MANGEMENT OF HIRRANDENTIS SUUPRATIVA AS PER STANDARD BOOK AND PROTOCOL
"hidradenitis suppurativa" AND management
Hidradenitis Suppurativa (HS) - Management
Definition & Overview
- Prevalence: ~0.1% in the United States
- Disproportionately affects women, African Americans, and those aged 18-29 years
- Not seen before puberty; rarely presents after the 4th decade
- Anogenital disease is more common in men
Pathogenesis
- Terminal follicle hyperkeratosis leads to follicular occlusion
- Rupture of follicular epithelium releases keratin, sebum, bacteria, and hairs into the dermis
- Inflammatory cascade results in abscess formation
- Gland rupture leads to bacterial proliferation and spread into subcutaneous soft tissue
- Secondary infection causes sinus tract formation, bridged scarring, and multiple communicating subcutaneous sinuses
| Gene | Protein Product | Role in HS |
|---|---|---|
| NCSTN | Nicastrin (γ-secretase complex) | Follicular keratinocyte differentiation |
| PSENEN | Presenilin enhancer-2 | γ-secretase complex function |
| PSEN1 | Presenilin 1 | γ-secretase complex function |
| TNF | Tumor necrosis factor | Promotion of inflammation |
| IL12Rβ1 | IL-12 and IL-23 receptor subunit | T-cell subset differentiation |
Hurley Staging System
| Stage | Description |
|---|---|
| I | Single or multiple abscesses without sinus tracts or scarring |
| II | Recurrent abscesses with sinus tract formation and scarring; single or multiple widely separated lesions |
| III | Diffuse or near-diffuse involvement, or multiple interconnected sinus tracts and abscesses across an entire area |
Treatment Algorithm (Fitzpatrick's / European Guidelines)
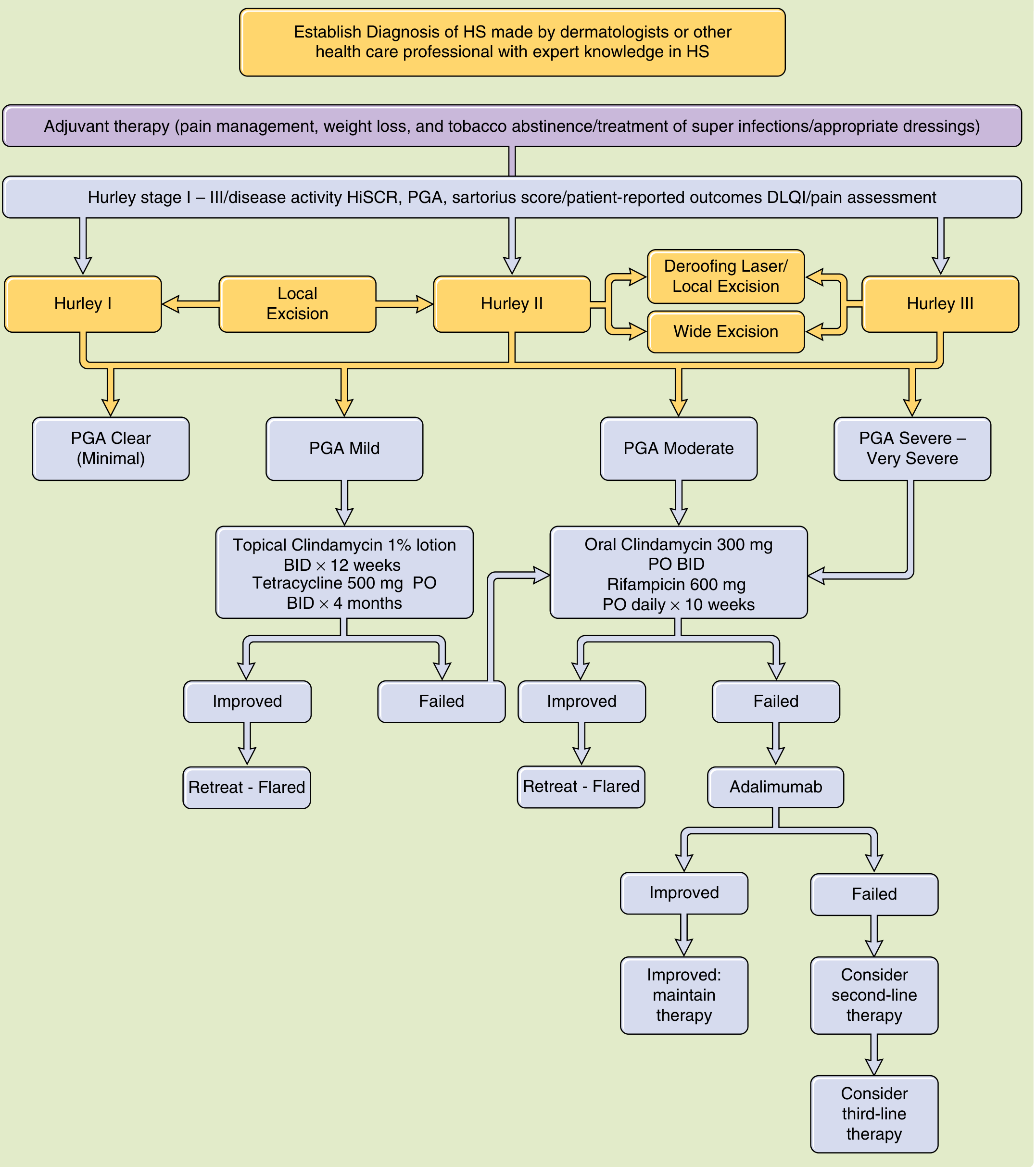
General / Adjuvant Measures (All Stages)
- Daily cleansing with chlorhexidine gluconate (Hibiclens) or benzoyl peroxide wash
- Weight loss (obesity is a common association)
- Smoking cessation (strong trigger)
- Wear loose-fitting clothing to reduce friction
- Heat avoidance
- Topical aluminum chloride or botulinum toxin A injections to reduce sweating
- Laser hair removal in unaffected sites as preventive therapy
