INR correlation
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
INR coagulation clinical correlation
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of INR correlations with clinical conditions and drugs:
INR (International Normalized Ratio) - Clinical Correlations
What the INR Measures
The INR is the standardized version of the Prothrombin Time (PT). It measures the activity of fibrinogen, prothrombin (factor II), and factors V, VII, and X - all components of the extrinsic coagulation pathway. The normal PT is 11-14 seconds; the normal INR is 0.8-1.2.
The INR was originally designed specifically to monitor warfarin (vitamin K antagonist) therapy - this is a key limitation to keep in mind when interpreting it in other clinical settings. - Morgan and Mikhail's Clinical Anesthesiology, p. 1334
INR Reference Ranges and Correlation with Conditions
| INR | Correlation |
|---|---|
| 0.8-1.2 | Normal (no anticoagulation) |
| 2.0-3.0 | Therapeutic target: most warfarin indications (AF, DVT/PE, bioprosthetic valves) |
| 2.5-3.5 | Therapeutic target: mechanical heart valves |
| > 3.5-4.5 | Supratherapeutic - elevated bleeding risk |
| > 4.5-10 | High bleeding risk; hold warfarin +/- oral vitamin K |
| > 10 | Very high bleeding risk; consider urgent reversal |
- Quick Compendium of Clinical Pathology, pp. 2217-2247
- Harrison's Principles of Internal Medicine 22E, p. 343
Diagnostic Flowchart (PT/INR vs. aPTT)
The pattern of which test is prolonged guides diagnosis:
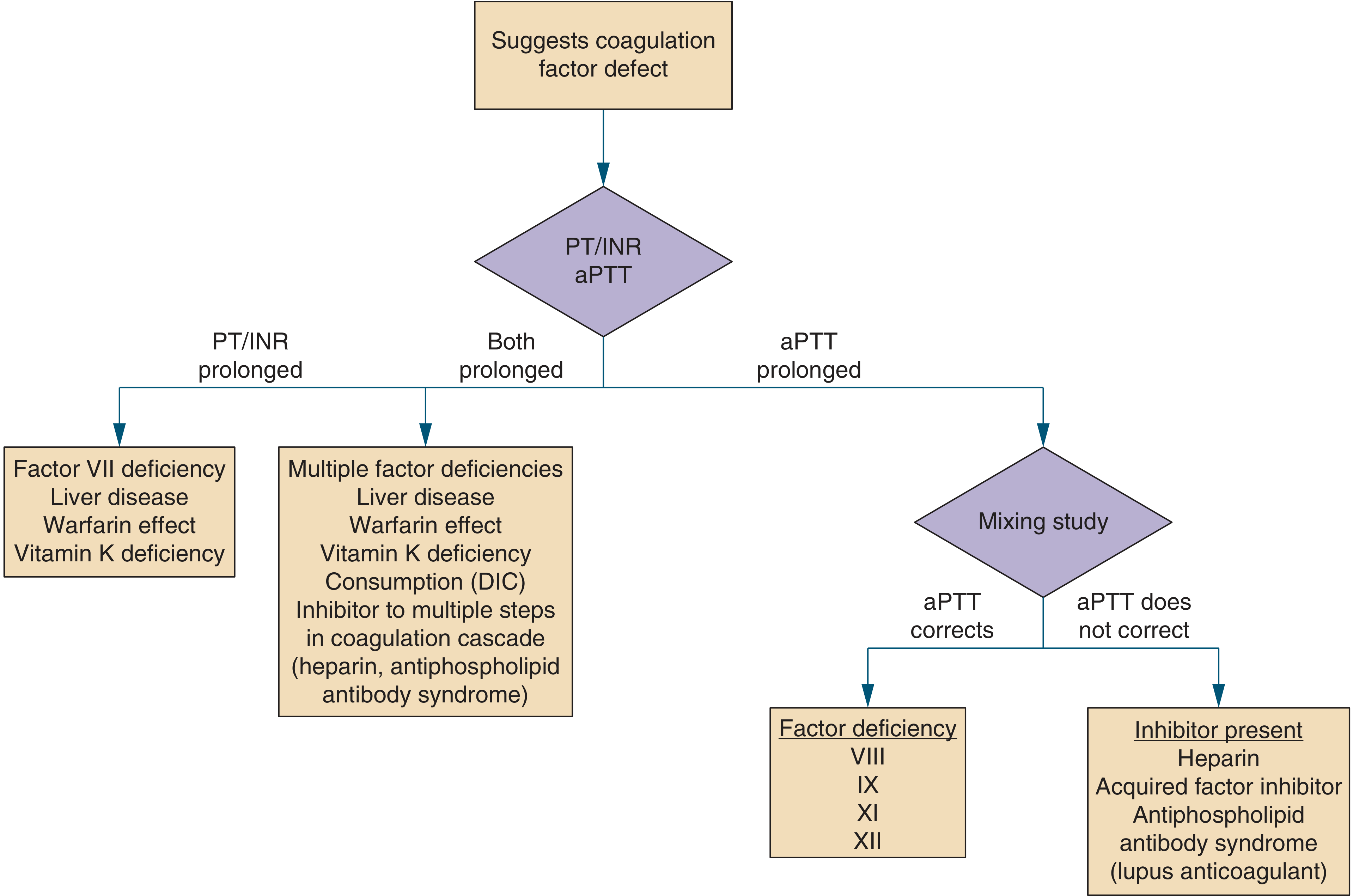
Figure: Diagnostic approach to coagulation factor defects based on PT/INR and aPTT pattern. - Symptom to Diagnosis: An Evidence-Based Guide, 4th ed., Figure 8-1
Key Clinical Correlations
1. Warfarin (Vitamin K Antagonist)
- INR is the primary monitoring tool for warfarin therapy
- Target typically INR 2.0-3.0; takes 3-5 days to reach therapeutic range (heparin bridging recommended)
- Factors affecting INR on warfarin:
- Pharmacogenomics: VKORC1 (encodes the warfarin target, vitamin K epoxide reductase) and CYP2C9 (warfarin metabolism) have the greatest genetic impact
- Diet: vitamin K intake (green leafy vegetables lower INR)
- Comorbidities and drug interactions
- Reversal guidelines (PCC dosing): INR 2-4 → 25 U/kg; INR 4-6 → 35 U/kg; INR >6 → 50 U/kg (max weight 100 kg)
- Asymptomatic supratherapeutic INR (no bleeding): hold warfarin ± oral vitamin K; daily INR monitoring until back in range
2. Liver Disease
- INR (and PT) reflects hepatic synthetic function - a prolonged INR in a non-anticoagulated patient strongly suggests dysfunctional liver - Morgan and Mikhail's, p. 1334
- Coagulopathy seen primarily in severe liver disease (significant hepatic reserve must be lost first)
- Characteristically: INR/PT disproportionately longer than aPTT (because factor VII, with the shortest half-life, is most prominently affected first)
- Important caveat: the INR is NOT calibrated for liver disease - it was validated only for patients on VKA therapy. The ISI (International Sensitivity Index) used to calculate INR does not harmonize across labs for liver disease. This causes interlaboratory variation in MELD scores
- Factor VIII is typically normal or elevated in liver disease (made by endothelial cells, not hepatocytes) - this can help distinguish liver disease from DIC, in which factor VIII is low
