | Reduce prostaglandins; reduce blood loss ~25-30%; less effective than tranexamic acid or LNG-IUD |
| GnRH agonists (elagolix 300 mg BID, relugolix 40 mg daily) | Symptomatic fibroids | Reduce estrogen; used pre-surgically or as medical alternative |
Profuse anovulatory bleeding - oral protocol: One combination OCP every 6 hours for 5-7 days; bleeding typically stops within 24 hours. Heavy withdrawal bleed expected 2-4 days after stopping.
Surgical Treatment
| Procedure | Indication |
|---|---|
| Hysteroscopic polypectomy | Endometrial/cervical polyps |
| Myomectomy | Symptomatic fibroids in women desiring fertility preservation |
| Endometrial ablation | Medical treatment failure; not 100% effective (~29% require hysterectomy within 5 years in trials) |
| Uterine artery embolization (UAE) | Fibroids; ~31% ultimately require hysterectomy in randomized trials |
| Hysterectomy | Definitive; reserved for failure of medical therapy, confirmed malignancy, or patient preference |
Note: Endometrial sampling should always be performed before hysterectomy. D&C alone is not an effective treatment for AUB and is not required before hysterectomy.
Postmenopausal Bleeding - Special Considerations
Any bleeding ≥12 months after cessation of menses is abnormal and must be fully evaluated. The most common cause is endometrial atrophy (thinning of the lining due to estrogen deficiency), but 90% of endometrial cancers present with postmenopausal bleeding. Other causes include polyps, fibroids, adenomyosis, and anticoagulant/hormone therapy use.
Prognosis
The prognosis depends entirely on the underlying cause. The vast majority of functional (anovulatory) AUB resolves with appropriate medical management. Cases due to malignancy require prompt surgical and oncologic management.
Sources:
- Rosen's Emergency Medicine, Ch. 86
- Goldman-Cecil Medicine (International Edition), Ch. 220
- Sabiston Textbook of Surgery, Ch. 120
- Berek & Novak's Gynecology, Ch. 26
- Harrison's Principles of Internal Medicine 22E, Ch. 405
Recent evidence note: A 2025 systematic review (PMID 39617186) on etiology and diagnosis of heavy menstrual bleeding found coagulopathies (especially vWD) are prevalent and often underdiagnosed. A 2026 meta-analysis (PMID 41791665) found a significant rate of AUB in women on anticoagulation for VTE - an important iatrogenic cause to recognize.
This is a shared conversation. Sign in to Orris to start your own chat.