Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have the complete Box 8.3 listing the contraindications to NPPV. Let me analyze the question:
Answer
Correct answer: (b) I, II and IV
Here is a breakdown of each option:
Contraindications to NPPV - Analysis of Each Statement
| # | Statement | Contraindication? | Explanation |
|---|---|---|---|
| I | Craniofacial abnormalities | YES | Facial surgery, trauma, or deformity limiting placement of the mask is a listed contraindication to NPPV - it prevents achieving an adequate mask seal. |
| II | Significant burns | YES | Burns to the face/head constitute facial injury/deformity that prevents mask placement and adequate seal - this is a contraindication. |
| III | Respiratory failure with PaCO2 of 60 mm Hg | NO - NOT a contraindication | Hypercapnia (elevated PaCO2) is actually one of the indications for NPPV, not a contraindication. NPPV is used precisely to treat type II (hypercapnic) respiratory failure, e.g., in COPD exacerbations. PaCO2 of 60 mm Hg is not a reason to avoid NPPV. |
| IV | Cardiovascular instability | YES | "Impending cardiovascular collapse" is explicitly listed as a contraindication to NPPV (Roberts and Hedges' Clinical Procedures in Emergency Medicine, Box 8.3). Rosen's Emergency Medicine also lists "hemodynamic instability" as a relative contraindication. |
Accepted Contraindications to NPPV (Box 8.3, Roberts & Hedges)
- Impending cardiovascular collapse or respiratory arrest
- Severe upper gastrointestinal bleeding
- Facial surgery, trauma, or deformity limiting mask placement
- Upper airway obstruction
- Inability to cooperate or protect the airway / altered mental status
- Inability to clear respiratory secretions
- High risk for aspiration
Why Option III (PaCO2 = 60 mm Hg) is NOT a contraindication
Hypercapnic respiratory failure is one of the strongest indications for NPPV - particularly in COPD exacerbations. Studies have even shown NPPV works in patients with hypercapnic coma (GCS <10) when monitored carefully in specialized units. A PaCO2 of 60 mm Hg is a trigger to use NPPV, not avoid it.
The answer is (b): I, II and IV - per Roberts and Hedges' Clinical Procedures in Emergency Medicine.
What is hidebound chest
Finding Sources
Searching the Web
hidebound chest definition clinical sign scleroderma
Reading File
Reading File
Excellent - the textbooks give a very complete picture. Here is the full answer:
Hidebound Chest
Hidebound chest is a clinical sign where the skin of the chest wall becomes tight, thickened, fibrotic, and bound down to the underlying structures - restricting chest wall movement and respiratory excursion. The term "hidebound" refers to skin that is so taut it resembles hide (animal skin) stretched tightly over a frame.
Cause
It is the hallmark feature of systemic sclerosis (scleroderma) - specifically diffuse cutaneous systemic sclerosis. The underlying mechanism is excessive collagen deposition in the dermis, causing the skin to become:
- Smooth, firm, yellowish, and inelastic
- Shrunken and bound down to deeper structures
- Immobile - unable to be lifted or pinched from the chest wall
What Happens to the Chest
From Andrews' Diseases of the Skin:
"A diffuse involvement of the chest may lead to a cuirass-like restraint of respiration."
The term "cuirasse" (a breastplate of armour) is also used - "thorax en cuirasse" - because the rigid, armour-like skin immobilizes chest expansion. This leads to:
- Restrictive lung physiology - reduced total lung capacity (TLC) and vital capacity (VC)
- Impaired ventilation and increased work of breathing
- Contributes to the pulmonary complications of scleroderma (alongside interstitial fibrosis)
The Full Picture of "Hidebound" Skin in Scleroderma
From Fishman's Pulmonary Diseases & Disorders:
"The skin manifestations progress to tapered fingers with shiny, hidebound skin (sclerodactyly). The feet, chest, face, and scalp are often involved in the sclerotic process. In time, the skin becomes taut, leading to contractures of the large and small joints."
From Andrews' Diseases of the Skin:
"In more advanced stages, these parts become hidebound, so the face is expressionless, the mouth is constricted, and the hands are clawlike."
