Mean arterial pressure
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Here is a thorough overview of Mean Arterial Pressure (MAP):
Mean Arterial Pressure (MAP)
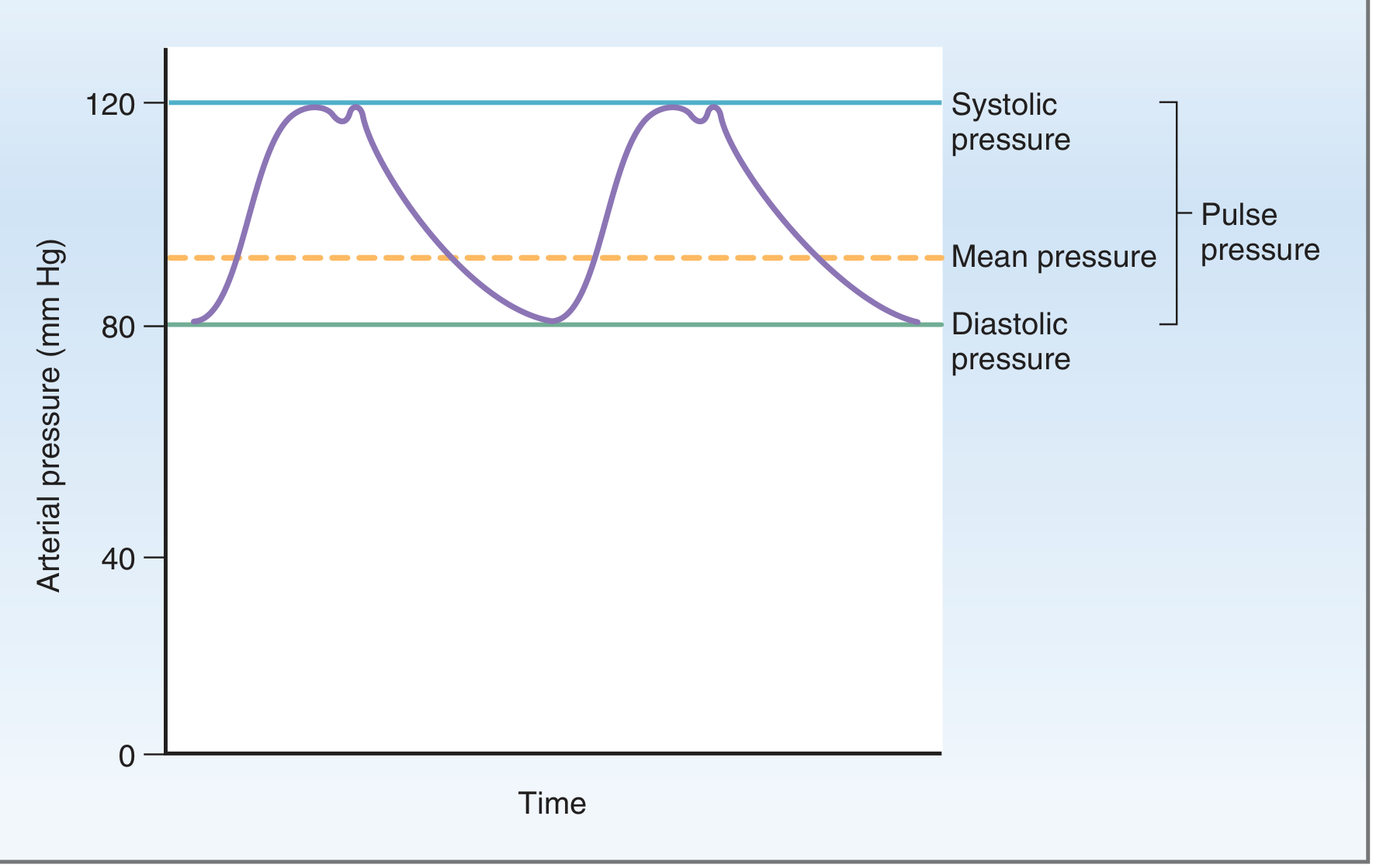
Fig. 4.9 - Costanzo Physiology, 7th Edition: Systemic arterial pressure during the cardiac cycle. Note that mean arterial pressure (dashed orange line) sits closer to diastole than to systole.
