Tibia bone
Reading File
Finding Sources
Searching Images
tibia bone anatomy
!
unable to open database file
We encountered an error while processing your request. Please try again or reach out to us for help.
Tibia
Reading File
Finding Sources
Searching Images
tibia bone anatomy labeled diagram
Reading File
Reading File
Loading Image
Finding Sources
Searching Images
tibia bone landmarks medial condyle tibial tuberosity shaft anatomy
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Now I have excellent textbook content and diagrams. Here is a comprehensive overview of the tibia:
The Tibia
The tibia is the medial and larger of the two bones of the leg (the other being the fibula). It is the primary weight-bearing bone of the leg, transmitting forces from the knee to the ankle.
Overview
| Feature | Detail |
|---|---|
| Type | Long bone |
| Location | Medial leg, between knee and ankle |
| Weight-bearing | Yes (primary) |
| Articulations | Femur (knee), fibula (proximal & distal), talus (ankle) |
Proximal End
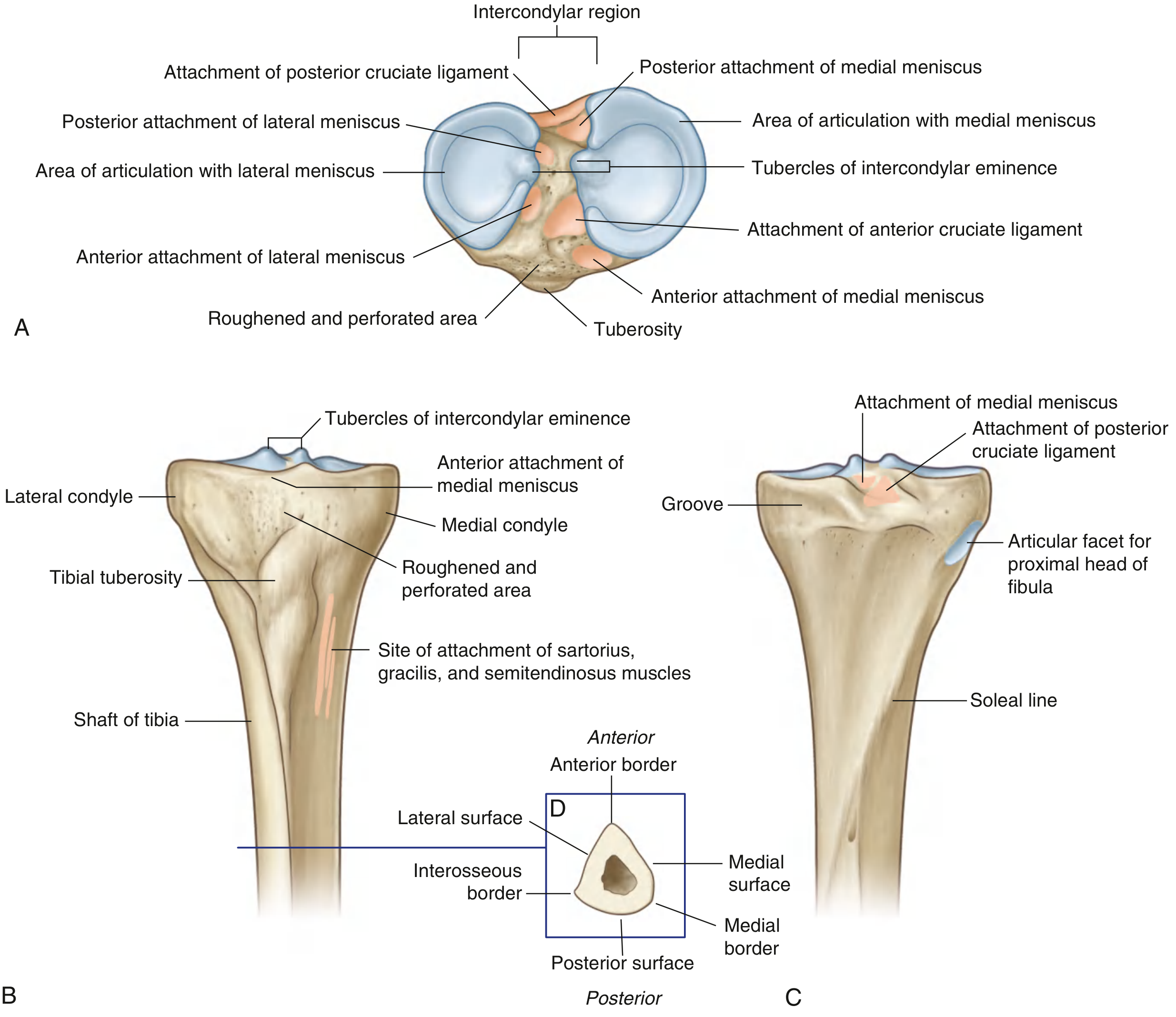
The proximal end is expanded in the transverse plane for weight-bearing and consists of:
Medial and Lateral Condyles (Tibial Plateau)
- The medial condyle is larger, oval in shape, and better supported over the shaft.