- Identify and treat comorbidities (metabolic syndrome, PCOS, inflammatory bowel disease)
- Pain management is a key adjuvant concern
Medical Management
Hurley Stage I (Mild Disease)
- Topical clindamycin 1% lotion BID x 12 weeks - RCT-proven reduction of pustules, inflammatory nodules, and abscesses
- Oral tetracyclines (tetracycline 500 mg PO BID x 4 months) - used for their anti-inflammatory effect in any stage
- Intralesional corticosteroid injection - especially for early lesions, may be combined with topical clindamycin or oral doxycycline/minocycline
- Topical metronidazole 0.75%
- Topical erythromycin 2%
Hurley Stage II (Moderate Disease)
- Clindamycin 300 mg PO BID + Rifampicin 600 mg PO daily x 10 weeks - extensively studied, quite effective
- Rifampicin 10 mg/kg/day + Moxifloxacin 400 mg/day + Metronidazole 500 mg TID
Hurley Stage III / Biologic-Refractory Disease
| Agent | Mechanism | Dosing |
|---|---|---|
| Adalimumab (FDA-approved) | Anti-TNF-α monoclonal antibody | 160 mg SC at week 0, 80 mg at week 2, then 40 mg weekly |
| Infliximab | Chimeric anti-TNF-α | 5 mg/kg at weeks 0, 2, 6, then every 8 weeks |
| Secukinumab | Anti-IL-17A | Per protocol |
| Anakinra | IL-1 receptor antagonist | Case reports of efficacy |
| Ustekinumab | Anti-IL-12/23 | Case reports |
Second-Line / Adjuvant Medical Options
- Spironolactone 100-150 mg daily - for women (anti-androgen effect)
- Finasteride 5 mg daily - for men or postmenopausal women
- Oral contraceptives (OCs) - helpful in women as adjuvants
- Metformin 500-1500 mg daily - particularly for women with HS and PCOS/metabolic syndrome; improved clinical severity in 72% of patients in a small prospective study
- Isotretinoin: largely ineffective (only 16% response rate); still commonly prescribed - most useful in young women with mild-to-moderate disease
- Acitretin (0.25-0.88 mg/kg for 9-12 months): better evidence than isotretinoin
- Alitretinoin 10 mg daily x 24 weeks: 50% reduction in Sartorius score in 6/14 patients
Note: Incision and drainage is strongly discouraged as it does not address the underlying pathology and promotes recurrence.