- Despite prolonged INR, liver disease creates a rebalanced hemostasis - some patients may actually be hypercoagulable (due to concurrent protein C/S deficiency)
3. Vitamin K Deficiency
- Prolongs PT/INR (and sometimes aPTT) by impairing gamma-carboxylation of factors II, VII, IX, and X
- Pattern: PT/INR disproportionately longer than aPTT (same as liver disease, because factor VII has shortest half-life)
- Key distinguishing point: factor V is normal in pure vitamin K deficiency, whereas both factors V and VII are low in liver disease
- Common causes: malnutrition, prolonged antibiotic use (kills gut flora), malabsorption (fat-soluble vitamin)
- Responds to vitamin K replacement (if INR fails to correct → consider PIVKA-II measurement to confirm)
4. Disseminated Intravascular Coagulation (DIC)
- Both PT/INR and aPTT are prolonged (combined pattern)
- Additional markers: thrombocytopenia, reduced fibrinogen, elevated D-dimer and fibrin degradation products
- Requires an inciting cause: sepsis, major trauma, obstetric crisis, shock
- Factor VIII is LOW (consumed) - helps distinguish from liver disease
5. Isolated Factor VII Deficiency
- Prolonged PT/INR only (aPTT normal) - because factor VII is the only extrinsic pathway factor
- Congenital deficiency is rare; acquired usually from early liver disease or early vitamin K deficiency
INR and Procedural/Invasive Risk
An elevated INR is not an absolute contraindication to most procedures. Multiple studies have shown that select invasive procedures can be performed safely despite laboratory coagulopathy. - Roberts and Hedges' Clinical Procedures in Emergency Medicine
For procedures near the liver, note that hepatic blood flow can drop by up to 60% during surgery, which compounds any existing coagulopathy.
Limitations of INR
- Not calibrated for non-warfarin states - the ISI is validated only for VKA-treated patients; using INR in liver disease or other acquired coagulopathies introduces significant interlaboratory variation - Tietz Textbook of Laboratory Medicine, 7th ed.
- Does not reflect anticoagulant factors (protein C, protein S, antithrombin III) - so a patient with INR of 3 (not on warfarin) may still be in a net procoagulant state if anticoagulant proteins are more depleted than coagulant factors
- DOACs (apixaban, rivaroxaban, etc.) do not use INR for monitoring - these are monitored with anti-Xa assays
Summary Table: PT/INR Pattern by Condition
| Condition | PT/INR | aPTT | Fibrinogen | Platelets | Key distinguisher |
|---|---|---|---|---|---|
| Warfarin | ↑↑ | Normal/↑ | Normal | Normal | On VKA; corrects with vitamin K |
| Liver disease | ↑↑ | Normal/↑ | Normal/↓ | Normal/↓ | Factor VIII normal/elevated |
| Vitamin K deficiency | ↑↑ | Normal/↑ | Normal | Normal | Factor V normal; corrects with vitamin K |
| DIC | ↑ | ↑ | ↓↓ | ↓↓ | D-dimer elevated; inciting cause present |
| Factor VII deficiency | ↑ | Normal | Normal | Normal | Only PT prolonged |
| Heparin | Normal/↑ | ↑↑ | Normal | Normal | Anti-Xa or anti-IIa activity |
| Antiphospholipid Ab syndrome | Normal | ↑ | Normal | Variable | Mixing study does not correct |
This is a shared conversation. Sign in to Orris to start your own chat.