You are 2nd year mbbs student tell me detail about pathogenesis of entamoeba histolytica
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, detailed information from multiple authoritative textbooks. Let me compile the full answer now.
Pathogenesis of Entamoeba histolytica (Amebiasis)
1. The Organism - Quick Recap
E. histolytica exists in two forms:
- Cyst (10-20 µm): Infective form, quadrinucleate, has chitin wall, resistant to gastric acid and chlorination. Has rounded-end chromatoid bars (key ID feature).
- Trophozoite (10-60 µm): The ONLY form present in tissues, responsible for all pathology. Has ingested RBCs in cytoplasm - pathognomonic finding.
Note: E. histolytica is morphologically identical to non-pathogenic E. dispar, E. moshkovskii, and E. bangladeshi - molecular methods are needed for differentiation.
2. Life Cycle and Entry
- Ingestion - Cysts are swallowed in fecally contaminated food/water
- Excystation - Cysts pass through the stomach (gastric acid actually triggers excystation), then in the duodenum/small intestine the quadrinucleate cyst undergoes nuclear and cytoplasmic division → 8 trophozoites per cyst
- Colonization - Trophozoites travel to the large intestine (cecum and ascending colon most commonly) and multiply under anaerobic conditions (they are obligate fermenters of glucose; they lack mitochondria and Krebs cycle enzymes)
Only 10-20% of infected persons develop invasive disease. The rest remain asymptomatic carriers.
3. Pathogenesis - Stepwise Invasion (The Core Topic)
The stepwise invasion of the colonic mucosa is the centerpiece of E. histolytica pathogenesis:
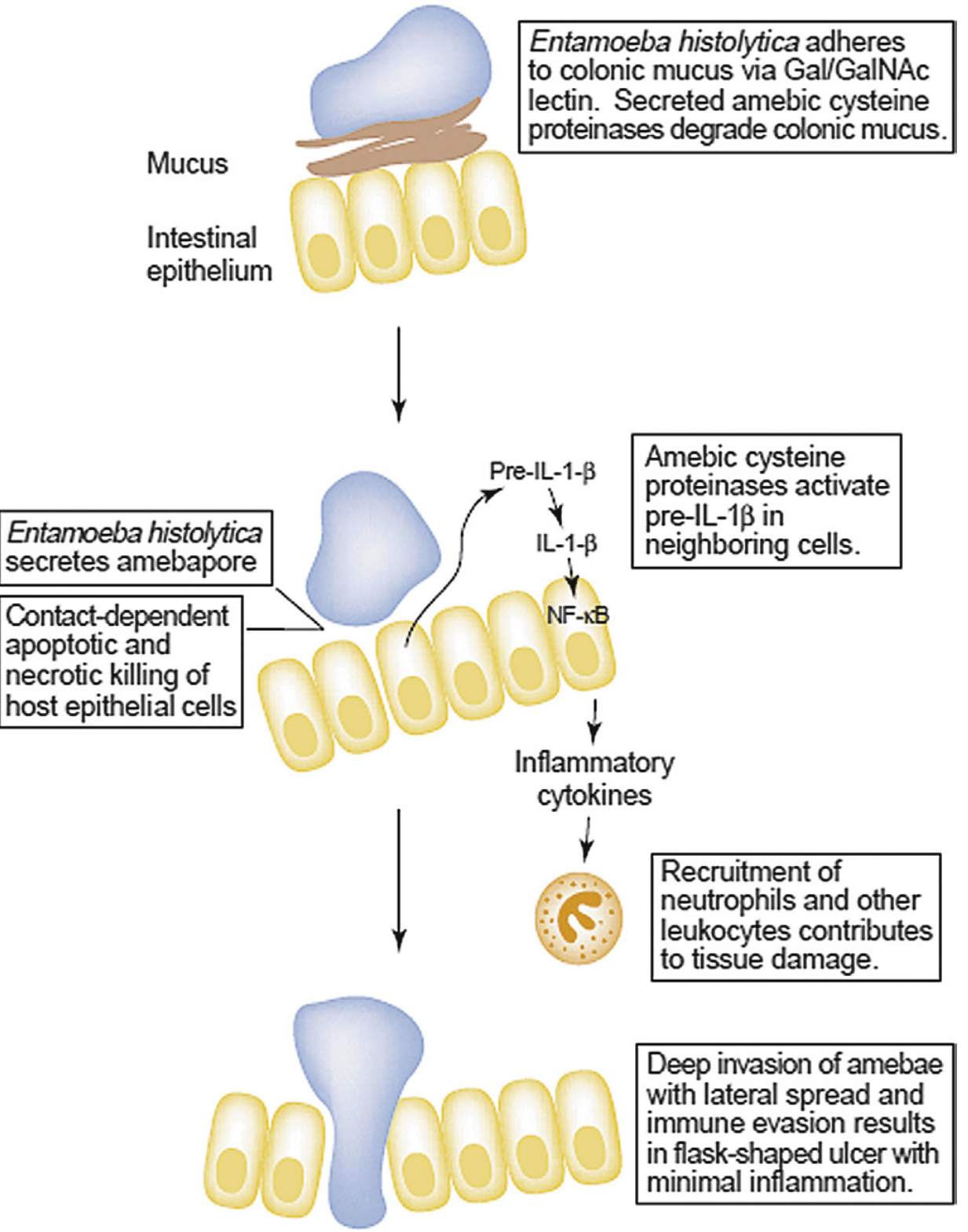
Fig. 113.2 - Model for stepwise colonic invasion by E. histolytica (Sleisenger & Fordtran's Gastrointestinal and Liver Disease)
Step 1: Adherence to Colonic Mucus
- Trophozoites adhere to colonic mucins via the Gal/GalNAc lectin (galactose/N-acetylgalactosamine-inhibitable adherence lectin)