- The lateral condyle is smaller and circular; its undersurface has a circular facet for articulation with the head of the fibula (proximal tibiofibular joint).
- Both condyles are concave superiorly, particularly centrally — the outer margins contact the menisci.
- Together they form the tibial plateau, which articulates with the distal femur at the knee joint.
Intercondylar Region
Between the two articular surfaces lies the intercondylar eminence with medial and lateral intercondylar tubercles. This non-articular region bears six attachment facets for:
- Anterior horn of medial meniscus
- Anterior cruciate ligament (ACL)
- Anterior horn of lateral meniscus
- Posterior horn of lateral meniscus
- Posterior horn of medial meniscus
- Posterior cruciate ligament (PCL)
Tibial Tuberosity
- Palpable inverted triangular elevation on the anterior aspect below the condyle junction.
- Site of attachment of the patellar ligament (continuation of the quadriceps femoris tendon below the patella).
Shaft
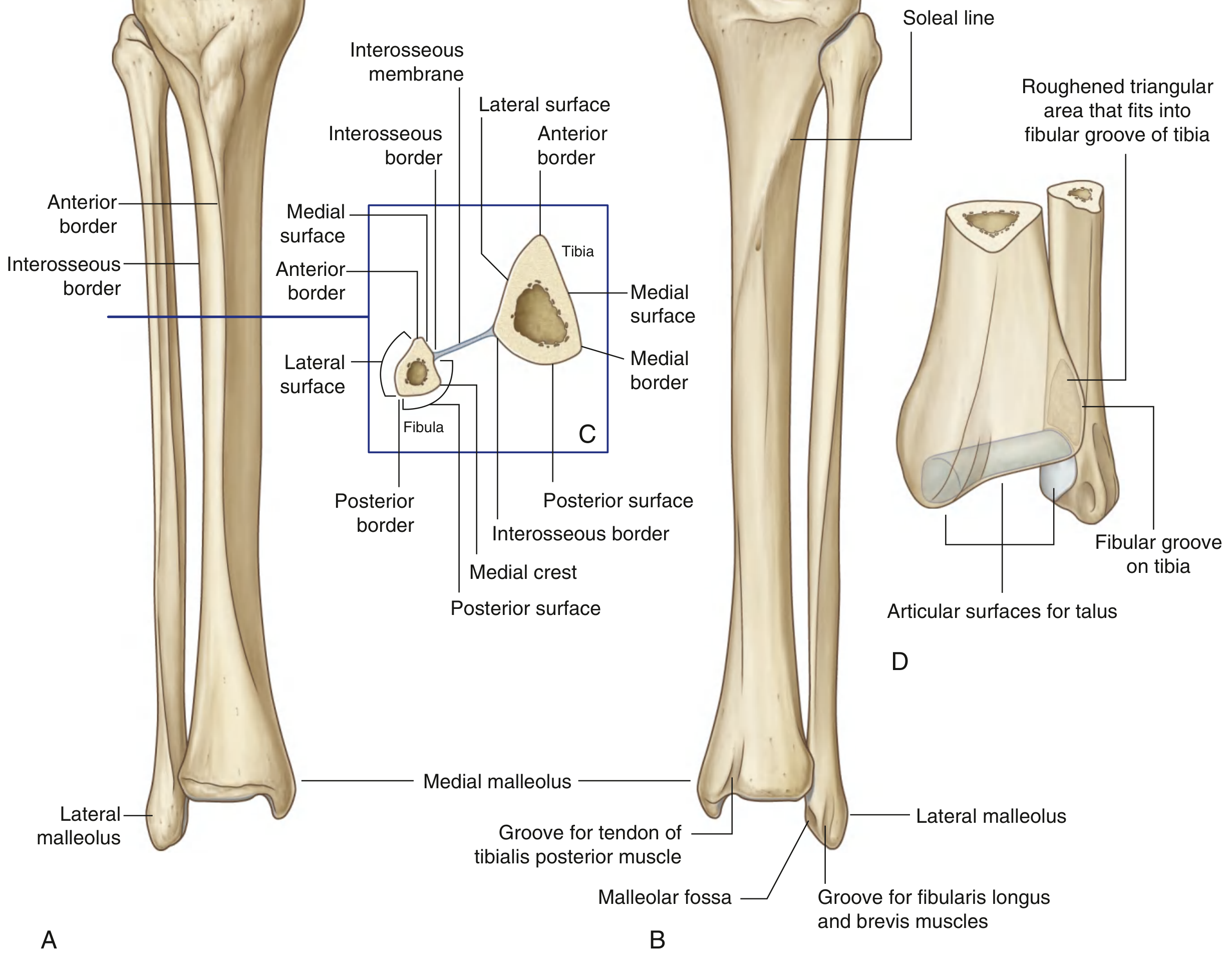
The shaft is triangular in cross section and has:
Three Borders
| Border | Notes |
|---|---|
| Anterior border | Sharp; descends from tibial tuberosity; subcutaneous and palpable ("shin") |
| Interosseous border | Vertical ridge on lateral aspect; connected to fibula by the interosseous membrane |
| Medial border | Indistinct superiorly, sharp at midshaft |
Three Surfaces
| Surface | Notes |
|---|---|
| Medial surface | Smooth, subcutaneous, palpable throughout; bears the pes anserinus attachment (sartorius, gracilis, semitendinosus) |