Other Conditions Causing Hidebound Skin
The term "hidebound" can apply to skin bound down in other settings too:
- Carcinoma en cuirasse - metastatic breast carcinoma infiltrating the chest skin, causing indurated, hidebound, leathery skin (scirrhous carcinoma)
- Chronic graft-versus-host disease (cGVHD) - can produce "pipestem" limbs with overlying shiny hidebound skin resembling scleroderma
- Restrictive dermopathy (rare genetic disorder)
Clinical Examination Finding
On examination, hidebound chest presents as:
- Chest skin that cannot be pinched or lifted off the chest wall (the classic test)
- Reduced chest expansion on measurement (normal >5 cm)
- Associated signs of scleroderma: sclerodactyly, Raynaud's phenomenon, facial tethering, telangiectasia
Summary Table
| Feature | Detail |
|---|---|
| Definition | Tight, fibrotic skin bound to the chest wall, restricting expansion |
| Primary disease | Systemic sclerosis (scleroderma) |
| Mechanism | Excess collagen deposition in dermis |
| Respiratory effect | Restrictive ventilatory defect |
| Also called | Thorax en cuirasse |
| Other causes | Carcinoma en cuirasse, cGVHD |
- Andrews' Diseases of the Skin, Clinical Dermatology (scleroderma section)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
Where are rheumatic pulmonary nodules lovated and what are there charctericritics
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, textbook-referenced answer:
Rheumatoid (Necrobiotic) Pulmonary Nodules
These are extra-articular manifestations of rheumatoid arthritis (RA) in the lung parenchyma. They are also called necrobiotic nodules.
Location
From Fishman's Pulmonary Diseases and Disorders:
"In the lung parenchyma, these nodules are located in the interlobular septa and in the subpleural parenchyma."
From Rheumatology (Elsevier 2022):
"The pulmonary nodules tend to be peripheral in location."
They can also appear in the pleura itself. In Caplan syndrome (RA + pneumoconiosis), several nodules >1 cm are scattered throughout the peripheral lung fields.
Summary of location:
- Subpleural (just under the visceral pleura) - most common
- Interlobular septa
- Pleura itself
- Peripheral lung fields (especially in Caplan syndrome)

Characteristics
Clinical Features
| Feature | Detail |
|---|---|
| Symptoms | Generally asymptomatic |
| Who gets them | Seropositive patients (RF+) with widespread synovitis and rheumatoid nodules elsewhere |