- This lectin binding is essential for subsequent cytolysis - without contact, no killing occurs
- The lectin is also important for immune evasion and liver abscess formation
Step 2: Mucus Degradation
- Secreted amebic cysteine proteinases (especially cysteine protease 5/EhCP5) degrade the polymeric structure of colonic mucin
- This breaks the protective mucus barrier and enables direct contact with the underlying colonic epithelium
Step 3: Contact-Dependent Killing of Epithelial Cells
Once direct contact is established, trophozoites kill host cells via THREE mechanisms:
| Mechanism | Details |
|---|---|
| Apoptosis induction | Contact-dependent signaling triggers programmed cell death in epithelial cells |
| Necrosis | Via amebapore - a pore-forming protein that inserts into lipid membranes, forms ion channels, depolarizes target cells, and causes an irreversible increase in intracellular Ca²⁺ → membrane permeability alteration → lytic necrosis |
| Trogocytosis ("nibbling") | A phenomenon where trophozoites take small bites of living host cell membranes piece by piece, ultimately killing the cell |
Step 4: Inflammatory Amplification (Host Damage)
- Amebic cysteine proteinases activate pre-IL-1β → IL-1β in neighboring epithelial cells
- IL-1β activates NF-κB, triggering a pro-inflammatory cytokine cascade
- This recruits neutrophils to the site
- Trophozoites then lyse the neutrophils, releasing toxic neutrophil granule contents - this causes further, amplified tissue damage (essentially the ameba turns the host's own defenses against the host)
Step 5: Tissue Invasion and Flask-Shaped Ulcer Formation
- After epithelial destruction, trophozoites degrade the extracellular matrix via proteinases and invadopodia (similar to metastatic cancer cell invasion structures)
- Trophozoites accumulate above the muscularis mucosae - downward invasion is often halted here for unclear reasons
- They then spread laterally, undermining the overlying mucosa