Surgical Management
| Procedure | Indication | Recurrence Rate |
|---|---|---|
| Deroofing of sinus tracts | Hurley I-II; single tracts | ~27% |
| Local excision | Hurley I-II; limited disease | ~22% |
| Wide local excision | Hurley II-III; moderate-severe | ~13% overall |
| - Wide excision + graft closure | Severe with larger defects | ~6% |
| - Wide excision + flap closure | Severe with larger defects | ~8% |
| - Wide excision + primary closure | Standard closure | ~15% |
- Intraoperative color marking of sinus tracts improves completeness of excision
-
90% patient satisfaction after surgery
- Open areas may be left to heal by secondary intention or closed primarily
- Wide excision in the axillary and perianal areas has low recurrence; inguinal and submammary sites more often recur (excision of submammary HS is uncommonly recommended)
- CO2 laser may destroy lesions and sinus tracts as an alternative to cold-knife excision
Laser & Photodynamic Therapy
| Modality | Evidence |
|---|---|
| Nd:YAG laser | Prospective RCT (n=22): significant improvement after 3 monthly sessions |
| Photodynamic therapy (MAL or 5-ALA + blue/red light) | Mixed anecdotal reports; costly, painful, no remission - further studies required |
| CO2 laser | Useful to destroy lesions and sinus tracts |
| Laser hair removal | Preventive in unaffected sites |
Complications to Monitor
| Complication | Notes |
|---|---|
| Squamous cell carcinoma (SCC) | After average 19 years of active disease; manifests as ulceration/thickening in skin crease |
| Spondyloarthropathy | Rare |
| Pyoderma gangrenosum (PG) | Rapidly expanding, painful ulcer with undermined edges; median 19 years after HS onset |
| Urethral/vesical/rectal fistulas | Rare |
| Secondary amyloidosis | Rare |
| Lymphedema | Of penis and groin in long-standing/surgically-treated disease |
| Anemia and hypoproteinemia | Chronic disease |
| PASH syndrome | HS + acne conglobata + pyoderma gangrenosum |
Differential Diagnosis
- Furunculosis (early stages)
- Crohn's disease (especially perianal)
- Cryptoglandular fistula-in-ano
- Pilonidal sinus
- Tuberculosis
- Actinomycosis
- Lymphogranuloma venereum
- Granuloma inguinale
Summary: Stage-Based Treatment Ladder
STAGE I (Mild)
├── General measures (always)
├── Topical clindamycin 1% BID x 12 weeks
├── Oral tetracycline 500 mg BID x 4 months
├── Intralesional steroids for early lesions
└── Surgical: Local excision / deroofing
STAGE II (Moderate)
├── Clindamycin 300 mg + Rifampicin 600 mg PO daily x 10 weeks
├── Triple therapy (Rifampicin + Moxifloxacin + Metronidazole)
├── Hormonal therapy (spironolactone/finasteride)
├── Metformin (if PCOS/metabolic syndrome)
├── Adalimumab (if antibiotic-refractory)
└── Surgical: Deroofing, wide local excision
STAGE III (Severe)
├── Adalimumab 40 mg SC weekly (FDA-approved)
├── Infliximab 5 mg/kg at 0, 2, 6 weeks then q8 weeks
├── Other biologics (infliximab, secukinumab, ustekinumab)
├── IV ertapenem (bridging for severe flares)
└── Surgical: Wide excision with graft/flap closure
Recent Evidence Updates (2024-2026)
- Australasian HS management guidelines (2025) - PMID 39578415, Practice Guideline + Systematic Review
- North American clinical practice guidelines for special populations (2025) - PMID 39725212 - addresses pediatric, pregnant, and immunocompromised patients
- Italian Delphi consensus: Surgery + biologics integration (2024) - PMID 39004081
- A 2026 systematic review and network meta-analysis on biologics confirmed short-term efficacy of biologics in moderate-to-severe HS (PMID 41457056)
- Andrews' Diseases of the Skin - Clinical Dermatology, pp. 289-290
- Fitzpatrick's Dermatology, Vol. 1&2, pp. 1518-1520 (European/North American guidelines-based algorithm)
- Dermatology 2-Volume Set 5e (Hurley staging, pathogenesis, genetics)
- Bailey & Love's Short Practice of Surgery 28th Ed., pp. 1463 (surgical perspective)
- Sabiston Textbook of Surgery (perianal HS, Hurley-based treatment table)
DAPARYL L HAVE RISK OF UTI PREVALNCED IN MALE PATIENT ALONG WITH HOW TO PREVENT FURTHER RISK OF UTI FROM STANDARD SOURCES
"dapagliflozin" AND "urinary tract infection"
Dapagliflozin Daparly UTI risk male patients prevention guidelines 2024
PMID: 37010676
Dapagliflozin (Daparly-L) - UTI Risk in Male Patients & Prevention
What is Daparly-L?
- Type 2 Diabetes Mellitus (T2DM)
- Heart failure with reduced ejection fraction (HFrEF)
- Chronic kidney disease (CKD)
Mechanism of Action (Why UTI Risk Exists)
- Increased urinary glucose excretion (glucosuria) - up to 70 g glucose/day excreted in urine
- Osmotic diuresis and natriuresis
- Glucosuria creates a nutrient-rich environment in the urinary tract that promotes growth of uropathogens, particularly Escherichia coli and Klebsiella species
- Patients with T2DM already have baseline immune dysfunction and bladder abnormalities (diabetic cystopathy) - compounding the risk
UTI Risk with Dapagliflozin - Evidence Summary
Meta-Analysis Data (Best Available Evidence)
| Comparison | Odds Ratio (OR) | 95% CI | p-value |
|---|---|---|---|
| Dapagliflozin (all doses) vs. placebo/active | 1.17 | 1.04-1.31 | 0.006 |
| Dapagliflozin 10 mg/day > 24 weeks vs. placebo | 1.27 | 1.13-1.43 | <0.0001 |
| Dapagliflozin as add-on (combination) therapy | 1.27 | 1.09-1.48 | 0.008 |
| Dapagliflozin as monotherapy | 1.05 | 0.88-1.25 | NS |
Key finding: High-dose (10 mg), long-duration (>24 weeks), and combination therapy with dapagliflozin significantly increases UTI risk.