| Lateral surface | Smooth; between anterior and interosseous borders |
| Posterior surface | Marked by the oblique soleal line (origin of soleus muscle); a vertical line descends from its midpoint in the upper shaft |
Distal End
The distal end is shaped like a rectangular box with a bony protuberance on the medial side:
- Medial malleolus — the medial protuberance; articulates with the talus to form part of the ankle mortise.
- Inferior surface — the tibial plafond; flat articular surface for the body of the talus.
- Posterior surface — bears a groove for the tendon of the tibialis posterior muscle.
- Fibular notch — a deep triangular notch on the lateral surface anchoring the distal fibula via thickened interosseous membrane (inferior tibiofibular syndesmosis).
Key Articulations
| Joint | Bones | Type |
|---|---|---|
| Knee | Tibia + femur | Synovial, condylar |
| Proximal tibiofibular | Tibia + fibular head | Synovial, plane |
| Distal tibiofibular | Tibia + fibular distal end | Fibrous (syndesmosis) |
| Ankle (talocrural) | Tibia + fibula + talus | Synovial, hinge |
Clinically Important Points
- The anterior border and medial surface are entirely subcutaneous — vulnerable to direct trauma and common sites for stress fractures and shin splints (medial tibial stress syndrome).
- The tibia is the most common site for intraosseous (IO) access in emergencies, accessed at the proximal tibia (anteromedial surface, ~2 cm below the tibial tuberosity) or the distal tibia (medial malleolus).