- This produces the classic "flask-shaped ulcer": narrow neck through the mucosa, expanding into a broad necrotic area in the submucosa
- The ulcers have a pinhead-sized opening, small neck, and large base - undermining large mucosal surfaces
- In established ulcers, few inflammatory cells are seen (immune evasion is highly effective)
4. Virulence Factors Summary Table
| Virulence Factor | Function |
|---|---|
| Gal/GalNAc lectin | Adhesion to colonic mucins + epithelial cells; required for cytolysis |
| Cysteine proteinases (EhCPs) | Degrade mucus, ECM, complement; activate IL-1β; cleave IgA |
| Amebapore | Pore-forming protein → membrane depolarization → Ca²⁺ influx → cell lysis |
| Phospholipase A | Membrane damage |
| Erythrophagocytosis | Ingestion of RBCs - pathognomonic; provides nutrients, suppresses oxidative burst |
5. Extraintestinal Spread
Once the mucosa is breached, trophozoites penetrate the splanchnic (portal) vessels and are carried hematogenously to distant sites:
-
Liver (most common) - ~40% of amebic dysentery cases develop liver abscesses
- Amebic liver abscesses: >10 cm, "anchovy paste" contents, scant inflammatory reaction at margins, shaggy fibrinous lining
- Central liquefaction of tissue, minimal mononuclear cell infiltrate
-
Lung - by direct extension from liver (transdiaphragmatic) or hematogenous spread
-
Brain - hematogenous spread (rare)
-
Pericardium/Heart - direct extension (rare)
-
Kidney - hematogenous (rare)
Key note: Amebae survive only in environments with low oxygen pressure (anaerobic). Ambient oxygen concentrations kill them - this is why they favor mucosal crypts and anaerobic tissue planes.
6. Host Factors that Determine Invasion
As summarized by Jawetz Microbiology, factors determining whether invasion occurs:
- Number of cysts ingested
- Pathogenic capacity of the strain (genetic polymorphisms in the E. histolytica genome correlate with virulence)