Definition
MAP is the average arterial pressure throughout one complete cardiac cycle. It represents the true perfusion pressure delivered to tissues and organs.
Formula
MAP = Diastolic Pressure + 1/3 (Pulse Pressure)
Where Pulse Pressure = Systolic - Diastolic
Equivalently:
MAP = (SBP + 2 × DBP) / 3
Example (BP = 120/80 mmHg):
- Pulse pressure = 120 - 80 = 40 mmHg
- MAP = 80 + 1/3(40) = 80 + 13.3 = ~93 mmHg
Why not a simple average? Because more time is spent in diastole than systole during each cardiac cycle - so diastolic pressure is weighted more heavily. This is why the MAP sits closer to diastole, not exactly midway between SBP and DBP. - Costanzo Physiology, 7th Edition, p. 135
Normal Values
| Parameter | Normal Value |
|---|---|
| MAP | ~70-100 mmHg |
| Critical minimum (organ perfusion) | ≥65 mmHg (often cited as target in shock) |
Why MAP is the Principal Controlled Variable
The cardiovascular system prioritizes MAP above all other variables because:
- All organs receive the same MAP - the branched arterial network delivers to each organ a pressure approximating mean aortic pressure, regardless of how close or distant they are from the heart.
- Local autoregulation depends on it - each organ independently controls its own blood flow by varying local arteriolar resistance, but this only works if MAP is maintained.
- Minimum pressure requirements - MAP must stay high enough to drive glomerular filtration in the kidneys and overcome elevated tissue pressures in organs like the eye.
The analogy is a city water tower: a constant pressure head allows every "house" (organ) to take what it needs by opening or closing faucets (arterioles), without affecting others. - Medical Physiology (Boron & Boulpaep), p. 779
Determinants of MAP
From Ohm's Law applied to circulation:
MAP = Cardiac Output (CO) × Systemic Vascular Resistance (SVR)
So MAP rises when:
- CO increases (higher heart rate or stroke volume)
- SVR increases (vasoconstriction)
And falls when either decreases.
Regulation of MAP
Short-term (seconds to minutes) - Neural:
- Baroreceptors at the carotid sinus and aortic arch are stretch receptors that detect changes in arterial wall tension
- They send afferent signals to the medullary control centers via cranial nerves IX (carotid sinus nerve) and X (vagus/aortic arch)
- The medulla adjusts heart rate, stroke volume, and vascular tone via sympathetic and parasympathetic efferents
- Chemoreceptors are secondary sensors that respond to changes in PO2, PCO2, and pH
Long-term (hours to days) - Renal:
- The kidneys regulate MAP by controlling extracellular fluid (ECF) volume
- Changes in ECF volume alter plasma volume, which alters venous return and ultimately MAP
- The key sensor is "effective circulating volume" (not a literal volume, but the functional perfusion sensed by stretch receptors in low- and high-pressure vessels)
- Hormonal mediators include RAAS (angiotensin II, aldosterone), ANP, and ADH
Clinical Relevance
| Scenario | MAP target |
|---|---|
| Septic shock | ≥65 mmHg (surviving sepsis guidelines) |
| Traumatic brain injury | ≥80 mmHg (to maintain cerebral perfusion) |
| Post-cardiac arrest (TTM) | Often ≥65 mmHg |
Effect of pathology on pulse pressure and MAP:
- Arteriosclerosis: decreased arterial compliance → higher systolic, higher pulse pressure, elevated MAP
- Aortic stenosis: reduced stroke volume → lower systolic, lower pulse pressure, reduced MAP
- Aortic regurgitation: retrograde diastolic flow → very high systolic + very low diastolic = wide pulse pressure, MAP often normal or mildly elevated
MAP in Anesthesia
MAP = Pump flow (CO) × SVR is the core equation guiding hemodynamic management. Inhalational agents, neuraxial blockade, and vasodilating drugs all reduce MAP primarily through SVR reduction, while positive chronotropes/inotropes raise MAP via CO. - Morgan & Mikhail's Clinical Anesthesiology, 7e
Sources:
- Costanzo Physiology, 7th Edition, pp. 134-135
- Medical Physiology (Boron & Boulpaep), pp. 779-782, 812
- Morgan & Mikhail's Clinical Anesthesiology, 7e
This is a shared conversation. Sign in to Orris to start your own chat.