Dose-Response Relationship (Network Meta-Analysis, 2024):
- Dapagliflozin 10 mg carries 55% more risk of genital infections vs 2.5 mg (OR 1.55, 95% CI 1.08-2.23)
- Dapagliflozin 10 mg had significantly more UTIs vs. placebo (OR 1.28, 95% CI 1.06-1.54)
- Only dapagliflozin (not empagliflozin or canagliflozin) showed a clear dose-response relationship for UTI risk
UTI Risk in MALE Patients Specifically
Is the Risk Lower in Men?
| Aspect | Male Patients | Female Patients |
|---|---|---|
| Baseline UTI risk | Lower (longer urethra, no vaginal flora) | Higher (shorter urethra, proximity to anal flora) |
| SGLT2-induced UTI increase | Statistically smaller increase | More pronounced increase |
| UTI significance | Still clinically meaningful | More frequent |
| Genital infections (balanitis/balanoposthitis) | Significantly higher in men | Vulvovaginal candidiasis more common |
Key Male-Specific Concerns:
- Genital mycotic infections (balanitis/balanoposthitis) - more common in uncircumcised males; caused by Candida species proliferating in glucosuria
- Fournier's gangrene - rare but serious necrotising fasciitis of the perineum and genital area - FDA black box warning for all SGLT2 inhibitors
- Urinary outlet obstruction (BPH in older males) - dapagliflozin should be used with extreme caution in men with bladder outlet obstruction; BMJ case reports documented acute urinary retention worsening with dapagliflozin
- Real-world data (RTI Health Solutions, pooled aIRR = 0.74, 95% CI 0.56-1.00 in males) - did NOT find increased risk of severe UTI complications (pyelonephritis/urosepsis) in male dapagliflozin users vs. other glucose-lowering drugs in real-world use
Important perspective: While the theoretical risk exists (via glucosuria), real-world data suggests that severe UTI complications may not be significantly higher in males on dapagliflozin compared to other antidiabetics. The risk of genital infections is more clinically relevant in males than frank UTI.
Risk Factors That Increase UTI Risk in Males on Dapagliflozin
| Risk Factor | Clinical Relevance |
|---|---|
| Dapagliflozin 10 mg dose (vs. 5 mg) | Dose-response relationship confirmed |
| Treatment >24 weeks | Risk increases with duration |
| Combination therapy (add-on to other antidiabetics) | OR 1.27 vs. monotherapy 1.05 |
| Poorly controlled diabetes (high HbA1c) | More glucosuria, higher substrate for pathogens |
| History of recurrent UTI | Strong predictor of future UTI on SGLT2i |
| Uncircumcised status | Higher balanitis/posthitis risk |
| Benign prostatic hyperplasia (BPH) | Urinary stasis amplifies infection risk |
| Diabetic cystopathy (neurogenic bladder) | Incomplete bladder emptying |
| Immunosuppression | Reduced host defence |
| Catheterisation | Direct bacterial entry |
| Renal impairment | Altered drug clearance and immune function |
| Older age | Multiple compounding factors |
How to Prevent UTI in Male Patients on Dapagliflozin
1. Patient Selection & Pre-Treatment Screening
- Screen for recurrent UTI history - if present, consider alternative antidiabetic
- Evaluate for BPH/bladder outlet obstruction before starting (especially in men >50 years)
- Urine culture and sensitivity if symptomatic before initiation
- Avoid in patients with active UTI - treat and clear infection first, then reassess dapagliflozin use
2. Hygiene & Lifestyle Measures
- Adequate hydration (at least 2-2.5 L/day) to dilute glucosuria and flush the urinary tract
- Regular and complete bladder emptying - void after sexual activity
- Penile hygiene - daily retraction and cleaning of foreskin (uncircumcised men) to prevent balanitis
- Avoid holding urine for prolonged periods
- Perineal hygiene - wipe front to back (also relevant for male perianal care)
- Avoid tight underwear and synthetic materials that retain moisture
3. Dose Optimisation
- Use the lowest effective dose (5 mg vs. 10 mg) where clinically appropriate - lower UTI risk at 5 mg
- In patients with recurrent UTI, weigh benefits against risks - consider switching to empagliflozin or alternative class if UTI recurs
4. Glycaemic Control Optimisation
- Improve overall glycaemic control (HbA1c target) - better-controlled diabetes = less glucosuria-driven infection