- Host factors: gut motility, immune competence, HLA class II alleles (susceptibility is linked to specific HLA types), leptin receptor mutation affecting epithelial cell signaling
- Enteric bacterial flora: certain bacteria enhance amebic growth
7. Immune Response and Evasion
- Children with fecal anti-amebic lectin IgA have short-lived protection against re-infection
- Amebic cysteine proteinases cleave IgA - a direct immune evasion mechanism
-
90% of colonized persons spontaneously clear infection within a year
- The parasite kills neutrophils and lymphocytes, releasing their toxic contents to cause more damage while eliminating the immune response
8. Pathology - What You'll See
| Site | Gross/Microscopic Findings |
|---|---|
| Colon (early) | Mucosal thickening, multiple punctate ulcers with normal intervening tissue |
| Colon (classic) | Flask-shaped ulcers - narrow neck, broad submucous base, shaggy overhanging edges |
| Histology | Acute inflammation + hemorrhage; trophozoites with ingested RBCs (erythrophagocytosis); amebae resemble macrophages (diagnostic pitfall) |
| Liver abscess | >10 cm cavity, "anchovy paste"/chocolate-colored pus, fibrinous lining, minimal surrounding inflammation |
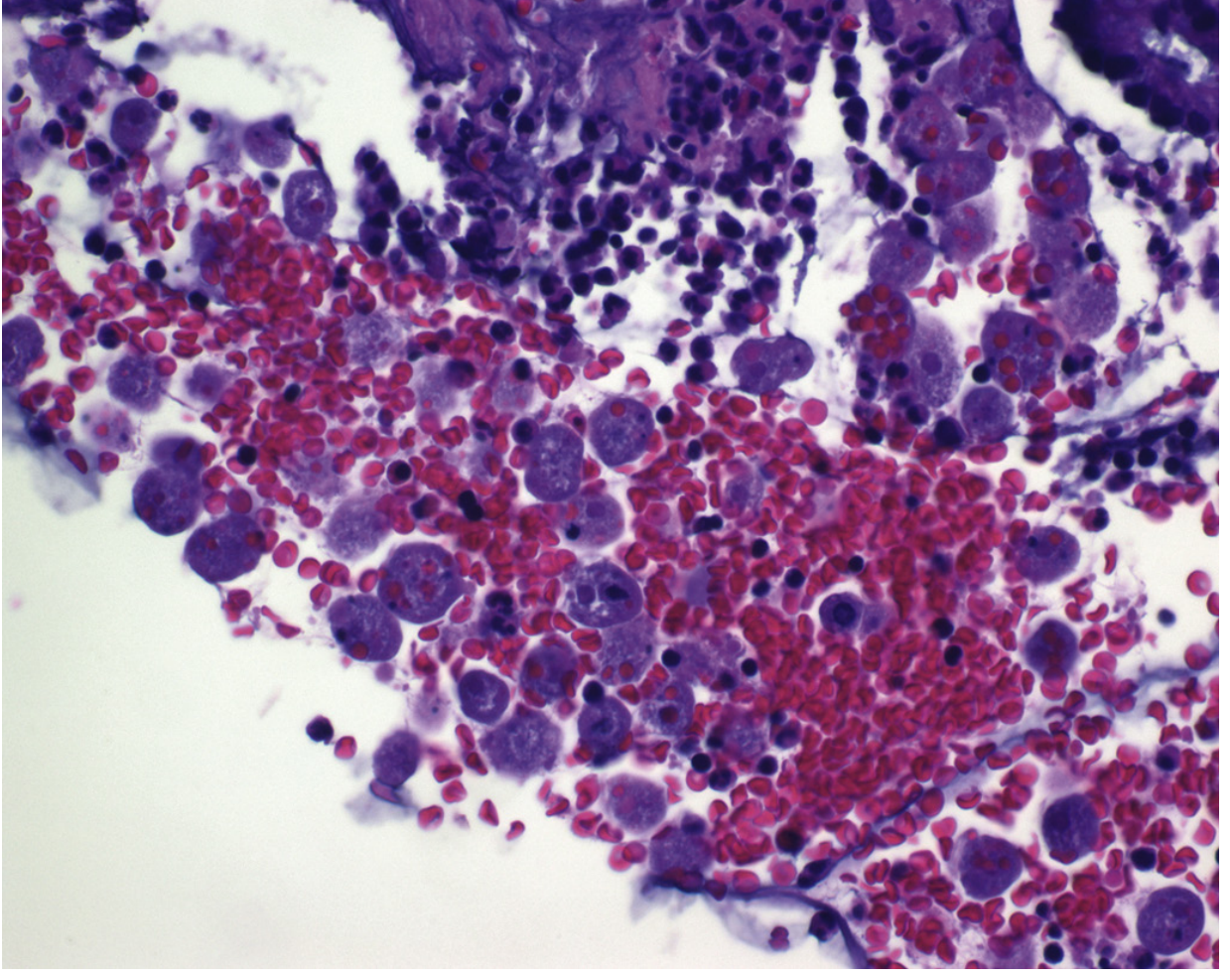
Fig. 113.4 - Amebic colitis biopsy. Trophozoites with ingested RBCs (erythrophagocytosis) - H&E stain (Sleisenger & Fordtran)
9. Treatment Basis (Biochemical Rationale)
E. histolytica lacks mitochondria and Krebs cycle enzymes - it is an obligate fermenter of glucose. Metronidazole inhibits pyruvate oxidoreductase (ferredoxin-linked), an enzyme required for anaerobic fermentation. This is why metronidazole is the most effective treatment for systemic/invasive disease.
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 113
- Medical Microbiology, 9e (Murray), Ch. 72
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28e, Ch. 46
This is a shared conversation. Sign in to Orris to start your own chat.