Teach me Forensics Traumatology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
forensic traumatology types of wounds injuries classification forensic medicine
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9802595
Reading File
Searching the Web
forensic traumatology vital reaction antemortem postmortem gunshot wounds firearm injuries forensic pathology
Loading Image
Loading Image
Loading Image
I now have comprehensive material. Let me compile the complete lesson on Forensic Traumatology.
Forensic Traumatology - Complete Lesson
Forensic traumatology is the branch of forensic medicine that studies injuries (wounds, trauma) from a medico-legal perspective - not just to treat the patient, but to reconstruct what happened, who did it, when, and with what. It bridges clinical medicine, pathology, and the justice system.
1. Core Definitions
| Term | Definition |
|---|---|
| Injury | Any harm illegally caused to a person in body, mind, reputation, or property (Section 44, IPC) |
| Wound | Any breach in the natural continuity of tissues of a living body |
| Trauma | Any physical or psychological injury |
| Vital reaction | The body's living response to injury - bleeding, inflammation, clotting. Proves injury was inflicted while the person was alive (antemortem) |
The key forensic question is always: Was this injury inflicted before or after death?
2. Classification of Injuries
A. By Causative Agent
1. Mechanical Injuries (most common in forensic practice)
- Blunt force: Abrasions, Contusions, Lacerations, Fractures, Dislocations
- Sharp force (sharp-edged): Incised wounds, Chop wounds
- Piercing/sharp-pointed: Stab wounds
- Firearm injuries: Gunshot wounds (entry/exit)
2. Thermal Injuries
- Heat: Burns (partial and full thickness)
- Cold: Frostbite, hypothermia
3. Chemical Injuries
- Corrosive agents (strong acids/alkalis): true corrosion
- Irritant agents (weak): inflammation without destruction
4. Miscellaneous
- Electrical injuries
- Lightning strikes
- Radiation injuries
B. Medico-Legal Classification
| Type | Description |
|---|---|
| Suicidal | Self-inflicted with intent to die; accessible locations, hesitation marks often present |
| Homicidal | Inflicted by another person; defense wounds often present |
| Accidental | No intent; may mimic either of the above |
| Defense wounds | Injuries on palms, dorsal forearms from warding off an attacker |
| Fabricated (Self-inflicted) | Simulated injuries; accessible areas only; superficial, parallel cuts |
C. Legal Classification
| Type | Criteria |
|---|---|
| Simple wound | Heals within 20 days; no permanent defect |
| Dangerous wound | Takes >20 days or causes permanent impairment of function |