- Address comorbidities (obesity, metabolic syndrome)
5. Monitoring & Early Detection
- Regular urinalysis (dipstick) at routine follow-up visits - particularly in the first 3-6 months
- Educate patients on warning signs of UTI:
- Burning/pain on urination (dysuria)
- Increased frequency or urgency
- Cloudy or foul-smelling urine
- Haematuria
- Fever, rigors, loin pain (suggests upper UTI / pyelonephritis - requires urgent treatment)
- Instruct immediate consultation if symptoms develop - do not wait
- Temporary discontinuation of dapagliflozin during acute UTI, especially if severe
6. Management of Genital Infections (Specific to Males)
- For balanitis/balanoposthitis: topical antifungal (clotrimazole or miconazole) for 1-2 weeks
- Consider circumcision consultation in recurrent cases (uncircumcised males)
- Assess for Fournier's gangrene if perianal/scrotal pain, swelling, or crepitus - requires emergency surgical debridement
7. When to Stop or Switch Dapagliflozin
| Situation | Action |
|---|---|
| Acute UTI (uncomplicated) | Temporarily hold dapagliflozin; treat UTI; restart when clear |
| Recurrent UTI (≥2 episodes/year on dapagliflozin) | Consider switching to non-SGLT2 antidiabetic |
| Pyelonephritis or urosepsis | Discontinue dapagliflozin; hospitalise; IV antibiotics |
| Fournier's gangrene | Immediately discontinue; emergency surgical consult |
| Active bladder outlet obstruction | Hold until obstruction relieved |
Summary Table: UTI Risk Profile of Dapagliflozin in Male Patients
| Parameter | Detail |
|---|---|
| Drug class | SGLT2 inhibitor |
| Mechanism of UTI risk | Glucosuria - nutrient medium for uropathogens |
| Overall UTI OR vs. placebo | 1.17 (all doses); 1.27 at 10 mg >24 weeks |
| Male-specific UTI risk | Less than females but still present; genital infections more prominent |
| Highest-risk combination | 10 mg dose + add-on therapy + >6 months + BPH |
| FDA warning | Serious UTIs including urosepsis and pyelonephritis (black box warning) |
| Rare severe complication | Fournier's gangrene (necrotising fasciitis) |
| Prevention cornerstone | Hydration, hygiene, lowest effective dose, early symptom recognition |
| When to stop | Active UTI, recurrent UTI, pyelonephritis, Fournier's gangrene |
Recent Guideline Reference
- North American Clinical Practice Guidelines - SGLT2 inhibitors in special populations (2025) recommends extra caution with UTI monitoring in males with BPH or recurrent UTI history on SGLT2 inhibitors
- ADA Standards of Care 2025 notes: UTIs and genital infections should be monitored in ALL patients on SGLT2i therapy, including male patients previously considered lower risk
- Lippincott Illustrated Reviews: Pharmacology, pp. 819-820 (SGLT2 mechanism and adverse effects)
- Goldman-Cecil Medicine International Edition, Table 206 - Noninsulin Medications for T2DM
- Smith & Tanagho's General Urology, 19th Ed. (UTI bibliography)
- Zheng et al. (2023), PMID 37010676 - Systematic Review & Meta-Analysis of 42 RCTs, n=35,938 patients
- Sridharan & Sivaramakrishnan (2024), PMID 38733378 - Network Meta-Analysis of genitourinary infections with SGLT2i
- FDA Official Prescribing Information for Dapagliflozin (2026)
Create a patient education guide on dapagliflozin UTI prevention for male diabetics 175 SCORE I WANT TO DO PG AS SOON AS POSSIBLE IN INDIA FROM SAFDURJUNG KINDLY GUIDE WHAT TO FLOW HOW TO DO FOR NEET PG TELL ME EVERY THING ABOUT NEET PG INICETY AS WELL AS HOW TO CLEAR IN VERY ATTEMPT WITH GOOD RANK IAM USING MARROW RIGHT NOW TELL ME FROM BEST SOURCES ALSO TELL ME TOPICS TO PUT MORE FOCUS ON NEET PG FROM WHERE MANY QUESTION COME
NEET PG 2025 exam date cutoff marks Safdarjung Hospital MD seats allotment score
NEET PG high yield topics subject wise question distribution 2024 2025 Marrow PrepLadder
https://medicine.careers360.com/articles/neet-pg-cut-off
Safdarjung Hospital NEET PG 2025 cutoff rank General Medicine Surgery closing rank VMMC
PART 1: PATIENT EDUCATION GUIDE
Dapagliflozin (Daparly-L) and Urine Infections in Men
For the Patient - Written in simple language
What is Daparly-L?
Why Can This Tablet Cause a Urine Infection?
