Thyroid examination
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the material needed for a complete, well-structured answer. Here it is:
Thyroid Examination
A thorough thyroid examination covers inspection, palpation, percussion, auscultation, and a search for systemic signs of thyroid dysfunction.
1. General Approach
The examination has two components:
- The thyroid gland itself - size, shape, consistency, nodularity, mobility
- Systemic signs - evidence of hypo- or hyperthyroidism, plus extrathyroidal features (e.g. Graves' ophthalmopathy, dermopathy)
Ask the patient about symptoms of compression (dysphagia, hoarseness, stridor) and symptoms of dysfunction (heat/cold intolerance, weight change, palpitations, bowel changes).
2. Positioning
- Patient seated, neck slightly flexed to relax the strap muscles
- Examiner stands behind or in front, using both approaches when nodules are small
3. Inspection
Stand in front of the patient and inspect in good light.
- Look for surgical scars, obvious masses, or distended neck veins
- Ask the patient to swallow a sip of water and observe - the thyroid (and any thyroid mass) rises with swallowing, distinguishing it from non-thyroid neck masses
- A midline mass that rises on tongue protrusion suggests a thyroglossal duct cyst, not true thyroid tissue
- Look for tracheal deviation (suggests large/asymmetric goiter)
4. Palpation
Use both the posterior and anterior approaches - switch between them especially when looking for small nodules.
Posterior approach (preferred):
- Stand behind the patient
- Place fingertips of both hands along either side of the trachea
- Locate the cricoid cartilage first - the thyroid isthmus attaches to the lower one-third of the thyroid lobes just below it
- Follow the isthmus laterally to locate each lobe
- The right lobe is normally slightly larger than the left
Anterior approach:
- Face the patient
- Use both thumbs to palpate each lobe alternately
During palpation, ask the patient to swallow sips of water - the gland moves upward beneath the fingers, making its borders easier to define and consistency easier to appreciate.
Assess and document:
| Feature | What to note |
|---|---|
| Size | Normal is 12-20 g. A lateral lobe larger than the patient's own thumb = goiter. Total thyroid volume >30 mL on ultrasound is abnormal. |
| Consistency | Soft (normal/colloid), firm (Hashimoto's), hard/stony (malignancy, Riedel's) |
| Surface | Smooth (diffuse goiter, Graves') vs. nodular (MNG) |
| Nodularity | Solitary vs. multiple; size, borders, mobility of each nodule |
| Tenderness | Present in thyroiditis (De Quervain's), absent in most other conditions |
| Fixation | A fixed, hard gland suggests malignancy or Riedel's thyroiditis |
Check for substernal extension by palpating the sternal notch and lower borders of each lobe - if the inferior borders are not felt, suspect a retrosternal goiter. A drawing is often the best way to record findings.
5. Pemberton's Sign
Raise the patient's arms above the head and hold for 1 minute.
A positive Pemberton's sign = facial flushing, cyanosis, and venous distention of neck veins due to jugular venous obstruction as the thyroid (or substernal goiter) is drawn into the thoracic inlet. This indicates significant mediastinal compression.
6. Auscultation
Place the bell of the stethoscope over each lobe.
- A thyroid bruit (continuous systolic or systolic-diastolic murmur directly over the gland) indicates increased vascularity - classic in Graves' disease