| Sex | Men more commonly affected |
| Number | Single or multiple/clustered |
| Size | < 1 cm up to 6-8 cm in diameter |
Histological Features
From Fishman's Pulmonary Diseases and Disorders:
"The necrobiotic nodule is comprised of palisading histiocytes, giant cells, and other mononuclear cells surrounding an area of fibrinoid debris."
They are identical in appearance to subcutaneous rheumatoid nodules.
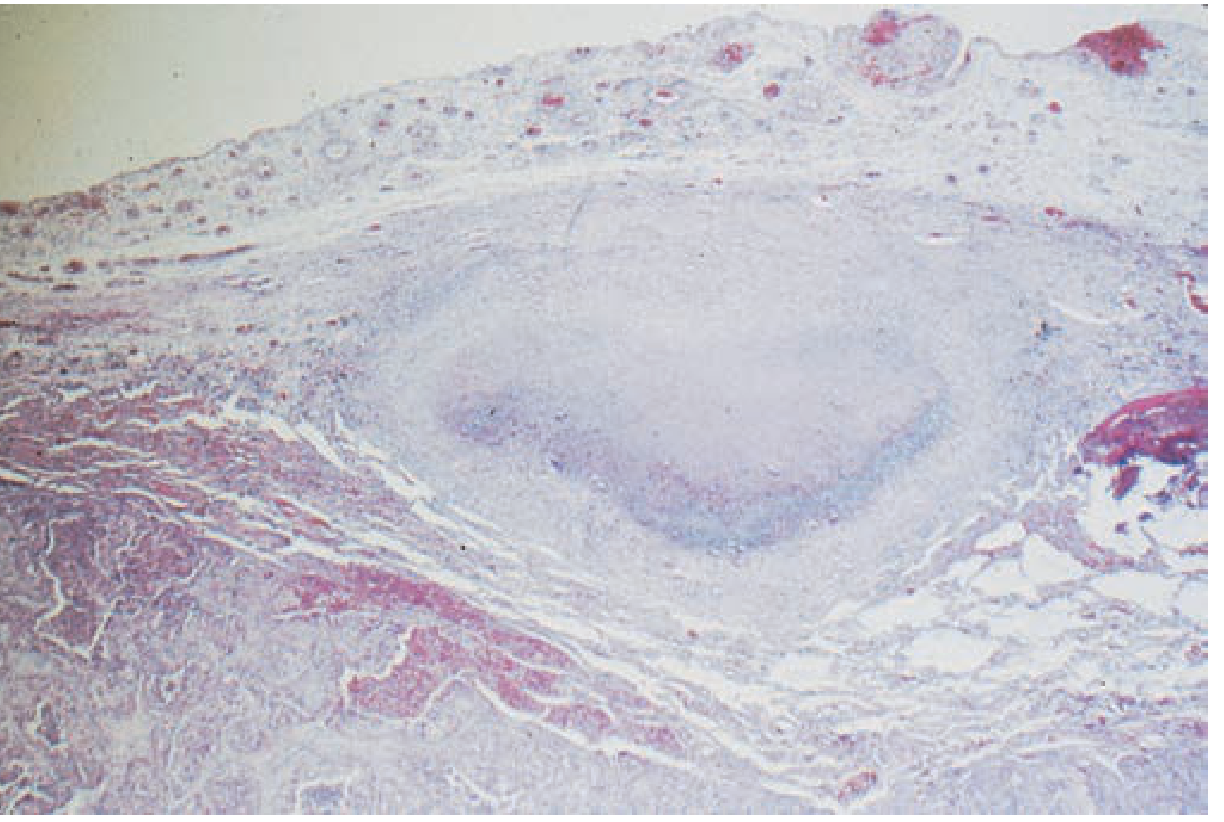
Three-layered structure:
- Central zone - fibrinoid necrosis / fibrinoid debris
- Middle zone - palisading histiocytes and proliferating fibroblasts
- Outer zone - mononuclear cells, giant cells, inflammatory infiltrate
Complications
From Firestein & Kelley's Textbook of Rheumatology:
"Pulmonary nodules from RA can cavitate, leading to the formation of bronchopleural fistulas and rarely pneumothorax."
Full list of complications:
- Cavitation (due to central necrosis)
- Bronchopleural fistula
- Pneumothorax
- Pleural effusion
- Hemoptysis
- Secondary infection of cavitated nodule
Differential Diagnosis
Must be distinguished from:
- Bronchogenic carcinoma (important - PET/CT may not reliably discriminate)
- Tuberculosis
- Fungal infections (histoplasmosis, coccidioidomycosis)
- Metastatic malignancy
A solitary pulmonary rheumatoid nodule may require excisional biopsy to confirm the diagnosis and exclude malignancy.
Special Association: Caplan Syndrome
Rheumatoid nodules + pneumoconiosis (coal dust, silica, asbestos exposure) = Caplan syndrome. Nodules here are:
- Multiple, >1 cm
- Scattered throughout peripheral lung fields
- Appear rapidly, often in crops
- May precede joint manifestations
Treatment
"Treatment of the underlying rheumatoid disease frequently results in improvement in the pulmonary nodules." - Rheumatology, Elsevier 2022
- Fishman's Pulmonary Diseases and Disorders, Chapter 58
- Rheumatology, 2-Volume Set (Elsevier 2022), Chapter 91
- Firestein & Kelley's Textbook of Rheumatology, Chapter 72
What is lemeirre syndrome
Finding Sources
Searching the Web
Lemierre syndrome definition pathophysiology treatment
Reading File
Reading File
Reading File
Reading File
I now have comprehensive textbook content for a full answer.
Lemierre Syndrome
Also called "the forgotten disease" or postanginal septicemia, Lemierre syndrome is a rare but potentially fatal condition first described by French physician André Lemierre in 1936.