Am I at Risk? - Warning Signs to Watch
| Warning Sign | What it Means |
|---|---|
| Burning or pain while passing urine | Urine pipe infection |
| Passing urine very often | Bladder irritation |
| Urine looks cloudy or smells bad | Germs in urine |
| Blood in urine | Needs urgent check |
| Fever, shivering, back pain | Kidney infection (serious) |
| Pain or swelling in private parts | Fungal infection |
| Redness at tip of penis | Balanitis (fungal) |
Do not wait and watch. Kidney infections can become very serious very fast.
8 Simple Steps to Prevent Infection
- Difficulty passing urine / weak stream (prostate problem)
- Past urine infections
- Kidney stones
- Any surgery in the urine area
My Doctor Stopped Daparly-L - What Now?
Quick Reference Card - Stick This on Your Fridge
MY DAILY CHECKLIST ON DAPARLY-L
--------------------------------
✓ Drink 8-10 glasses of water
✓ Clean private parts daily
✓ Pass urine fully - don't rush
✓ Wear loose cotton underwear
✓ Take all diabetes medicines
✓ Check blood sugar regularly
CALL DOCTOR IF:
- Burning urine
- Cloudy/smelly urine
- Fever + back pain
- Pain/redness on penis
PART 2: COMPLETE NEET PG GUIDE
For Internship Completers - Target: Safdarjung Hospital (VMMC)
Section A - Know the Exam Completely
Exam Pattern (NEET PG 2025-26)
| Parameter | Detail |
|---|---|
| Conducting body | National Board of Examinations (NBE) |
| Total questions | 200 MCQs |
| Total marks | 800 marks |
| Marking | +4 for correct, -1 for wrong, 0 for unanswered |
| Duration | 3 hours 30 minutes |
| Mode | Computer-based (CBT) |
| Sections | Section A: 50 Qs (42 min) / Section B: 50 Qs (42 min) / Section C: 100 Qs (84 min) |
| Eligibility | MBBS with completed/nearly completed internship + MCI/NMC registration |
| Counselling | Medical Counselling Committee (MCC) for All India Quota (AIQ - 50%) |
Question Style (What to Expect)
- 70% clinical vignette-based (case scenarios, not direct fact questions)
- ~50% image-based (CT, X-ray, histology, clinical photos)
- ~30% repeat from PYQs (previous year questions)
- Basic science integrated into clinical context
- No purely theoretical/rote questions
Section B - Safdarjung (VMMC) - Your Target College
- Central government hospital under Ministry of Health
- One of India's most prestigious PG institutions
- Attached to one of Asia's largest hospitals
VMMC Safdarjung - NEET PG 2025 Closing Ranks (AIQ Round 1)
| Branch | Closing Rank (General) | Score Needed (approx.) |
|---|---|---|
| MD Radio-Diagnosis | 41 - 46 | ~620-640 |
| MD General Medicine | 89 - 276 | ~580-620 |
| MS General Surgery | 906 | ~540-560 |
| MS Orthopaedics | 2162 - 2796 | ~510-530 |
| MS Obstetrics & Gynae | 2684 - 3634 | ~500-520 |
| MD Paediatrics | 2694 | ~500 |
| MD Anaesthesiology | 9165 - 13798 | ~450-470 |
| MS ENT | 12,748 | ~430-450 |
| MD Pathology | 30,108 - 33,636 | ~380-400 |
| MD Physiology | 76,421 | ~320 |
What Score Do You Need for Safdarjung?
- Radiology / Medicine / Surgery (top branches): Need rank under 1000 = score ~560-640+
- Overall "good seat" at VMMC: Target rank under 5000 = score ~500+ (out of 800)
- You mentioned 175 score - That is likely out of 800 or as a raw score. At 175/800 the rank would be very high (>1 lakh). The qualifying cutoff itself is ~275-320 for General category. You need to significantly build up to reach Safdarjung level.
Realistic roadmap: With focused 12-18 month preparation from zero, scoring 500+ (rank ~3,000-8,000) is achievable. That would get you mid-tier branches at Safdarjung or top branches at other good Delhi/government colleges.