- Distinguish from a carotid bruit (heard higher up and does not disappear with light pressure over the gland) or a venous hum (disappears on gentle compression of the jugular vein)
7. Percussion
Percuss down from the clavicle along the sternum - dullness to percussion extending below the sternal notch suggests a retrosternal goiter.
8. Systemic Examination for Thyroid Dysfunction
Signs of Hyperthyroidism / Thyrotoxicosis
| System | Signs |
|---|---|
| General | Weight loss despite good appetite, heat intolerance, diaphoresis |
| Skin/hair | Warm, moist, fine skin; fine hair; onycholysis (Plummer's nails) |
| Eyes | Lid retraction, lid lag (von Graefe's sign), exophthalmos/proptosis (Graves') |
| CVS | Tachycardia (resting), atrial fibrillation, bounding pulse, wide pulse pressure, systolic hypertension, cardiac failure in severe cases |
| Neurological | Fine tremor of outstretched hands, hyperreflexia, proximal myopathy |
| GI | Increased bowel frequency |
| Graves' specific | Diffuse goiter with bruit, ophthalmopathy (periorbital edema, chemosis, diplopia), pretibial myxedema (indurated skin plaques on shins), thyroid acropachy (periosteal new bone) |
Signs of Hypothyroidism
| System | Signs |
|---|---|
| General | Weight gain, cold intolerance, fatigue, periorbital puffiness, macroglossia |
| Skin/hair | Dry, coarse skin; non-pitting edema (myxedema); dry/brittle hair; loss of outer third of eyebrows (Queen Anne's sign) |
| CVS | Bradycardia, hypotension, muffled heart sounds (pericardial effusion in severe cases) |
| Neurological | Slow relaxing (hung-up) reflexes, cerebellar signs, carpal tunnel syndrome |
| Voice | Hoarse, croaky voice |
| Thyroid | Usually enlarged (goitrous Hashimoto's) or small/impalpable (atrophic) |
9. Special Signs Summary
| Sign | Elicited by | Indicates |
|---|---|---|
| Pemberton's sign | Arms raised above head | Retrosternal goiter compressing thoracic inlet |
| Thyroid bruit | Auscultation over gland | Graves' disease (high vascularity) |
| von Graefe's sign | Downward gaze - lid lags behind eyeball | Thyrotoxicosis |
| Plummer's nails | Inspection | Thyrotoxicosis (onycholysis) |
| Hung-up reflex | Ankle jerk with slow relaxation | Hypothyroidism |
| Berry's sign | Absent carotid pulsation on palpation | Thyroid malignancy (carotid encasement) |
10. What to Record
After examination, document:
- Location (isthmus, right/left lobe, superior/inferior pole)
- Size (estimate in grams or cm - a diagram is ideal)
- Consistency and surface
- Number and size of any nodules
- Fixation, tenderness, lymph nodes
- Systemic signs of dysfunction
- Any features of obstruction (stridor, dysphagia, Pemberton's sign)
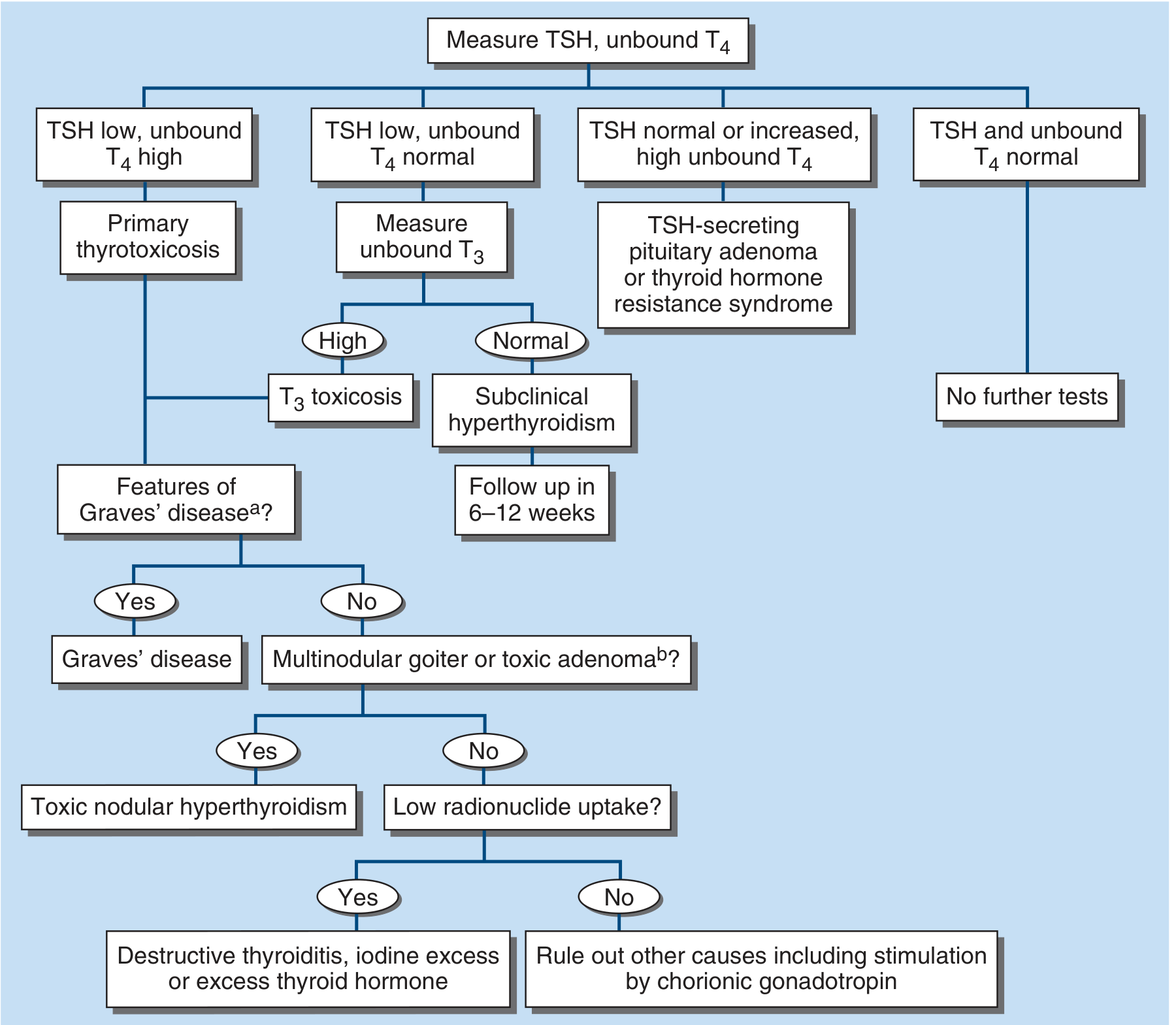
Evaluation Algorithm After Examination
If thyroid enlargement or dysfunction is suspected on examination, investigations begin with TSH and unbound T4:
- Ultrasound provides the most accurate thyroid volume measurement and is the best way to characterize nodules
- Ultrasound is not indicated if the physical examination is entirely normal
- Substernal goiter evaluation requires respiratory flow measurements plus CT or MRI
Sources: Harrison's Principles of Internal Medicine 22E, 2025 (Physical Examination of the Thyroid; Goiter and Thyroid Nodular Disease) | Current Surgical Therapy 14e | Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.