- Tibial plateau fractures result from axial loading + valgus/varus forces (e.g., bumper fractures); the lateral plateau is more commonly involved.
- Tibial shaft fractures are the most common long bone fractures; at risk for compartment syndrome due to tight fascial compartments.
- The soleal line on the posterior tibia marks the origin of the soleus and the lower border of the popliteus insertion.
Sources: Gray's Anatomy for Students; Miller's Review of Orthopaedics 9th Edition; Rockwood and Green's Fractures in Adults 10th ed.
Patella
Finding Sources
Searching Images
patella bone anatomy labeled diagram anterior posterior
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive content for a thorough response on the patella.
The Patella
The patella (kneecap) is the largest sesamoid bone in the body, formed within the tendon of the quadriceps femoris muscle as it crosses the anterior aspect of the knee joint to insert on the tibia.
Anatomy
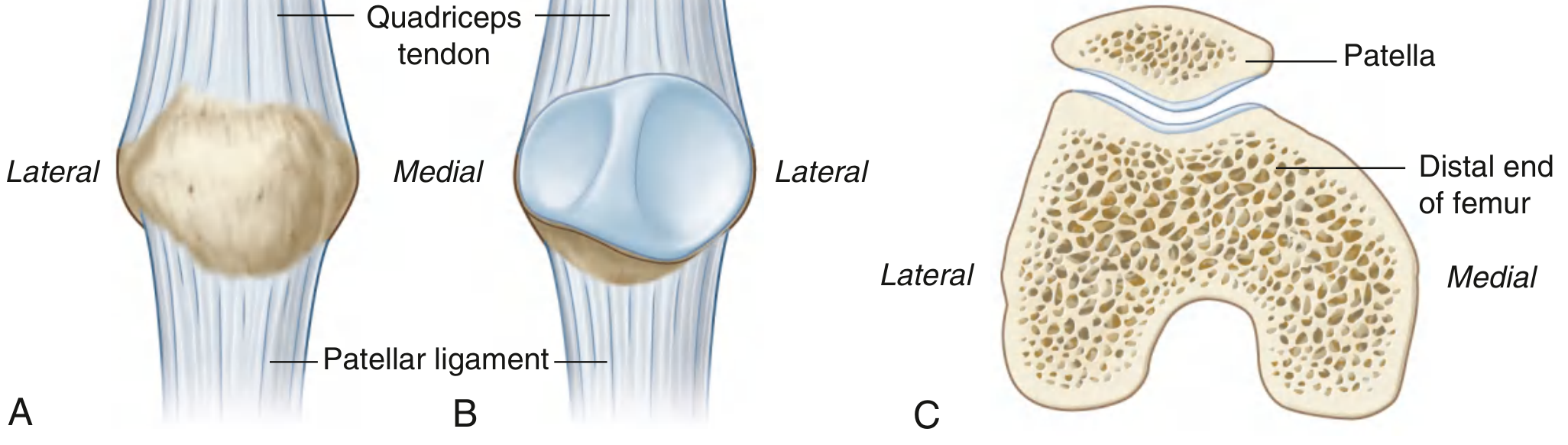
Shape
The patella is triangular in shape with:
| Feature | Details |
|---|---|
| Base | Broad, thick superior border — attachment of the quadriceps tendon |
| Apex | Pointed inferior end — attachment of the patellar ligament (to tibial tuberosity) |
| Anterior surface | Convex, rough, subcutaneous; covered by the prepatellar bursa |
| Posterior surface | Articular; divided by a smooth vertical ridge into medial and lateral facets |
Posterior (Articular) Surface
- The lateral facet is larger than the medial facet, corresponding to the larger lateral femoral condyle.
- Both facets articulate with the trochlear groove (sulcus) of the femur — the patellofemoral joint.
- The lower one-quarter of the posterior surface is non-articular (occupied by the infrapatellar fat pad and patellar tendon attachment).