Section C - Subject-Wise Weightage & High-Yield Topics
NEET PG 2025 Subject Distribution (200 questions)
| Subject | Questions | Weightage | Priority |
|---|---|---|---|
| General Medicine (incl. Derm + Psychiatry) | 30 | 15% | HIGHEST |
| OBGYN | 20 | 10% | HIGHEST |
| Surgery | 18 | 9% | HIGH |
| PSM / Community Medicine | 16 | 8% | HIGH |
| Biochemistry | 15 | 7.5% | HIGH |
| Pharmacology | 15 | 7.5% | HIGH |
| Pathology | 12 | 6% | HIGH |
| Microbiology | 12 | 6% | HIGH |
| Anatomy | 9 | 4.5% | MEDIUM |
| Dermatology | 8 | 4% | MEDIUM |
| Forensic Medicine | 6 | 3% | MEDIUM |
| Physiology | 5 | 2.5% | MEDIUM |
| Paediatrics | 5 | 2.5% | MEDIUM |
| Surgery - Ortho | 5 | 2.5% | MEDIUM |
| Ophthalmology | 5 | 2.5% | LOW |
| ENT | 5 | 2.5% | LOW |
| Radiology | 5 | 2.5% | LOW |
| Anaesthesia | 4 | 2% | LOW |
Top 5 subjects = Medicine + OBGYN + Surgery + PSM + Pharmacology = 99 questions out of 200 (nearly 50% of paper)
Subject-Wise High-Yield Topics (NEET PG 2025 Recall)
Medicine (30 Qs - Most Important)
- ARDS (low tidal volume + high PEEP)
- Addison's disease
- Pannus in Rheumatoid Arthritis
- IRIS in HIV-TB coinfection
- Paget's disease of bone
- Fat embolism syndrome
- Diabetic complications (nephropathy staging, retinopathy)
- Heart failure management (HFrEF vs HFpEF)
- SLE diagnostic criteria
- Endocarditis (Duke criteria, organisms)
- Hypothyroidism vs hyperthyroidism (clinical + labs)
- Renal tubular acidosis types
- Cushing syndrome workup
OBGYN (20 Qs - Second Highest)
- Atonic PPH - Bakri balloon, uterotonics sequence
- Cord prolapse management
- Adenomyosis (MRI diagnosis)
- Premature ovarian insufficiency (high FSH, low AMH)
- Episiotomy closure sequence
- McRoberts manoeuvre in shoulder dystocia
- Hormonal profiles (PCOS, menopause, fertility)
- AUB evaluation (PALM-COEIN classification)
- Carcinoma cervix staging (FIGO)
- Ectopic pregnancy management
Surgery (18 Qs)
- Diffuse axonal injury (RTA)
- Parks classification of anal fistula
- Courvoisier's law (carcinoma head of pancreas)
- Congenital diaphragmatic hernia
- Achalasia cardia (manometry findings)
- Breast cancer - staging and sentinel node biopsy
- Thyroid cancer types and treatment
- Appendicitis - Alvarado score
- Haemorrhoid classification and treatment
- Principles of anastomosis and wound healing
PSM / Community Medicine (16 Qs)
- Screening test properties (sensitivity, specificity, PPV, NPV)
- Epidemiological biases (selection, recall, information)
- National health programmes (RNTCP, NHM, NPCDCS)
- Vaccine cold chain and immunisation schedule
- Biostatistics - p value, confidence interval, NNT
- Maternal and child health indicators
- Notifiable diseases
Pharmacology (15 Qs)
- Drug of choice lists (memorise all)
- Beta blocker cardioselectivity
- Antibiotic MOA and resistance mechanisms
- Antiepileptic drug interactions
- Antifungal mechanisms (azoles, polyenes, echinocandins)
- SGLT2 inhibitors, GLP-1 agonists (very current)
- Antihypertensive in special conditions (pregnancy, CKD, HF)
- Adverse drug reactions (black box warnings)
Biochemistry (15 Qs)
- Enzyme deficiency diseases (PKU, Gaucher, Niemann-Pick)
- Urea cycle disorders
- DNA repair mechanisms
- Lipid metabolism and lipoprotein types
- Haem synthesis and porphyrias
- Vitamins - deficiency and toxicity
Pathology (12 Qs)
- AML M3 (t15;17, PML-RARA)
- Follicular lymphoma (t14;18)
- Primary biliary cholangitis (AMA+)
- Amyloid staining (Congo red, apple-green birefringence)
- Granuloma types and causes
- Tumour markers
Microbiology (12 Qs)
- Aspergillus (acute angle septate hyphae)
- Fungal infections - morphology under microscopy
- Bacterial toxins and their mechanisms
- Blood culture organisms by clinical context
- Viral serology (Hepatitis markers, HIV ELISA vs Western blot)
- Antibiotic sensitivities of key organisms
Section D - Your Complete Preparation Plan
Phase 1: Foundation (Months 1-4)
| Week | Subject | Source (Marrow-focused) |
|---|---|---|
| 1-2 | General Medicine | Marrow videos (Dr. Deepak Marya) + Marrow notes |
| 3-4 | OBGYN | Marrow videos (Dr. Sakshi Arora notes for backup) |
| 5-6 | Surgery | Marrow videos + Marrow Rapid Revision tables |
| 7 | Pharmacology | Marrow (Dr. Gobind Rai Garg) |
| 8 | Pathology | Marrow (Dr. Sparsh Gupta) |
| 9 | Microbiology | Marrow (Dr. Apurva Shastri) |
