1. A 55-year-old female presented to the surgical OPD with complaints of swelling in the right breast. On examination, the swelling was hard and fixed. Needle biopsy was taken. What is the diagnosis, classify lesion and morphology, and prognostic factor of the lesion? 2. 46-year-old female presented with a left breast mass with nipple retraction and axillary lymphadenopathy. What is the probable diagnosis, etiology, pathogenesis, morphology, and lab diagnosis?
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I now have all the information needed to provide a comprehensive answer for both cases. Let me compile the full response.
Case 1: 55-Year-Old Female with Hard, Fixed Right Breast Swelling
Diagnosis
Invasive Breast Carcinoma of No Special Type (NST) - also called Invasive Ductal Carcinoma (IDC), NOS. This is the most common breast malignancy, accounting for ~75% of all invasive breast carcinomas.
The clinical hallmarks pointing to this diagnosis:
- Hard, fixed swelling (fixation due to invasion into surrounding structures and desmoplastic reaction)
- Postmenopausal age (55 years) - peak incidence for luminal-type breast cancer
- Needle biopsy confirms malignancy histologically
Classification of the Lesion
Breast cancers are classified using two complementary systems:
A. Histological/Morphological Classification (WHO)
| Type | Frequency |
|---|---|
| Invasive carcinoma of no special type (NST/ductal) | ~75% |
| Invasive lobular carcinoma | ~15% |
| Special types (mucinous, tubular, papillary, cribriform, etc.) | ~10% |
B. Molecular/Biomarker Classification (Clinical Groups)
| Molecular Subtype | ER | PR | HER2 | Notes |
