Bires block acoording millers books refferance in simple way
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, simple explanation. Here is the full answer:
Bier's Block (Intravenous Regional Anesthesia - IVRA)
Based on Miller's Anesthesia 10th Ed., Campbell's Operative Orthopaedics 2026, and Pfenninger & Fowler's Procedures for Primary Care
What Is It?
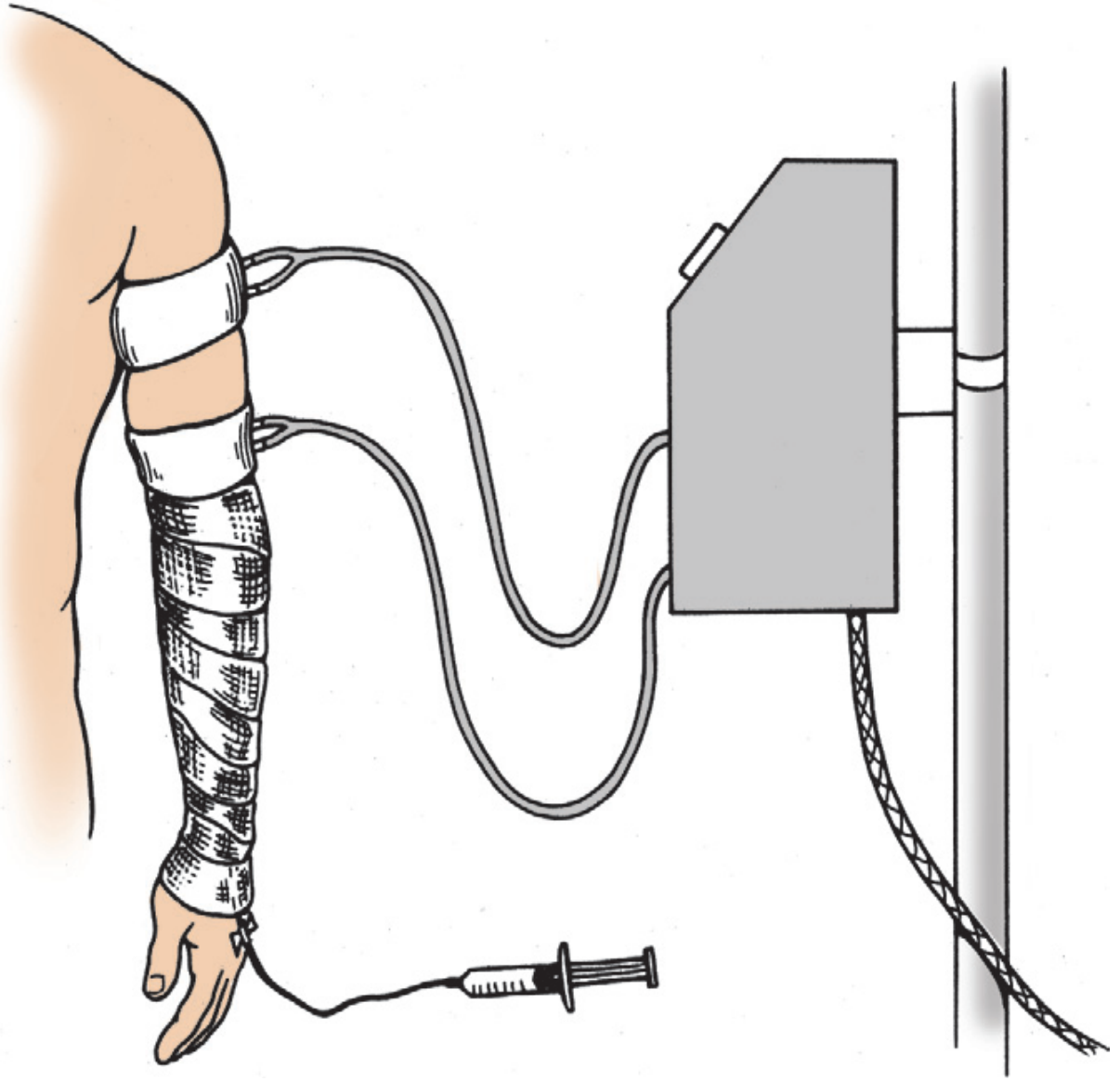
Bier's block is a technique where a local anesthetic is injected into a vein of a tourniquet-occluded limb. The drug diffuses from blood vessels to nearby nerves, producing anesthesia of the whole limb below the tourniquet. It is simple, reliable, and especially useful for short upper limb surgery (45-90 minutes).