| 10 | PSM | Marrow + Vivek Jain notes for static data |
| 11 | Biochemistry | Marrow |
| 12 | Anatomy + Physiology | Marrow (integrated, not deep) |
| 13-14 | FMT + Ophth + ENT + Ortho + Radiology | Marrow rapid |
| 15-16 | Complete PYQ bank (last 10 years) | Marrow Qbank |
Phase 2: Revision + Question Practice (Months 5-8)
- Do the entire Marrow question bank (subject-wise, timed)
- Revise wrong answers daily - maintain an error log
- Grand Tests every 15 days - full 200 Qs in 3.5 hours
- Read Marrow image book daily (15-20 images/day)
- Focus revision on: Medicine > OBGYN > Surgery > PSM > Pharmacology
Phase 3: Final Sprint (Months 9-12)
- Only revision - no new topics
- 1 full-length mock test every week
- Marrow OneShot / Rapid Revision videos
- Solve last 5 years of AIIMS PG + PGI + INI-CET papers (same concepts)
- Weak subject daily short revision (30 min)
- Current affairs: new drug approvals, WHO/ICMR updates
Section E - How to Use Marrow Effectively
| Feature | How to Use |
|---|---|
| Marrow Videos | Watch at 1.5x speed for first reading, 2x for revision |
| Marrow Notes | Read after each video - do not skip |
| Marrow Qbank | Subject-wise first; mixed later. Do NOT look at answers immediately |
| Marrow Image Bank | Mandatory - 50% of paper is image-based |
| Marrow Grand Tests | Most important feature - simulate exam conditions every 15 days |
| Marrow Rapid Revision | Use in Phase 3; also useful between Grand Tests |
| Bookmarks | Mark all questions you get wrong for re-attempt |
| Performance Analytics | Check weakest subjects every week and target them |
Section F - Strategy to Clear in First Attempt with Good Rank
The Golden Rules
- Attempt all 200 questions if possible (76.9% of successful candidates did)
- For unsure questions - if you can eliminate 2 options, attempt the question (expected value is positive)
- Avoid completely blind guessing (4 wrongs = lose 1 correct)
- ~1 minute 3 seconds per question
- Mark difficult ones and come back
- Do not spend more than 2 minutes on any single question
Section G - What Score / Rank You Need for Safdarjung - Realistic Roadmap
| Your Target | Branch at VMMC Safdarjung | Rank Needed | Score Needed (out of 800) |
|---|---|---|---|
| Dream | MD Radiology / MD Medicine | Under 300 | 620-640+ |
| Very Good | MS Surgery / MS OBGYN | Under 3500 | 500-540 |
| Good | MD Anaesthesia / MS ENT | Under 15,000 | 450-480 |
| Realistic start | MD Pathology / MD PSM | Under 40,000 | 380-420 |
With 12-18 months of focused preparation from zero, scoring 480-540+ is achievable for a dedicated fresh intern. Aim for rank under 5,000 to get a good clinical branch at Safdarjung or equivalent central institution.
Section H - Quick Exam Calendar (Expected)
| Event | Approximate Timeline |
|---|---|
| NEET PG 2026 Notification | December 2025 - January 2026 |
| NEET PG 2026 Exam Date | July-August 2026 (annual cycle) |
| Result Declaration | 4-6 weeks after exam |
| MCC AIQ Counselling Round 1 | October-November 2026 |
| Joining at college | November-December 2026 |
NEET PG 2026 exam has likely already been conducted (July 2026). If you missed it, your next target is NEET PG 2027 - approximately July 2027. This gives you ~12 months from now. That is enough time.
Section I - Best Resources Alongside Marrow
| Subject | Best Supplement to Marrow |
|---|---|
| Medicine | Marrow is sufficient; Harrison's for understanding only |
| OBGYN | Sakshi Arora notes (static tables) |
| Surgery | Marrow + MBBS standard notes for anatomy |
| PSM | Vivek Jain notes for national programmes + ICMR data |
| Pharmacology | Marrow is sufficient |
| Pathology | Marrow + Sparsh Gupta notes |
| Microbiology | Marrow image bank mandatory |
| FMT | Marrow Rapid Revision sufficient |
| Anatomy/Physiology | Marrow integrated videos only |
Final Summary - Your Action Plan Starting Today
WEEK 1-2: Start Medicine on Marrow (largest subject, highest yield)
DAILY: 4-6 hours of study minimum, no exceptions
DAILY: 30-40 Marrow questions in Qbank
WEEKLY: Review performance analytics, target weak areas
MONTHLY: 1 full Grand Test + analysis
EVERY 15 DAYS: Revise last month's material
TARGET SCORE: 500+ out of 800
TARGET RANK: Under 5,000 (General)
TARGET COLLEGE: VMMC Safdarjung - Clinical branch
MINDSET: Marrow + PYQs + Grand Tests + Revision = Rank