Definition
Septic thrombophlebitis of the internal jugular vein arising from a primary oropharyngeal infection, leading to bacteremia and metastatic septic emboli - most commonly to the lungs.
Causative Organism
| Organism | Detail |
|---|---|
| Fusobacterium necrophorum | Responsible for ~81% of cases |
| Other Fusobacterium spp. | Can cause the same presentation |
| Arcanobacterium haemolyticum, Bacteroides spp. | Lemierre-like syndromes |
F. necrophorum is a gram-negative anaerobic rod, cigar/spindle-shaped, found in normal flora of the oropharynx, GI tract, and female genital tract. In the anaerobic conditions of a peritonsillar abscess, it multiplies rapidly, invades the circulation, and causes severe systemic sepsis.
Pathophysiology (Step-by-Step)
Oropharyngeal infection (tonsillitis / pharyngitis / peritonsillar abscess)
↓
F. necrophorum invades local tissues → anaerobic multiplication
↓
Spread to peritonsillar/parapharyngeal space → local vascular invasion
↓
Septic thrombophlebitis of the INTERNAL JUGULAR VEIN
↓
Bacteremia + septic emboli → metastasize to distant organs
↓
Lungs (most common), bone/joints, liver, CNS
Who Gets It
- Predominantly young, otherwise healthy adolescents and young adults
- Incidence: ~3.6 cases/million/year (rare)
- Declined dramatically after antibiotics in the 1940s, but recently increasing again
Clinical Features
Classic triad:
- Preceding sore throat / oropharyngeal infection
- Unilateral neck swelling and tenderness (over the jugular vein)
- Evidence of septic emboli (especially pulmonary)
Symptoms:
- High fever, rigors, chills
- Sore throat, neck pain, neck swelling
- Dyspnea (23.8%), pleuritic chest pain (31.1%)
- Abdominal pain (13.7%)
- Trismus (9.1%)
- Oropharynx may show ulceration, pseudomembrane, or erythema
Important: Symptoms of thrombophlebitis and septic emboli can mask the initial oropharyngeal symptoms, leading to delayed or missed diagnosis.
Complications (from Septic Emboli)
| System | Complication |
|---|---|
| Lungs (most common) | Septic emboli, pulmonary infiltrates, lung abscess, pleural effusion, empyema |
| Bone & joints | Septic arthritis, osteomyelitis |
| Liver | Liver abscess |
| CNS | Brain abscess, meningitis, cavernous sinus thrombosis |
Diagnostic Criteria (all 4 = strong evidence)
- Anaerobic primary infection of the oropharynx
- Subsequent septicemia (at least 1 positive blood culture)
- Metastatic infection of 1 or more distant sites
- Thrombophlebitis of the internal jugular vein
Best diagnostic modality: CT scan of the neck with contrast - demonstrates the thrombus in the IJV, perivascular inflammation, and any abscess.
Note: It may take 5-8 days to isolate F. necrophorum in blood cultures due to its fastidious, anaerobic nature - requiring a high index of clinical suspicion.
Treatment
| Modality | Detail |
|---|---|
| Antibiotics (mainstay) | Beta-lactamase-resistant beta-lactam (e.g., amoxicillin-clavulanate, piperacillin-tazobactam), clindamycin, metronidazole, or chloramphenicol. Variable response to 2nd/3rd-gen cephalosporins |
| Duration | Prolonged (typically 3-6 weeks) |
| Surgery | For abscesses not responding to antibiotics; rarely IJV ligation |
| Anticoagulation | Controversial - no controlled studies; used on a case-by-case basis |
Memory Aid
"POST-ANGINAL SEPTICEMIA"
-
Pharyngitis/tonsillitis → Oropharyngeal abscess → Septic IJV thrombosis → Throwing septic emboli to lungs
-
Symptom to Diagnosis: An Evidence-Based Guide, 4th Edition, Chapter on Sore Throat
-
Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, Vol. 1
-
K.J. Lee's Essential Otolaryngology
-
Red Book 2021, Committee on Infectious Diseases
This is a shared conversation. Sign in to Orris to start your own chat.