| Fatal wound | Directly causes death |
3. Blunt Force Injuries (The Big Four)
3.1 Abrasion
An abrasion is a wound produced by scraping or rubbing the skin surface, removing only the epidermal layer.
Types:
- Scratch abrasion - linear, fingernail or thorn
- Graze/Friction abrasion - tangential scraping (road rash)
- Pressure/Impact abrasion - perpendicular impact imprints the pattern of the object
- Patterned abrasion - the object's texture is reproduced on the skin (forensically valuable - can identify the weapon)
Forensic value:
- Indicates direction of force (the "tail" of scraped epidermis points away from the direction of travel)
- Patterned abrasions can physically link a weapon to a victim
- Can preserve trace evidence (fibers, grit, paint)
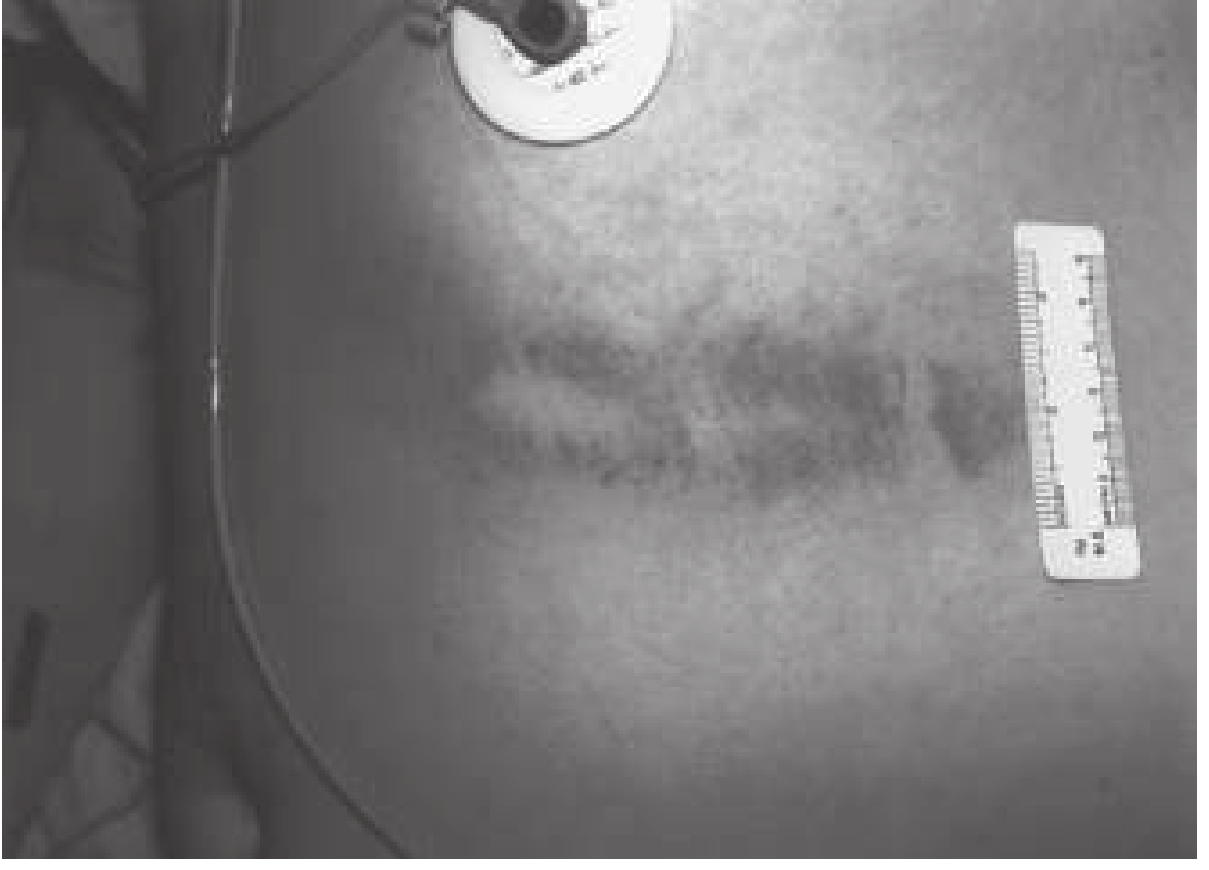
3.2 Contusion (Bruise)
A contusion is damage to blood vessels with extravasation of blood into tissues, caused by blunt trauma.
Forensic value:
- Pattern contusions can identify the weapon and link it to the assailant
- Circular contusions from fingertip pressure indicate grasping/assault
- Important caveat: The color of a bruise CANNOT reliably date when it occurred. Development depends on force applied, tissue vascularity, skin tone, hemoglobin oxygenation, and depth - no reproducible standard exists.
- A bruise may "migrate" superficially over hours to days and appear far from the original impact site
Factors that affect bruise appearance:
- Deep bruises may not appear on the skin surface for 24-72 hours
- Blood may track along fascial planes, appearing distant from the impact
- Age, medications (anticoagulants), and skin tone all affect visibility
3.3 Laceration
A laceration is a tear in the skin and subcutaneous tissue produced by blunt force - NOT to be confused with a cut (incised wound).

Characteristic features:
- Ragged, irregular margins
- Bruised/abraded edges
- Tissue bridges crossing the wound base (intact nerve/vessel strands - hallmark feature)
- Crushed hair follicles
- Gaping of edges
Types of Lacerations:
| Type | Mechanism |
|---|---|
| Split laceration | Blunt object over a bony surface (scalp, shin) - looks deceptively incised |
| Stretch/Tear laceration | Tearing force stretches skin to breaking point |
| Crush laceration | Compressive force; may cause amputation |
| Avulsion laceration | Rotary/grinding force degloving the skin |
Critical clinical-forensic distinction: Lacerations have abraded edges + tissue bridges. Incised wounds have clean, sharp edges. Incorrectly calling a laceration an "incised wound" in a surgical note can undermine the entire prosecution's blunt force theory in court.