|---|---|---|---|---|
| Luminal A | + | + | - | Best prognosis, low grade |
| Luminal B | + | +/- | - or + | Higher proliferation |
| HER2-enriched | - | - | + | Responds to trastuzumab |
| Triple-negative (TNBC) | - | - | - | Worst prognosis |
C. Histologic Grade (Nottingham Score - Bloom-Richardson)
Based on three criteria:
- Tubule formation (glandular differentiation)
- Nuclear pleomorphism
- Mitotic rate
- Grade 1 (well differentiated): tubular/cribriform pattern, small uniform nuclei, low mitoses
- Grade 2 (moderately differentiated): solid clusters, moderate nuclear pleomorphism
- Grade 3 (poorly differentiated): ragged nests/sheets, enlarged irregular nuclei, high mitotic rate, necrosis common
Morphology
Gross appearance:
- Hard, irregular mass (typically 2-3 cm at presentation without screening)
- Irregular margins on imaging and gross examination (Fig. 23.20A, B)
- Chalky-white desmoplastic stroma; produces a characteristic grating sound when cut or scraped
- Occasional foci of calcification
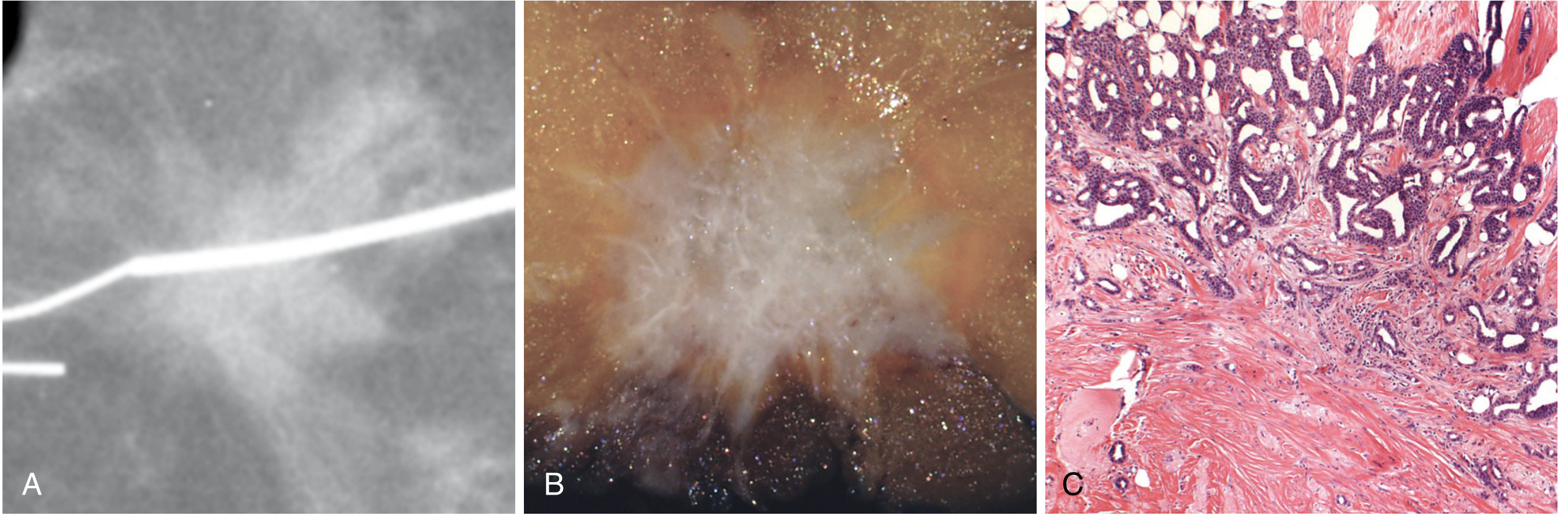
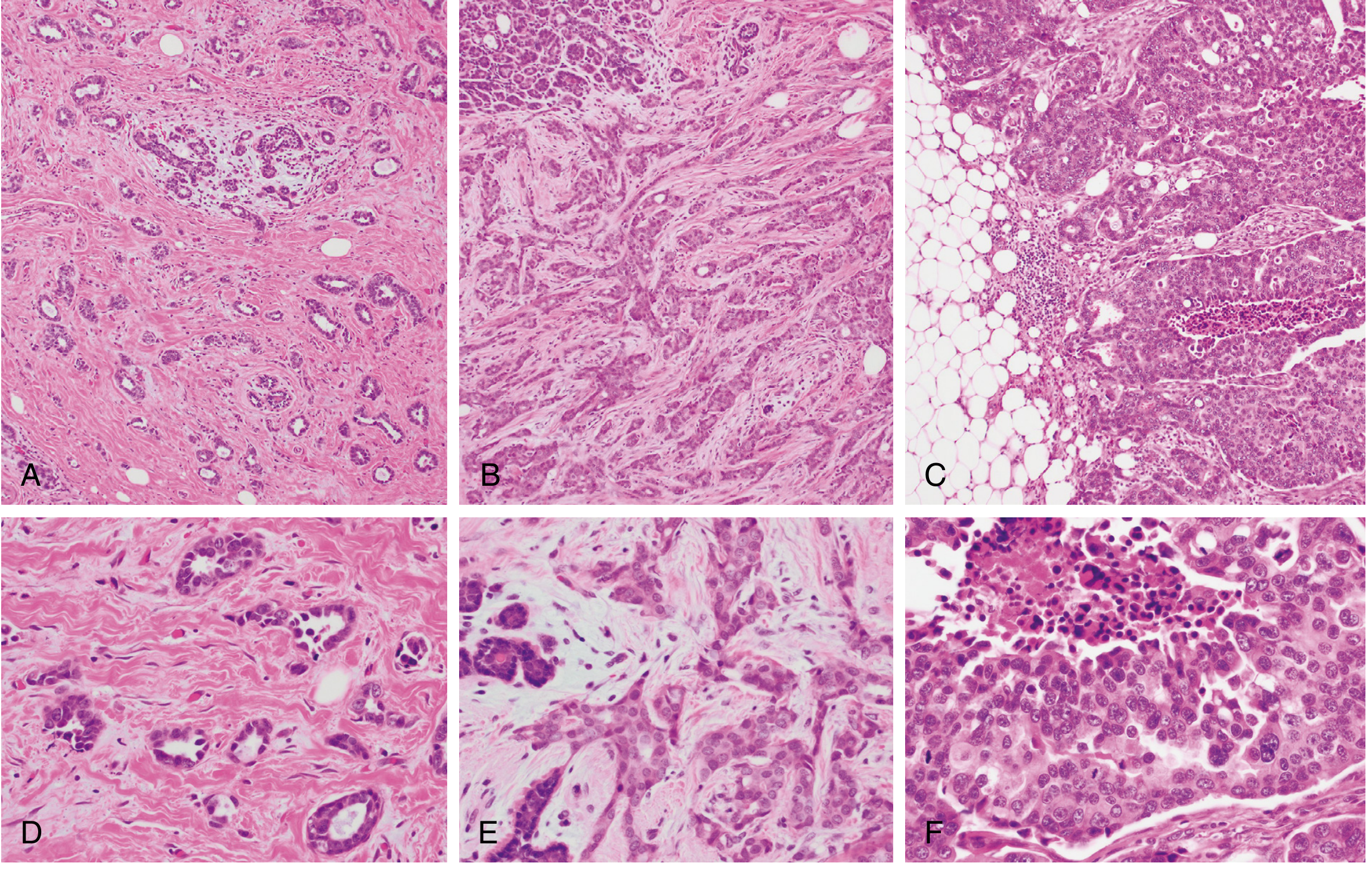
Microscopic appearance:
- Irregular nests, cords, and sheets of malignant epithelial cells invading stroma
- Desmoplastic stromal reaction (key feature)
- Varying degrees of glandular differentiation depending on grade
- Tumor cells with enlarged nuclei, mitoses, and necrosis (in high-grade tumors)
Prognostic Factors
Prognosis depends on biological features + anatomic stage (AJCC 8th edition combines both):
Major Prognostic Factors (Table 23.5)
1. Distant Metastasis (M stage)
- The single most important prognostic factor. Once present, cure is unlikely.