The Extensor Mechanism
The patella is a central component of the extensor mechanism of the knee, which includes:
- Quadriceps muscles (rectus femoris, vastus medialis, vastus lateralis, vastus intermedius)
- Quadriceps tendon
- Patella
- Patellar ligament (tendon)
- Medial and lateral patellar retinacula
- Tibial tuberosity
Function of the Patella
- Acts as a mechanical pulley: provides anterior displacement of the quadriceps tendon, thereby increasing the lever arm and mechanical advantage of the quadriceps by ~30–50%.
- Protects the knee joint anteriorly.
- Improves the efficiency of knee extension, especially in the last 15–20° of extension.
Patellofemoral Joint & Stability
The patella sits in the trochlear groove of the femur and is stabilized by:
- Medial patellofemoral ligament (MPFL) — the primary static restraint against lateral dislocation; a thickening of the medial retinaculum.
- Lateral retinaculum
- Quadriceps pull — a net lateral vector (due to the Q-angle); the vastus medialis oblique (VMO) provides the primary medial counterbalance.
Patellar Height (Insall-Salvati Ratio)
- Ratio of patellar tendon length : patella length; normally ~1.0
- Patella alta (high-riding patella): ratio >1.5 → predisposes to patellar maltracking and lateral dislocation
- Patella baja (low-riding patella): ratio <0.8 → may occur after tibial tubercle osteotomy or quadriceps shortening
TT-TG Distance
- Tibial tubercle–trochlear groove (TT-TG) distance, measured on CT or axial MRI.
- Normal <15 mm; >18–20 mm indicates excessive lateralization → predisposes to lateral dislocation.
Bursae Around the Patella
| Bursa | Location | Clinical significance |
|---|---|---|
| Prepatellar bursa | Between patella and skin | "Housemaid's knee" (prepatellar bursitis) |
| Suprapatellar bursa | Extension of knee joint cavity | Expands with knee effusion |
| Deep infrapatellar bursa | Between patellar tendon and tibia | "Clergyman's knee" |
| Superficial infrapatellar bursa | Between tibial tuberosity and skin | Overuse bursitis |
Ossification
- The patella is cartilaginous at birth and begins to ossify around 3–5 years of age.
- Bipartite patella: failure of complete fusion of an accessory ossification center (most commonly the superolateral corner); present in ~1–2% of the population; typically bilateral; distinguished from fracture by smooth, rounded cortical margins.
Clinically Important Conditions
Patellar Fractures
- Account for ~1% of all skeletal fractures.
- Mechanisms: direct blow (dashboard, fall onto knee) → comminuted/stellate; indirect (forceful quadriceps contraction) → transverse.
- Types (most common → least): Transverse > stellate/comminuted > avulsion (pole fractures).
- Key assessment: integrity of extensor mechanism — test with straight-leg raise against gravity.
- Nonoperative management: intact extensor mechanism + <2 mm step-off + <3 mm displacement → hinged knee brace in extension.
- Operative management: displaced fractures or disrupted extensor mechanism → ORIF (tension band wiring or screws).
Patellar Dislocation
- Almost always lateral (due to lateral quadriceps pull vector).
- Usually transient — most have relocated by time of presentation.
- MRI findings: "kissing contusions" — bone marrow edema of the medial patella + lateral femoral condyle; tear of MPFL; possible osteochondral fracture.
- Trochlear dysplasia (shallow sulcus) is a major predisposing factor.
Chondromalacia Patellae
- Softening and degeneration of the patellar articular cartilage.
- Common in young active individuals; presents as anterior knee pain worse with stairs, squatting, and prolonged sitting ("theatre sign").
Patellar Tendinopathy ("Jumper's Knee")
- Focal thickening of the central deep portion of the proximal patellar tendon at its attachment to the inferior pole.
- Associated with high jumping, basketball, and volleyball.
- MRI/US shows hypoechoic signal, focal thickening, and increased vascularity.
Sources: Gray's Anatomy for Students; Rosen's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Tintinalli's Emergency Medicine; Rockwood and Green's Fractures in Adults 10th ed.
This is a shared conversation. Sign in to Orris to start your own chat.