- Robbins & Kumar Basic Pathology, p. 284
4. Sharp Force Injuries
4.1 Incised Wound (Cut)
- Length > depth
- Clean, sharp margins - no abrasion, no tissue bridges
- Bleeds freely (no bridging vessels)
- Examples: knife cuts, razor, glass edges
Forensic significance:
- Location and pattern distinguish homicide vs. suicide
- Wounds on neck, chest, and back = assault (hard to self-inflict)
- Wounds only on anterior trunk/forearms with parallel "hesitation marks" = self-inflicted
4.2 Stab Wound
- Depth > width (puncture deeper than it is wide)
- Caused by a pointed instrument
- Clean wound edges
Forensic analysis of stab wounds:
- Number: Multiple stab wounds strongly suggest homicide over accident
- Anatomical location: Wounds over the back, buttocks, or inaccessible areas indicate assault
- Wound dimensions: Suggest blade width
- Shape of wound ends: One blunt end + one sharp end = single-edged blade; two sharp ends = double-edged blade
- Hilt mark: Surrounding bruise/abrasion from hilt impact indicates full blade penetration
- Clothing examination: Can reveal blade type (rounded vs. sharp tip)
4.3 Chop Wound
- Heavy, sharp-edged weapon (axe, machete, cleaver)
- Combines sharp-force AND blunt-force features
- Deeply penetrating; may sever bone
5. Gunshot Wounds (Firearm Injuries)
Gunshot wounds are a special category of puncture wounds. The forensic pathologist must determine four things:
- Trajectory - path of the projectile through the body
- Range of fire - distance from muzzle to target
- Entry vs. exit - distinguishing the two
- Manner of death - homicide, suicide, accident
Entry vs. Exit Wound
| Feature | Entry Wound | Exit Wound |
|---|---|---|
| Margins | Inverted, smooth | Everted, irregular |
| Abrasion collar | Present (characteristic) | Absent |
| Size | Smaller | Larger (usually) |
| Contusion ring | Present | Absent |
| Soot/powder | Present at close range | Absent |
Range of Fire
| Distance | Findings |
|---|---|
| Contact/Hard contact | Muzzle imprint, extensive soot, stellate laceration (gas explosion), cherry-red coloration (CO) |
| Near contact (<1 inch) | Soot deposit, searing |
| Intermediate (<4-5 feet) | Gunpowder stippling (tattooing) |
| Distant (>4-5 feet) | Abrasion collar only - NO soot, NO stippling |
Wound ballistics:
-
Permanent cavity - the direct tissue destruction along the bullet path
-
Temporary cavity - temporary displacement of tissue by pressure wave (more significant with high-velocity rifles)
-
Tissue disruption is directly proportional to mass × velocity² of the projectile
-
Robbins & Kumar Basic Pathology, p. 284
6. Thermal Injuries
Burns are classified by depth:
| Grade | Depth | Features |
|---|---|---|
| Superficial (1st degree) | Epidermis only | Erythema, pain, no blisters |
| Partial thickness (2nd degree) | Epidermis + superficial dermis | Blisters, painful, heals without grafting |
| Full thickness (3rd degree) | Full dermis destroyed | Leathery, insensate (nerve destruction), needs grafting |
Forensic significance of burns:
- Location is key: Burns on the gluteal area/perineum are rarely accidental
- Intentional burns tend to be well-demarcated and deeper
- Children with circumferential "stocking/glove" pattern burns from immersion in hot water = abuse
- Perpetrators sometimes use fire to conceal blunt force injuries postmortem
7. Antemortem vs. Postmortem Injuries - The Vital Reaction
This is perhaps the most important forensic concept in traumatology.
| Feature | Antemortem | Postmortem |
|---|---|---|
| Hemorrhage | Profuse, arterial spouting possible | Minimal or none |
| Blood clotting | Present | Absent (blood stays liquid) |
| Wound edges | Gape open | Stay close together |
| Inflammation | Present (swelling, neutrophil infiltrate) | Absent |
| Serum serotonin/histamine | Elevated | Not elevated |
| Appearance | Red/pink, vital color | Leathery, yellow-brown, dry |
| Vital reaction | Present | Absent |
Key principle: Postmortem injuries or artifacts have a leathery, yellowish appearance with little or no hemorrhage and NO vital reaction. Insect activity can sometimes mimic antemortem abrasions.