2. Lymph Node Status (N stage)
- Most important factor in the absence of distant metastases
- 10-year disease-free survival: 70-80% with no nodal involvement → drops to 35-40% with 1-3 positive nodes → 10-15% with >10 positive nodes
3. Tumor Size (T stage)
- Node-negative tumors <1 cm: 10-year survival >90%
- Node-negative tumors >2 cm: survival drops to 77%
4. Histologic Grade
- Higher grade = worse prognosis at each stage level
5. ER/PR/HER2 Expression (Biomarker Profile)
- Best prognosis: high ER + high PR + HER2-negative
- Worst prognosis: ER/PR/HER2-negative (triple negative - TNBC)
- HER2 overexpression indicates aggressive behavior but responds to targeted therapy (trastuzumab)
6. Other Prognostic Factors
- Lymphovascular invasion: found in ~50% of invasive carcinomas; poor prognostic factor for recurrence
- Inflammatory carcinoma presentation: 3-year survival only 3-10%
- Tumor-infiltrating lymphocytes (TILs): high TILs = better prognosis in HER2 and TNBC
- Gene expression profiling (Oncotype DX, MammaPrint): identifies patients who can be spared chemotherapy
- Response to neoadjuvant chemotherapy: pathologic complete response (especially in TNBC/HER2) correlates with better survival
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, blocks 10-11
Case 2: 46-Year-Old Female with Left Breast Mass, Nipple Retraction, and Axillary Lymphadenopathy
Probable Diagnosis
Invasive Lobular Carcinoma (ILC) - the second most common invasive breast cancer subtype (~15% of all cases).
The clinical features fit this diagnosis:
- Nipple retraction - occurs when the central breast is involved and tumor invades toward the nipple via Cooper's ligaments
- Axillary lymphadenopathy - regional nodal spread
- ILC typically infiltrates the breast insidiously with minimal desmoplasia, making it difficult to detect on imaging, and may present as diffuse thickening rather than a discrete hard lump
Etiology
ILC arises from lobular epithelial cells of the terminal duct-lobular unit. Key etiological factors:
- CDH1 gene mutation/deletion (chromosome 16q22.1) - the foundational molecular event; CDH1 encodes E-cadherin
- Males and females with heterozygous germline CDH1 mutations are at increased risk for both lobular breast carcinoma and signet ring carcinoma of the stomach
- Most ILCs are ER-positive/HER2-negative (luminal subtype), driven by estrogenic stimulation
- Risk factors overlap with breast cancer generally: nulliparity/delayed childbearing, hormone replacement therapy, increasing age (peak 40s-60s)
- ILC shares the low-grade breast neoplasia pathway genomic alterations, including 16q deletion, with LCIS (its non-invasive precursor)
Pathogenesis
The key molecular event is loss of E-cadherin function:
- E-cadherin is a transmembrane cell adhesion protein expressed by epithelial cells; it acts as a tumor suppressor
- Loss-of-function mutations or deletion of the CDH1 gene → loss of E-cadherin expression
- Rarely, other components of the E-cadherin complex (e.g., beta-catenin) are dysfunctional instead
- Loss of E-cadherin disrupts cell-cell adhesion → dyscohesive tumor cells that cannot form glands or tubules
- These dyscohesive cells infiltrate the stroma individually or in single-file "Indian file" cords
- The lack of desmoplastic reaction explains why ILC is difficult to detect on imaging
- LCIS (lobular carcinoma in situ) represents the precursor in-situ phase; cells are morphologically identical to ILC and also lack E-cadherin
Characteristic metastatic spread (related to pathogenesis):
Due to E-cadherin loss enabling unusual infiltration patterns, ILC metastasizes to uncommon sites: peritoneum, retroperitoneum, leptomeninges (carcinomatous meningitis), gastrointestinal tract, ovaries, and uterus - in addition to standard lymph node and hematogenous routes.