How It Works (Mechanism)
The tourniquet cuts off blood flow. The injected local anesthetic diffuses from the venous bed outward to nerve trunks and free nerve endings. Both safety and effectiveness depend entirely on:
- Maintaining complete tourniquet occlusion during the procedure
- Gradual, controlled tourniquet release at the end
- Miller's Anesthesia, 10e, p. 3591
Step-by-Step Technique
| Step | What You Do |
|---|---|
| 1 | Take history, check allergies, NPO status, airway class |
| 2 | Attach cardiac monitor + pulse oximeter. BP cuff on the other arm |
| 3 | Place 2 IV lines - one on the operative arm (for LA), one on the other arm (for emergency drugs) |
| 4 | Optional: give midazolam 2-4 mg IV for comfort |
| 5 | Place a double pneumatic tourniquet on the proximal limb. Test it first |
| 6 | Elevate the arm and wrap an elastic bandage distal to proximal (Esmarch) to exsanguinate the limb |
| 7 | Inflate the proximal cuff to systolic + 50-100 mmHg (upper limb) or 2x systolic (lower limb) - usually 250-300 mmHg |
| 8 | Lower the arm, remove the bandage, check for absent distal pulse - then inject lidocaine |
| 9 | Wait 10-15 min for anesthesia to develop; test by gentle manipulation at the operative site |
| 10 | Once the proximal tourniquet becomes uncomfortable: inflate the distal cuff first, then deflate the proximal one. The anesthetic under that distal cuff numbs the skin under the new inflated cuff - reducing tourniquet pain |
| 11 | Operate. Maximum tourniquet time = 2 hours |
| 12 | At end: release cuffs no sooner than 20 min after injection (allows drug to diffuse out of vasculature) |
| 13 | Observe 10-15 min for signs of toxicity |
- Pfenninger & Fowler's Procedures for Primary Care, pp. 31-32
Drug of Choice and Dose
| Drug | Dose / Volume | Notes |
|---|---|---|
| Lidocaine (upper limb) | ~3 mg/kg, 40 mL of 0.5% solution (for 65-70 kg) | Most widely used; preservative-free, no epinephrine |
| Lidocaine (lower limb) | 50-100 mL of 0.25% solution | Higher volume needed |
| Prilocaine | Preferred in UK/Europe | Higher therapeutic index, lower toxicity |
| Ropivacaine | 0.2-0.375% | Longer postoperative analgesia but slower onset; higher plasma levels than prilocaine |
Never use bupivacaine - it has high cardiotoxicity potential if accidentally released into systemic circulation.
- Miller's Anesthesia, 10e, pp. 3591, 9997
Indications
- Short upper limb surgery: carpal tunnel release, hand fracture manipulation, tendon repairs
- Can be used for lower limb but less common
- Cost-effective alternative to general anesthesia for day-case surgery
- Miller's Anesthesia, 10e, p. 9997
Adjuvants (to Improve Block Quality)
| Adjuvant | Benefit |
|---|---|
| NSAIDs (lornoxicam, tenoxicam) | Reduce tourniquet pain, improve postoperative analgesia |
| Dexamethasone | Improves both block quality and postoperative analgesia |
| Dexmedetomidine (alpha-2 agonist) | Similar to dexamethasone |
| Opioids | Relatively ineffective + cause nausea/vomiting after cuff deflation |
Complications
| Complication | Cause / Notes |
|---|---|
| Local anesthetic toxicity | Most serious - especially if cuff deflates early |
| Seizures | Can occur with lidocaine as low as 1.4 mg/kg if cuff fails; treat with IV benzodiazepines/propofol |
| Cardiovascular collapse | Rare; almost always due to operator error or equipment failure |
| Cardiac arrhythmias | Bradycardia, cardiac arrest (rare) |
| Dizziness, tinnitus, bradycardia | Minor reactions in <2% after cuff deflation |
| Ecchymosis under tourniquet | Pad the arm with web roll to minimize |
| Compartment syndrome | Rare but reported |
- Campbell's Operative Orthopaedics 2026, p. 3510; Pfenninger & Fowler, p. 32
Double Tourniquet - Why and How

The proximal cuff is inflated first. Once the patient feels tourniquet pain (usually 20-30 min), the distal cuff - which now sits over anesthetized skin - is inflated and the proximal cuff deflated. This dramatically reduces tourniquet discomfort.
Key Safety Rules
- Never deflate the tourniquet before 20 minutes have passed from injection
- Never use bupivacaine for IVRA
- Always have resuscitation equipment and an ACLS-trained person present
- A dedicated person must continuously watch tourniquet pressure throughout the case
- The surgeon and the person monitoring the patient must be two different people
Quick Summary
IVRA / Bier's Block = tourniquet on limb → exsanguinate → inject lidocaine IV → wait 10-15 min → operate → release cuff after min. 20 min. Simple, cheap, effective for short limb procedures.
- Miller's Anesthesia 10e (pp. 3591, 9997); Campbell's Operative Orthopaedics 2026 (p. 3504); Pfenninger & Fowler's Procedures for Primary Care (pp. 31-32)
This is a shared conversation. Sign in to Orris to start your own chat.