Perimortem wounds (near the time of death) are the most difficult to classify - they may show minimal bleeding yet still be antemortem.
Recent research: Tissue leukotriene B4 (LTB4), an inflammatory mediator, is elevated in antemortem wounds and absent in postmortem wounds - a newer biochemical marker to assist classification.
8. Defense Injuries
Defense injuries occur when a victim attempts to ward off an attack.
Blunt force defense injuries: Contusions/fractures on the forearms and hands (raised to block blows)
Sharp force defense injuries: Incised wounds or stab wounds on:
- Dorsal surface of hands and fingers (grabbing the blade)
- Extensor surface of forearms
- Palms (grabbed the blade)
Forensic rule: Defense injuries strongly imply the victim was conscious and mobile during the assault - arguing against a story of "sudden death from behind."
9. Vehicular Accident Injuries
In a head-on collision, a non-belted driver classically sustains the "3-point impact" pattern:
| Structure | Injury |
|---|---|
| Head (windshield) | Scalp lacerations, skull fractures, brain contusions |
| Chest (steering column) | Sternal fractures, rib fractures, cardiac contusion, aortic laceration |
| Knees (dashboard) | Patellar fractures, posterior hip dislocation |
Critical forensic point: External evidence is often absent despite severe internal injury. A victim with only minor superficial abrasions may have a ruptured aorta.
- Robbins & Kumar Basic Pathology, p. 284
10. Documentation - The Forensic Imperative
A clinician treating a trauma patient is also, potentially, a forensic witness. Best practices:
- Describe, don't diagnose: Write "a 3 cm wound with irregular, abraded margins and tissue bridging" - NOT simply "a cut"
- Photograph with a scale ruler before cleaning
- Document location precisely: Anatomical landmarks, measured distances
- Preserve evidence: Swab bite marks before washing (DNA); bag hands in paper bags for gunshot residue
- Never render opinion on bruise age: Color-based dating is not scientifically valid
- Document clothing: Pattern injuries on clothing can corroborate wound findings
In trauma forensics, a minor wound can have enormous medicolegal importance, while a major trauma injury may have little forensic significance. Severity does not equal forensic relevance.
- PMC9802595 (Trauma Forensics in Blunt and Sharp Force Injuries)
11. Summary Table: Wound Comparison at a Glance
| Feature | Abrasion | Contusion | Laceration | Incised | Stab |
|---|---|---|---|---|---|
| Mechanism | Friction | Blunt | Blunt tear | Sharp | Sharp point |
| Margins | Scraped | Intact skin | Ragged, bruised | Clean, sharp | Clean |
| Depth | Superficial | Subcutaneous | Variable | L > D | D > W |
| Tissue bridges | No | No | Yes (hallmark) | No | No |
| Hemorrhage | Capillary | Subcutaneous | Moderate | Profuse | Variable |
| Weapon clues | Pattern, direction | Pattern, shape | Object surface | Blade length | Blade edge/type |
Key Exam Points
- Tissue bridges = LACERATION (blunt force) - never present in incised wounds
- Incised wound: length > depth; Stab wound: depth > width
- Abrasion collar = entry gunshot wound
- No soot/stippling at distance >4-5 feet from muzzle
- Defense wounds on dorsum of hands/forearms = victim was aware and fighting back
- Color alone cannot date a bruise - this is not scientifically valid
- Vital reaction (inflammation, hemorrhage, clotting) = antemortem injury
- Self-inflicted wounds: accessible locations, hesitation marks, anterior trunk/forearms; no defensive wounds on others
This is a shared conversation. Sign in to Orris to start your own chat.