Nipple retraction mechanism:
When the tumor involves the central breast, it invades along Cooper's ligaments toward the overlying skin and nipple. Fibrotic shortening of these ligaments causes skin dimpling and nipple retraction.
Morphology
Gross appearance:
- Often no discrete, well-defined mass - instead a diffuse, rubbery induration or ill-defined thickening
- Minimal desmoplasia (unlike IDC-NST) - hence soft/subtle
- May be almost imperceptible on gross examination
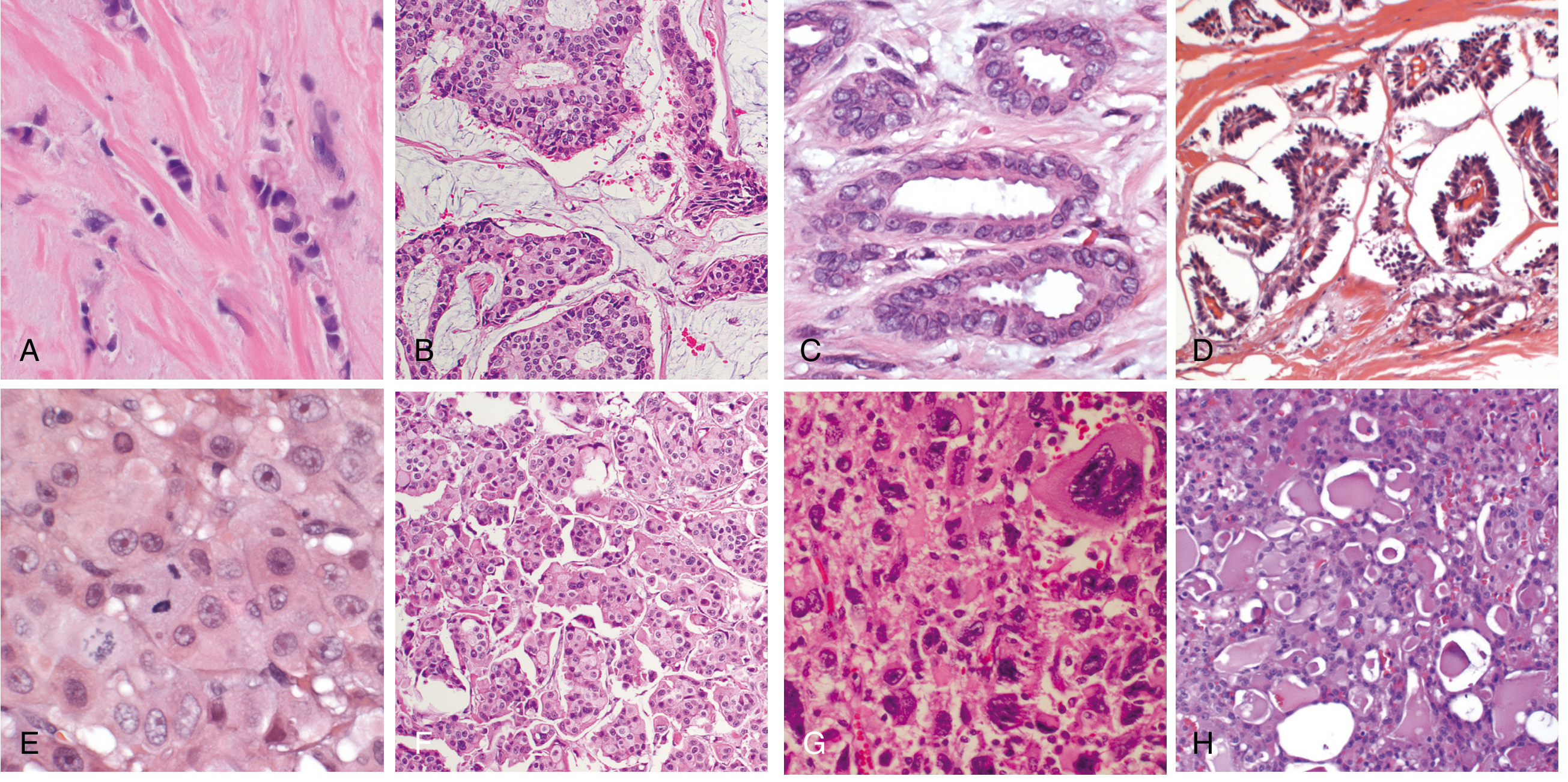
Microscopic appearance (Histologic hallmarks):
- Dyscohesive single infiltrating cells - due to E-cadherin loss
- "Indian file" or single-cell linear cords - the pathognomonic pattern; tumor cells line up in single file through stroma
- Targetoid (concentric) pattern - cells encircle normal ducts and lobules in a bull's-eye pattern
- Signet ring cells - mucin-positive intracytoplasmic vacuoles displacing the nucleus
- Cells are small, uniform, with round-to-oval nuclei and inconspicuous nucleoli
- Absent or minimal desmoplasia
- Almost always ER-positive, HER2-negative
Lab Diagnosis
1. Fine Needle Aspiration Cytology (FNAC) / Core Needle Biopsy
- FNAC: Dyscohesive, small uniform cells; Indian-file arrangement; signet ring cells with intracytoplasmic mucin; absence of tubule formation
- Core needle biopsy (preferred): Histologic sections showing the classic single-file infiltrating pattern; IHC can be performed
2. Immunohistochemistry (IHC) - Key Panel
| Marker | ILC Result | Significance |
|---|---|---|
| E-cadherin | Negative (absent) | Diagnostic - differentiates ILC from IDC (E-cadherin positive in IDC) |
| ER (estrogen receptor) | Positive (~95% of cases) | Prognostic + guides endocrine therapy |
| PR (progesterone receptor) | Usually positive | Prognostic |
| HER2 | Negative (usually) | Prognostic/therapeutic |
| p120-catenin | Cytoplasmic shift | Confirms E-cadherin dysfunction |
E-cadherin loss is the defining diagnostic marker for ILC. In IDC-NST, E-cadherin is retained (membrane positivity).
3. Imaging
- Mammography: May appear as architectural distortion rather than a discrete mass (low sensitivity ~60-70% due to minimal desmoplasia)
- MRI: Superior sensitivity; better characterizes extent of disease
- Ultrasound: May show heterogeneous hypoechoic area with shadowing
4. Additional Investigations
- Tumor markers: CA 15-3, CEA (not diagnostic alone; used for monitoring)
- Sentinel lymph node biopsy/axillary dissection: For staging nodal disease
- Gene expression profiling: Oncotype DX or MammaPrint if ER-positive, node-negative, to guide chemotherapy decision
- Germline CDH1 testing: Consider in cases with family history or signet ring gastric cancer history
5. Histologic Grading
- Most ILCs are Grade 1 or 2 (well-to-moderately differentiated) despite their invasive behavior
- Grade determined by Nottingham Histologic Score
Summary Table:
| Feature | Case 1 (IDC-NST) | Case 2 (ILC) |
|---|---|---|
| Frequency | ~75% of breast cancers | ~15% of breast cancers |
| Gross | Hard, irregular, desmoplastic mass | Diffuse thickening, no discrete mass |
| Microscopy | Irregular nests/cords, desmoplasia | Indian-file cords, dyscohesive cells |
| E-cadherin | Positive | Negative |
| ER status | Variable | Usually positive (~95%) |
| Key mutation | Varied (BRCA1, TP53, PIK3CA) | CDH1 loss |
| Detection | Often palpable hard mass | Subtle, imaging difficult |
| Metastatic pattern | Axillary nodes, bone, lung, liver | + Peritoneum, GI tract, meninges |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528), blocks 10-11; Robbins & Kumar Basic Pathology (9780323790185), block 7
This is a shared conversation. Sign in to Orris to start your own chat.